le petit Robert dit - Chi2 · “le petit Robert ” dit : zSavoir: zAvoir présent à lʼesprit...
32
“ le petit Robert ” dit : ” Savoir: ” Avoir présent à l’esprit (qqch que l’on identifie et que l’on tient pour réel) ” Etre conscient de ” Etre en mesure d’utiliser ” Avoir présent à l’esprit dans tous ses détails ” Souligne une affirmation ” Être capable par apprentissage par habitude de faire qqch, ” s’appliquer à ..par effort de volonté ” Ensemble de connaissances (culture, instructions, science) ” Pouvoir ” Avoir la possibilité de faire qqch ” Avoir le droit, la permission ” Etre capable ” Le fait de pouvoir titel 1 27/10/2016
Transcript of le petit Robert dit - Chi2 · “le petit Robert ” dit : zSavoir: zAvoir présent à lʼesprit...

“ le petit Robert ” dit :
Savoir:Avoir présent à l’esprit (qqch que l’on identifie et que l’on tient pour réel)Etre conscient deEtre en mesure d’utiliserAvoir présent à l’esprit dans tous ses détailsSouligne une affirmationÊtre capable par apprentissage par habitude de faire qqch,s’appliquer à ..par effort de volonté
Ensemble de connaissances (culture, instructions, science)
PouvoirAvoir la possibilité de faire qqchAvoir le droit, la permissionEtre capableLe fait de pouvoir
titel1 27/10/2016
Savoir et pouvoir: en pratique
Savoir: pouvoir dans le sens d’avoir appriscomment (Savoir→Pouvoir)
Pouvoir: verbe qu’on “sait” parfois remplacerpar savoir (Savoir Pouvoir)
titel2 27/10/2016
titel3 27/10/2016
Clinical examples
Blood administrationAgePulmonary hypertensionRenovascular diseaseDefibrillator limitsLactate (Bentall, post Fallot)Professionalism
Up to how far should we limit exogenousblood administraion ?
68 yrs prof Dr EmeritusParoxystic atrial fibrillation and CADCABG (LIMA LAD; AO-vene-diag-RDP; Ao-FRIMA-Cx)+ epicardialPVI + LAA excision12h ICU: Hb 7,8 g/dl Hct 22% hypotension:inotropics (dobu 2µg/kg/min, nor 0,1 µg/kg/min),fluids (3L +)IBP 92/45mm Hg 96bpm Temp 36,7° C1U PC: frisson, nausea, malaise
titel4 27/10/2016
Medical indication : transfusion limits
Murphy GJ (Circ 2007) : limit =Hct 21,transfusion = 6x↑mortality risk at 30d(cardiac & pulmonary),γ if no major renal, cerebral or intestinal antecedents
Patient’s preference
Contextual features
titel5 27/10/2016
titel6 27/10/2016
Age a cost-inducing and limiting factor ?
Man 92 yrs, MV disease: MS (gradient 17mm Hg) & MI 2/4 (multiple jets), atrialfibrillation, gardener, mentally optimalRepeated requests (3x) for surgeryMVR (Bio), stapling LAAExtubation: 3h; ICU: 36hAF: Cordarone postoperativelyLOS: 22d
titel7 27/10/2016
Did we have a choice? …
Repeated and convincing requestsYoung biological ageFamily supportCare for great-grand child
titel8 27/10/2016
Carottes
titel9 27/10/2016
Pulmonary hypertension
Female 85 years 9d inferior STEMI ,VSD 15 mm,Qp/Qs = 2,0; SPAP 60mm Hg, mental state: optimal
« Docteur, je ne veux pas mourir commeça, je me sens mourir à petit feu,remettez- moi vite d’aplomb… J’aitoujours été bien et ce n’est qu’aprèsque le remplaçant de mon généraliste aitaugmenté mes médicaments pour la tensionque je suis devenue malade »VSD-patch closure + CABG LIMA LAD; Ao-vene-RDPMilrinone, noradrenaline, NO + epoprostenolICU: 3d, delirium POD1-D2LOS: 28dtitel10 27/10/2016
Savoir: oui ? – pouvoir oui?
Observation timeMental stateRequest GP
titel11 27/10/2016
Medical indication
Age does not limit quality of life improvement incardiac valve surgery (Sedrakyan JACC 2003)
> 90 & 100 yrs: careful selection allows to reducerisk (Bridges CR J Am Coll Surg 2003)
Quality of life in the very elderly after cardiacsurgery: a comparison between long-term survivorsand an age - matched population population selection improves outcome
(Sjögren J, Gerontol 2004)
titel12 27/10/2016
titel13 27/10/2016
Renovascular disease
Female 57yrs with syncopes after eatingVascular obstructive disease (Ao-Bifemor bypas,2011), mesenteral & vascular ischemia, 1 No &atrophic Kidney- 1 renal artery stenosis (CNI, Cr Cl15ml/min) (Cl III-IV), recent ARF, CADScheduling: TPL Insertion supra-renal aorta Dacronprothesis with reimplantation aa. Mes, TC and renalartery reanastomisis
“I am too young to be on dialysis”Planning:
Optimizing renal treatment and blood pressure (8W)BMS-stent in left main
titel14 27/10/2016
Renovascular disease (2)
Hickman catheter - thoracoabdominal aorticendarterectomy (CSF drainage- renoplegia)Postoperative course : Addison (CVVH≠)ICU 6d, LOS 12d; Cr Clear 25 ml/min outApproach:
Preoperative renal (and cardiac)optimizationSurgical downsizing and renoplegiaPre-per & post operation anesthesia managementAnxiety reduction
titel15 27/10/2016
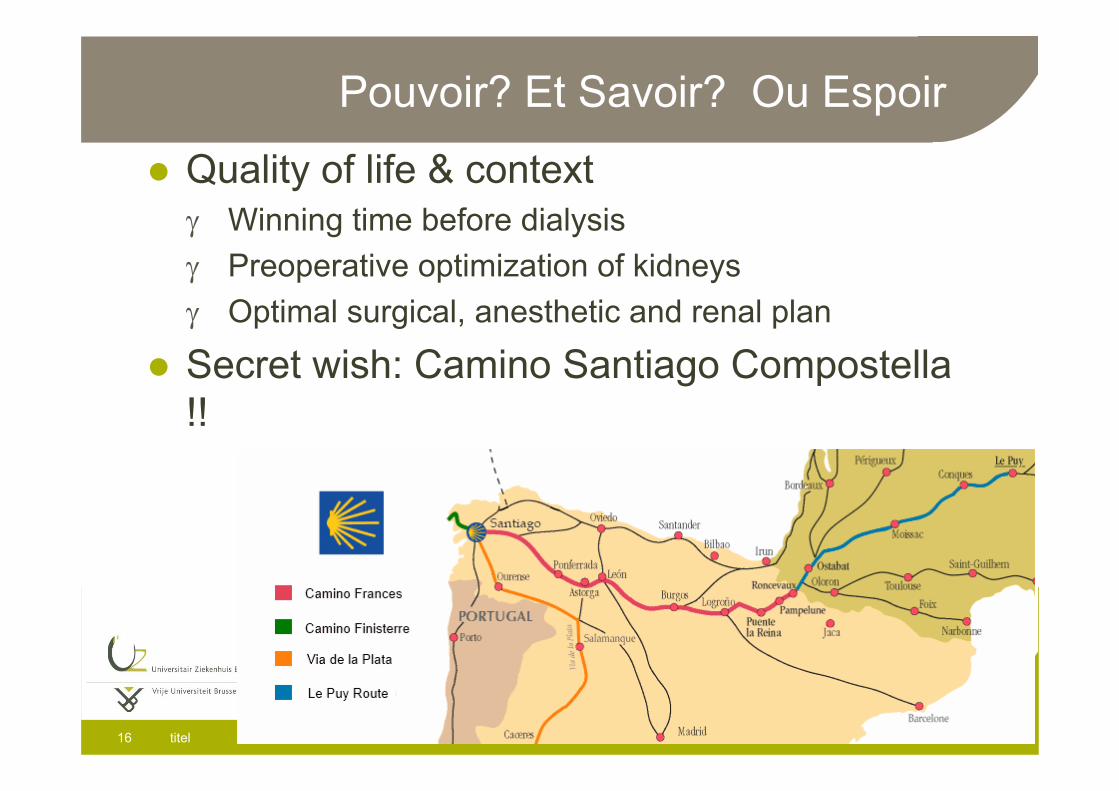
Pouvoir? Et Savoir? Ou Espoir
Quality of life & contextγ Winning time before dialysisγ Preoperative optimization of kidneysγ Optimal surgical, anesthetic and renal plan
Secret wish: Camino Santiago Compostella!!
titel16 27/10/2016
Bentall post Fallot : lactic acidosis
52 yrs, Fallot-correction at 6 yrs, now AI ¾-4/4Bentall and MorrowFemoro-femoral ECC initiationDuring ECC ↑ lactate concentrations ( 8,5 mmol/l)
Meanwhile urgent unstable CABG
titel17 27/10/2016
Causes of lactic acidosis
Cardogenic or hypovolemic shock, advanced heart failureSepsisSevere traumaSevere hypoxemiaCO poisoningSevere anemia (Hb 8.3 mg/dL)Diabetes mellitus (without meformin)Cancer ( lymphoma, leucemia)Liver disease (moderate alcohol use)PheochromocytomaMetformin, Cocaine, Alcohols, glycols,cyanide, β2 agonists,propofol, <vit B1
titel18 27/10/2016
Unforeseen extension of surgery time
Options:Continue surgery and consult internal medicine (time>)End surgery quit femoro-femoral ECC-bypass l (time<?)Change femoral bypass to aortic -graft-RA-ECC-bypass(time ?), See what happens with lactate (time <<?)
Lesser efficacy of inotrope?Workload: AVR (3) or urgent unstable left-mainCABG (2)
?
titel19 27/10/2016
Bentall post-Fallot correction: lactic acidosis
Removal of femoral cannulation, aorticcannulation, reperfusion end-surgery↓ lactate (6 mmol/l)
Start urgencyFirst case: ICU within 6h: ↓ lactate ( 2,9 mmol/l)
titel20 27/10/2016
Defibrillator impactEsophageal-neo 37kg,43yr-old Jewish malecancer patient admitted for gastrostomy feedingtube revision under general anaesthesiaCAD, EF 23% with AICDAgrees with minor surgery but wants to die –repeatedly resuscitated by his AICD
Some AICD can’t be turned off (rate & output voltagecan ↓but difficult to switch off)Magnet overruling (St-J Med Biotronik, Bos Sci Guid)AICD specific DNR-order?Off-switching AICD request: religious susceptibilities
Pre-AICD discussion of AICD consequencestitel21 27/10/2016
Use caution when applying magnets topacemakers or defibrillators for surgery
Timely preoperative review andprogramming of AICD function as necessaryfor surgery (Schulman Anest Analg 2013)
We need to understand our electronics!It’s not just about the magnet! (Welner -Huang Anesth Analg 2014)
Creating an Anesthesiologist-run pacemakerand defibrillator service ! ( Rozner MA, Anesthesiol
2015)
titel22 27/10/2016
Decision making
l Medical indicationl Key factorsl Professionalism
l Patient’s preference- wishl Quality of lifel Contextual factors
titel23 27/10/2016
Medical indication: avoid harm
Acute- Chronic-Critical-Reversible-Emergent -Terminal?Goals: cure, improve or maintain?Relief of symptoms: pain, suffering?Health promotion?Prevention?Education of patientWhen not indicated ?
titel24 27/10/2016
Medical indication: 4K-factors
Autonomy: emphasizes the respect of the patient’swishes, values and religious belief and the patient’sright to continue withdraw to medical treatment free frominfluenceBeneficence: moral obligation to act for the benefit ofothers requiring the prevention of harm, removing ofharm and the promotion of goodNon-maleficence assumes the obligation not to inflictharm to othersJustice refers to a fair and equitable distribution ofbenefits and burden of all individuals in a society
titel25 27/10/2016
Professionals…
+ Accountability+ Humanism+ Ethical behavior+ Well-being
≠ Abuse of power≠ Bullying≠ Inadequate man. private info≠ Dishonesty≠ Conflict of interest≠ Fraud
≠ Sexual harassment
titel26 27/10/2016
Patient’s preference
In accordance with their wishes, values,religionRight to initiate, continue or withdraw fromtreatmentAssess: adequate information provided,understanding consent
titel27 27/10/2016
Quality of life
Prospect of the future, return to normal lifeBiases present for the provider’s evaluationEthical issuesPlans for life-sustaining treatment?Legal and ethical status of suicide?
titel28 27/10/2016
Contextual feature (justice, fairness)
FamilySocialInstitutionalFinancialLegalBusinessProfessionalOther parties of interestReligion
titel29 27/10/2016
Religious perspectives for end-of-life issues
Consider also the religious & culturalperspective↓ Confusion, conflict & untoward clinicalevents!Conflict prevention = better knowledge &respect of patient’s wishes
titel30 27/10/2016
Judaism, islam and catholicism
“The proprietor of human life is god”
Individual great diversity of views
Judaism: continuous versus intermittent treatment
Islam (and Judaism): religious advisor and welfare in
accordance with religious laws
Catholicism: focus on patient’s decision for treatment,
may decline extraordinary mean to preserve life
titel31 27/10/2016

2015
titel32 27/10/2016
Cost Health-BenefitHuman well-being
Savoir/ Pouvoir