Irradiaon Prophylac&que Cérébrale (IPC) dans le Carcinome ... · dans le Carcinome à Pe&tes...
25
Irradia&on Prophylac&que Cérébrale (IPC) dans le Carcinome à Pe&tes Cellules (CPC) Situa&on en 2016 Dr Eric DANSIN Pneumo-oncologue Département de Cancérologie Générale, CLCC Lille [email protected] Mardi 12 janvier 2016
Transcript of Irradiaon Prophylac&que Cérébrale (IPC) dans le Carcinome ... · dans le Carcinome à Pe&tes...

Irradia&onProphylac&queCérébrale(IPC)
dansleCarcinomeàPe&tesCellules(CPC)
Situa&onen2016
DrEricDANSINPneumo-oncologue
DépartementdeCancérologieGénérale,[email protected]
Mardi12janvier2016

Déclara&ondeliensd’intérêts
• Enlienaveclesujetabordé:• Aucun
• Sanslienaveclesujetabordé:• Boardd’experts:Lilly,BIF,PFO,Roche,Novar&s,Pfizer,BMS,AZ
• CoordonnateuressaiscliniquesFrance:Pfizez,Roche,AZ
• Fondsderecherche:Roche
• Instances:ANSM,INCa

CPC.Evolu&onsrécentes
• Stadeslimités:• A[ente:CT-RTbifrac&onnée(45Gy)vsmonofrac&onnée(66Gy)(essaiCONVERT)
• Stadesdiffus• «succès»Amrubicine(phasesIIasia&quesnonconfirmées…)• Echecbevacizumab(PujolJL.AnnOncol.2015May;26(5):908-14)
• Signalsuni&nibenmaintenance(ReadyNE.JCO.2015May20;33(15):1660-5)• RTthoraciquechezlesrépondeurs(SlotmanBJ.Lancet.2015;385:36-42)

Design
• PhIIIrandomisée,42centres(EuropeNord,2009-2012)• CPCdiffusrépondeurs• IPCpourtous(20-30Gy)
30 Gy (10 fractions) Volume post chimio
OP: Taux de survie à 1 an OS: SSP, RO thorac., tox. N attendu: 483 patients Stratification: centre, présence ou absence de lésion thoracique
Slotman BJ et al. Lancet. 2015 Jan 3;385(9962):36-42
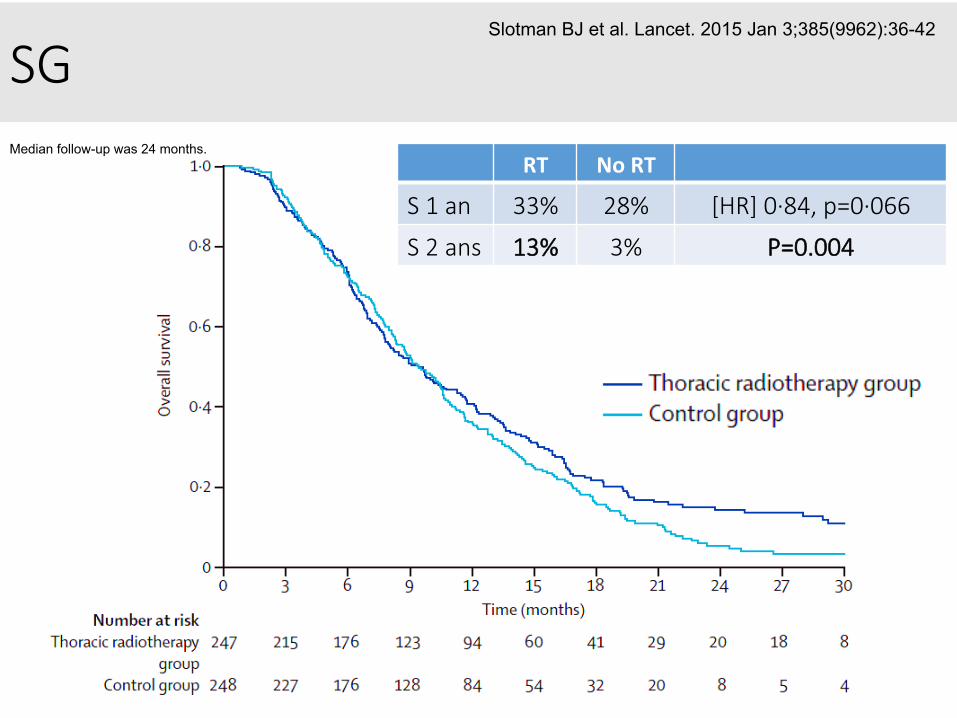
SG Median follow-up was 24 months.
RT NoRT
S 1 an 33% 28% [HR] 0·84, p=0·066
S 2 ans 13% 3% P=0.004
Slotman BJ et al. Lancet. 2015 Jan 3;385(9962):36-42

Rechutes
Slotman BJ et al. Lancet. 2015 Jan 3;385(9962):36-42
p<0.0001
Thorax:1ersitedeprogression103(42%) 193(78%)p=0.009

Quid de l’IPC ???
HistoriqueRecommanda&ons
Débat

IPC, niveau de preuve
• Méta-analyse(7essais,987pa&ents[86%localisés]enRCaprèsinduc&on)
• Réduc&ondurisquedeMCde54%• MCà3ans:avecIPC:33%vssansIPC:59%
• Réduc&ondurisquededécès• Sà3ans:avecIPC:21%vssansIPC:15%
• Bénéficeindépendantâge,PS,stades,typed’induc&on
AuperinA.NEnglJMed.1999;341:476–84.

SlotmanB.NEnglJMed.2007Aug16;357(7):664-72
IPC, niveau de preuve
• Essairandomisé:286pa&entsdiffus,répondeursaprèsinduc&on
• Résultats(1/2):Réduc=ondesMC
Risqueà1an:14.6%avecIPCvs40.4%sansRechutecérébrale1ère:9%avecIPCvs35%sans

SlotmanB.NEnglJMed.2007Aug16;357(7):664-72
IPC, niveau de preuve
• Essairandomisé:286pa&entsdestadeIV,répondeursaprèsinduc&on
• Résultats(2/2):bénéficeensurvie
MédianeSG(mois):6.7avecIPCvs5.4sansSGà1an:27.1%avecIPCvs13.3%sans

En praLque,
• IPCdoserecommandée:25Gyen10frac&ons(LePéchouxC.LancetOncol.2009May;10(5):467-74)
• encasdeM+:RTintoto30Gyen10frac&ons
• Pasdechimioconcomitanteàl’IPC• Pasd’IPCencasdePS≥2et/ousitroublesneurocogni&fs• Dosecorréléeàlamortalitéetàlaneuro-toxicité• Appari&onneuro-toxicité6à24moisaprèsPCI(CrossenJRJCO1994;12:627–42)
• Neuro-toxicité(plancogni&f)corréléeaussiàl’âge

Neuro-toxicité
Chronicneurotoxicityisdefinedasthedeteriora&oninatleastoneofthefollowingwithoutdevelopmentofbrainmetastasisat12months:HVLT-recall,HVLT-recogni&on,HVLT-delayedrecall,COWAT,TMT-A,orTMT-B
Wolfson AH. Int J Radiat Oncol Biol Phys. 2011 Sep 1;81(1):77-84
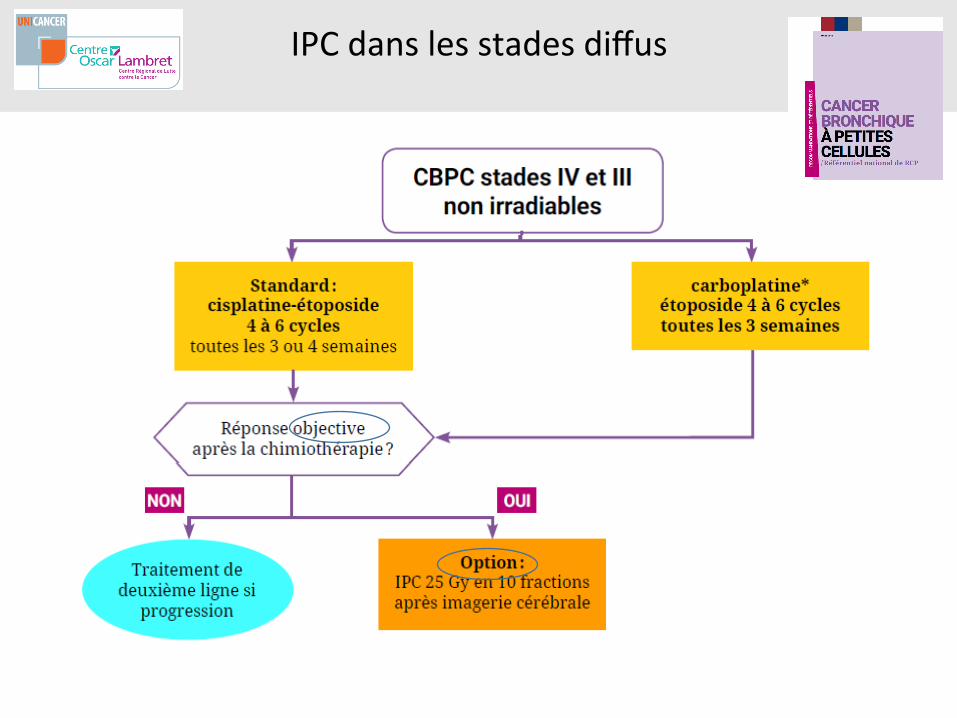
IPCdanslesstadesdiffus

IPCdanslesstadeslocalisés
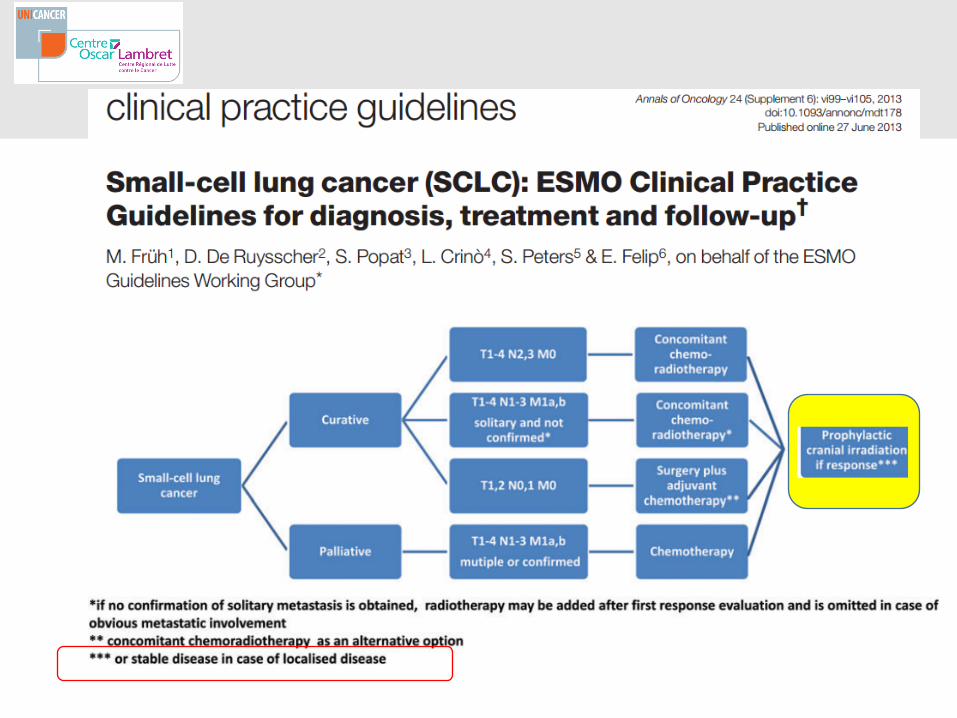


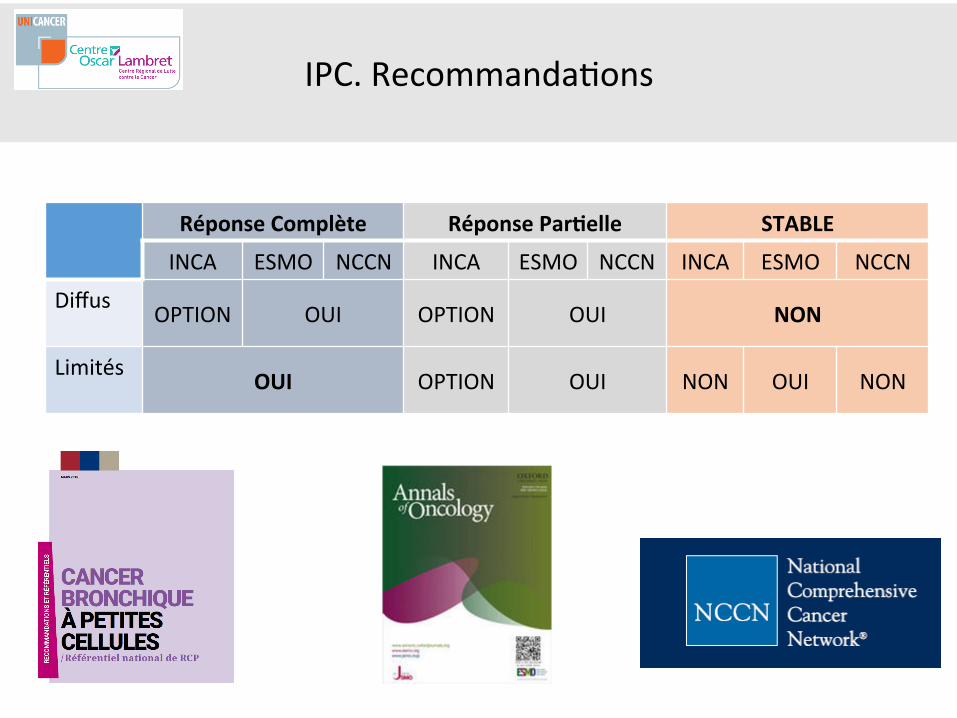
IPC.Recommanda&ons
RéponseComplète RéponsePar=elle STABLE
INCA ESMO NCCN INCA ESMO NCCN INCA ESMO NCCN
Diffus OPTION OUI OPTION OUI NON
Limités OUI OPTION OUI NON OUI NON
IPC.Recommanda&ons
RéponseComplète RéponsePar=elle STABLE
INCA ESMO NCCN INCA ESMO NCCN INCA ESMO NCCN
Diffus OPTION OUI OPTION OUI NON
Limités OUI OPTION OUI NON OUI NON
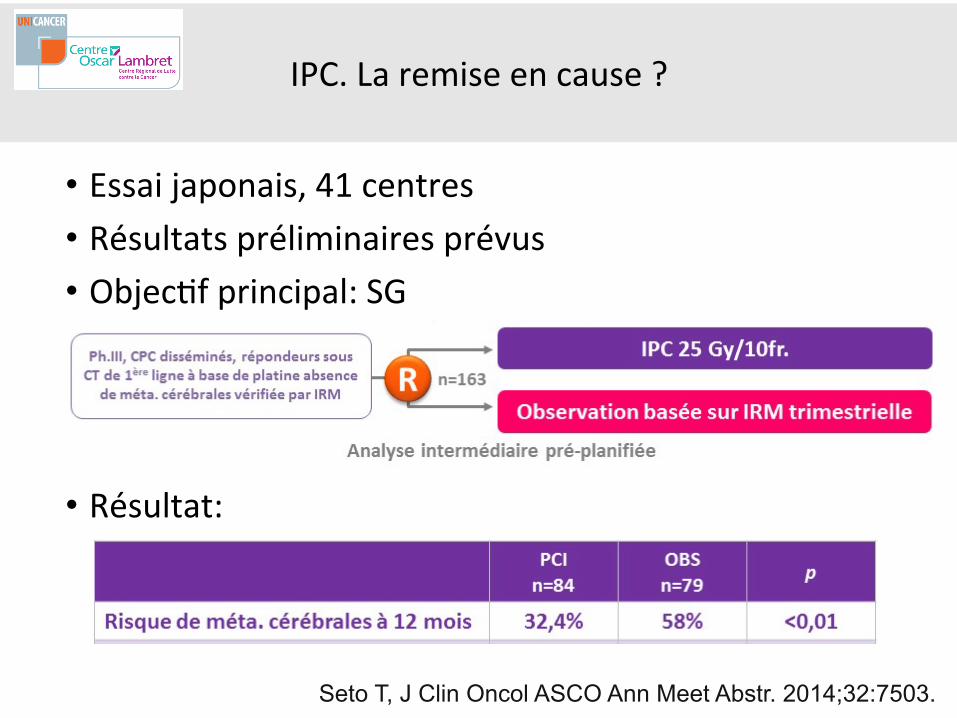
IPC.Laremiseencause?
• Essaijaponais,41centres• Résultatspréliminairesprévus• Objec&fprincipal:SG
• Résultat:
Seto T, J Clin Oncol ASCO Ann Meet Abstr. 2014;32:7503.

IPC.Laremiseencause?
• Résultat:SG
Seto T, J Clin Oncol ASCO Ann Meet Abstr. 2014;32:7503.
SG BrasIPCN=84
BrascontrôleN=79
Médiane(mois) 10.1 15.1
HR1.38CTultérieuresL2/L3/L4 82%/43%/16% 89%/53%/27%
RTcérébraleultérieure 69%

Analyse
Slotman Seto
Réduc&onrisqueMC oui oui
BénéficeenSG oui non
année 2007 2014
publica&on NEJM Abstract
N 286 163sur330prévus
Stadesdiffus exclusivement exclusivement
Typederéponse «répondeurs»sansdéf. ROetMS
Typed’induc&on +/-pla&ne +pla&ne
DoseIPC Variable(20à30Gy) Fixe(25Gy)
Imageriecérébrale CTouIRM IRM
Imageriesystéma&queàinclusion
non oui
Suivisystéma&que EncasdeSF oui(IRM/3mois)
Alors IPC ou pas ?...
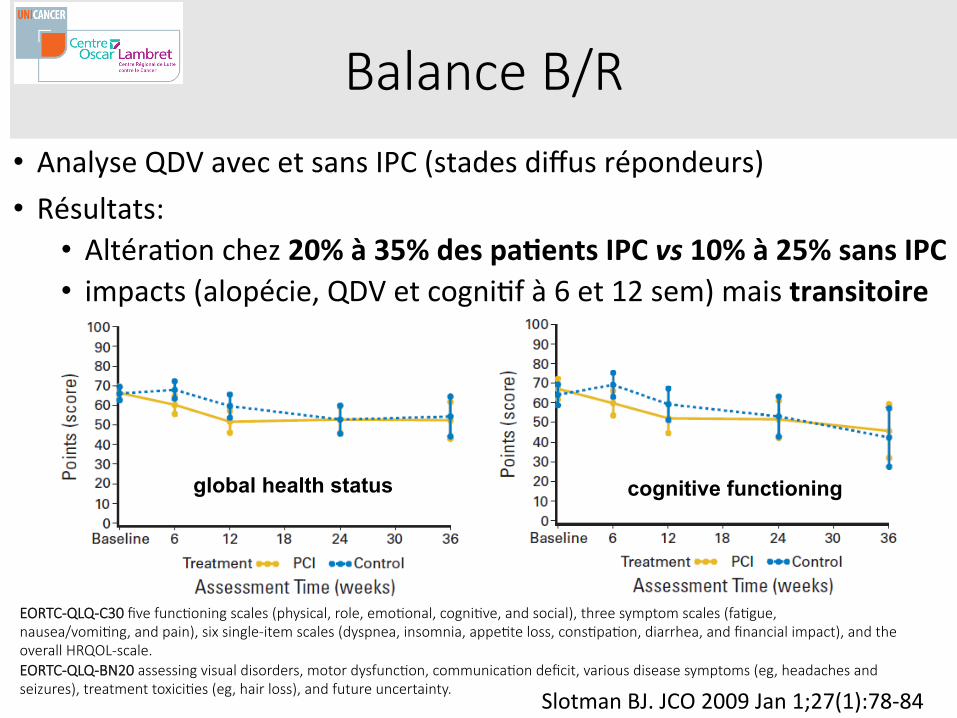
Balance B/R • AnalyseQDVavecetsansIPC(stadesdiffusrépondeurs)• Résultats:
• Altéra&onchez20%à35%despa=entsIPCvs10%à25%sansIPC• impacts(alopécie,QDVetcogni&fà6et12sem)maistransitoire
SlotmanBJ.JCO2009Jan1;27(1):78-84
EORTC-QLQ-C30 five funcLoning scales (physical, role, emoLonal, cogniLve, and social), three symptom scales (faLgue, nausea/vomiLng, and pain), six single-item scales (dyspnea, insomnia, appeLte loss, consLpaLon, diarrhea, and financial impact), and the overall HRQOL-scale. EORTC-QLQ-BN20 assessing visual disorders, motor dysfuncLon, communicaLon deficit, various disease symptoms (eg, headaches and seizures), treatment toxiciLes (eg, hair loss), and future uncertainty.
global health status cognitive functioning

Balance B/R • Effetsneuro-cogni&fsà2ansaprèsIPC(25Gy)• Compara&fsAVANTetAPRESIPC
• AvantIPC:altéra&onchez47%despa&ents• AprèsIPC:altéra&ontransitoiremaissansdéclinpersistantsignifica&f
GrosshansDR.Cancer.2008;112:589–95.
TesLng focused on learning and memory (Verbal SelecLve Reminding Test and Benton Visual RetenLon Test11,12), execuLve funcLon (Wisconsin Card SorLng, number of perseveraLve errors, and Trail Making Test Part B13,14), verbal and visual reasoning (SimilariLes and Block Design subtests of the Wechsler Adult Intelligence Scale-Revised [WAIS-R]15), afenLon (Digit Span and ArithmeLc subtests of the WAIS-R15), processing speed (Digit Symbol subtest of the WAIS-R and Trail Making Test Part A14,15), Expressive and recepLve language (Controlled Oral Word AssociaLon and Token Test16), motor coordinaLon (grip strength, grooved pegboard test, and finger tapping14).

Conclusion
• Demeureunstandardpourlespa&entslocalisésenRO• Remiseencausepourlesstadesdiffusrépondeurs
• Intégrerniveauderéponse:RCvsRP• Considérerencoreplusleséléments«freinants»:âge,co-morbidités,étatcogni&fpréalable
• PrivilégierIRMenbaseline• Evalua&oncogni&vesystéma&queavantIPC?
• Renforcerlacollabora&onavecneuro-oncologues• DiscuterbalanceB/Rindividuelle…
• Op&misa&onRT:protec&onhippocampesystéma&que?• RôledelaRTSàlaplacedel’IPCouaprèsIPC?• Défi=toujoursletraitementsystémique…