insuffisance rénale aiguë Acute Kidney Injury (AKI)cuen.fr/powerpoint/2018_fevrier...
23
19/04/2018 1 Pr L Frimat-Service de Néphrologie ([email protected] ) Épidémiologie de l’insuffisance rénale aiguë 1. Définition insuffisance rénale aiguë = Acute Kidney Injury (AKI)
Transcript of insuffisance rénale aiguë Acute Kidney Injury (AKI)cuen.fr/powerpoint/2018_fevrier...

19/04/2018
1
Pr L Frimat-Service de Néphrologie([email protected])
Épidémiologie
de l’insuffisance rénale aiguë
1. Définition
insuffisance rénale aiguë=
Acute Kidney Injury (AKI)

19/04/2018
2
Définition (2003)
si créatininémie < 221 µmol/l, augmentation de 44,2 µmol/l
si créatininémie ≥ 221 µmol/l, augmentation de 20 %
Singri N. JAMA 2003
S0 S1 S2 S3 S4
Cré
atin
iném
ie (
µm
ol/l)
80
100
120
140
160
180
200
220
240
260
B
C
Introduction de l’IEC
ou du sartan
A
Bakris G. Arch Intern Med 2000
A : Fonction rénale normale B : Fonction rénale altérée
Sténose bilatéraleInsuffisance cardiaqueDéplétion hydrosodée

19/04/2018
3
Bellomo Crit Care 2004Mehta RL. Crit Care 2007
Classification RIFLE (2004)Acute Dialysis Quality Initiative (ADQI)
Définition de l’insuffisance rénale aiguë
Acute Kidney Injury (AKI) is defined as any of the
following (Not Graded): – Increase in SCr by ≥ 0.3mg/dl (≥ 26.5 µmol/l) within
48 hours; or – Increase in SCr to ≥ 1.5 times baseline, which is known
or presumed to have occurred within the prior 7 days; or
– Urine volume < 0.5ml/kg/h for 6 hours.Thakar CV Crit Care Med 2009
Ioannidis M Intensive Care Med 2009KDIGO. KI 2012
Bellomo R. Lancet 2013

19/04/2018
4
Chapter 2.1 KDIGO. KI 2012
Chapter 2.5 KDIGO. KI 2012

19/04/2018
5
Chapter 2.5 KDIGO. KI 2012
Quelles sont les limites de ces définitions ?

19/04/2018
6
Wang HE. NDT 2013
Augmentation relative versus absolue de la créatinine plasmatique
26,5 / 61 µmol/l
62 / 105 µmol/l
≥ 106 µmol/l
Augmentation absolue de la créatinine plasmatique- Plus pratique
- pas besoin de rechercher une référence pré-hospitalière- pas besoin du volume d’urines
- Plus sensible pour des variations modestes- Plus performant pour la prédiction de la mortalité hospitalière
Wang HE. NDT 2013

19/04/2018
7
Diagnostic Insuffisance cardiaque & insuffisance rénale
BNP
Créatininémie Temps
Approche diagnostiqueAKI versus AMI
Années Coeur (AMI) Rein (AKI)
1960 LDH Créatininémie
1970 CPK, myoglobine Créatininémie
1980 CK-MB Créatininémie
1990 Troponine T Créatininémie
2000 Troponine I Créatininémie
����
Amélioration des traitements
50% ���� mortalité
����
Retard diagnostic,
traitement palliatif (suppléance)
Recherche clinique difficile, faute de
référence

19/04/2018
8
Schmidt-Ott KM. NDT 2011
NGAL
Proportion d’IRA détectées grâce à NGAL versus créatininémie
Haase M. JACC 2011

19/04/2018
9
2. Epidémiologie descriptive
Histoire naturelle de l’insuffisance rénale aiguë
17 aout 1999

19/04/2018
10
24.5%
29.6%
25.6%
14.7%
23.7%
16.7%
14.7%
22%
20.1%
31.5%
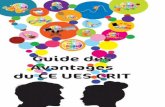
FIRST META-ANALYSIS 2004-2012AKI INCIDENCE BY KDIGO DEFINITION
FIRST META-ANALYSIS 2004-2012AKI INCIDENCE BY KDIGO DEFINITION
Selon une étude sur une cohorte de 50 millions de patients,
en cours d’hospitalisation (KDIGO definitions),
1 adulte sur 5,
1 enfant sur 3
a une insuffisance rénale aiguë.
Susantitaphong et al CJASN 2013

19/04/2018
11
Incidence annuelle de l’IRA requérant une épuration extra-rénalepar million d’habitants
après exclusion des IRC terminales
159,2
209,4
0
50
100
150
200
250
MARNE
Inci
denc
e pa
r m
illio
n d'
habi
tant Année
2000Année 2016
Courtoisie Prs Rieu et Touré, Reims
0
200
400
600
800
1000
1200
< 20 20-49 50-59 60-69 70-79 80-89
Inci
denc
e pa
r m
illio
ns d
'hab
itant
s
Âge (ans)
Année …Année …
Incidence annuelle de l’IRA requérant une EERpar million d'habitants
après exclusion des IRC terminales
Moyenne d’âge : � 67,2 ans� 66,1 ans
Incidence annuelle chez les patients âgés de ≥ 75 ans :� 889,3 par million d’habitants� 839,6 par million d’habitants
Courtoisie Prs Rieu et Touré, Reims

19/04/2018
12
Prescott GJ. NDT 2007
Ecosse 2002 – 2 facteurs ou plus dans 50 % des cas
A = IRC-versus
B= IRC+
ISN 0by25 mission is to achieve zero
preventable deaths from AKI by 2025 and by promoting globally applicable strategies
that permit timely diagnosis and treatment of AKI for patients with potentially reversible
diseases
WHAT IS 0by25?

19/04/2018
13
AKI IN HIGH INCOME COUNTRIES AKI IN LOW-MIDDLE INCOME COUNTRIES
Occurs predominantly in the ICU Two main patterns:
i. Small rural health
centers/hospitals
ii. Big cities big hospitals, ICUs
Associated with multiple organ failure Often caused by a single disease, multiple
organ failure less common
Associated with sepsis and complex surgery
(major trauma, cardiovascular surgery)
Frequently associated with
o Specific disease (example diarrhea)
o Specific infection (example malaria)
High mortality Apparently HIGHER mortality
A disease of increasingly older populations A disease of young, otherwise healthy people
Increasing incidence? Increasing incidence?
Accurately reported LESS Severely underreported
Difficult to prevent Eminently preventable
Very costly to treat Very inexpensive to treat at early stages,
unaffordable at severe stages
Characteristics of AKI in HIC and LMIC
Malaria deaths per 100000 population
Murray et al, A systematic analysis for the Global Burden of Disease Study 2013
Lancet 2014; 384: 1005-1070

19/04/2018
14
Relative contribution of medical, surgical, and obstetric causes of AKI in different tropical
countries .
Vivek Jha, AKI in the tropics, Oxford Textbook of Clinical Nephrology 4th edition, 2015
Conclusion• L’IRA est une pathologie fréquente, très
hétérogène qui survient souvent loin « des yeux des néphrologues ».
• 0by25 initiative =) 5Rs strategies• Risk anticiper le risque• Recognition surveiller• Response prévenir• Renal support pouvoir dialyser• Rehabilitation accompagner la convaslescence• Education

19/04/2018
15
EPIRAN studyEpidémiologie de l’insuffisance rénale chronique dans l’agglomération de
Nancy
� Population of 250 000
� The University hospital of Lorraine region
� 16 laboratories (3 non for profit, 13 for profit)
� Serum creatinine ≥ 150 µmol/l
Ayav C et al. BMC 2017 open access
From 1/1/04 to 30/6/06, 54884 measurements
4406 subjects (18% of the population)
Acute renal failure = 59%
Prevalent CKD = 23%
Incident CKD = 14.3% (630 patients)
145 impossible classifications
Chaque jour,1 IRA
pour 75 000 hbts

19/04/2018
16
Risque relatif de décès / moyenne

19/04/2018
17
IEC+
Furosémide+
AINS en automédication
=IRA sur IRC
avec hyperkaliémie
17 aout 1999

19/04/2018
18
Tremblement de terre
Le 17 aout 1999, sur une zone géographique de 15 millions d’habitants,
Plus de 17 000 mortsPrès de 45 000 blessés24 000 hospitalisations
639 IRA477 dialysés
97 décès

19/04/2018
19
3. Epidémiologie analytique
Mortalité non ajustée des patients
requérant une suppléance de la fonction rénale (England 1998 to 2013)
Kohle NV. KI 2015Durée moyenne de séjour : 20 jours

19/04/2018
20
Ali T. JASN 2007
Étude en populationPourcentage de décès associé au RIFLE
Méta-analyse
Par rapport à un groupe contrôle sans IRA,
� Risque de décès prématuré × 2
� Risque d’insuffisance rénale chronique
constituée × 9
A un an, suivi
� Par un médecin : 60%
� Par un néphrologue : 15%
Coca SG et al. KI 2012

19/04/2018
21
Kessler M. AJKD 2003
Précoce Intermédiaire Tardive ≤≤≤≤ 1 m
> 12 m 1
≤≤≤≤ 12 m > 4 m 2
≤≤≤≤ 4 m > 1 m 3
IRC > 1 m 4
IRC ≤≤≤≤ 1 m 5
p
n = 261 n = 85 n = 42 n = 60 n = 54
Délai IRC –IRT (m) 55.8 20.7 12.6 35.2 0.2 < 0.0001
Aucune prise en charge primaire (%) 0.8 2.3 14.6 17 43.4 0.0001
Age (années) 61.5 61.2 65.9 69.1 62.9 0.0098
Co-morbidités (%)
Diabète 29.1 40 45.2 36.7 18.5 0.0175
Affections cardiaques 54.1 58.8 59.5 66.6 29.6 0.0645
Cancer évolutif 3.4 7.1 1.2 3.3 14.8 0.0021
Traitement de suppléance (%)
Dialyse péritonéale 20.7 18.8 23.8 11.7 1.9 < 0.0001
Transplantation d’emblée 3.4 2.4 0 0 0 < 0.0001
Modalités d’initiation du traitement
Ambulatoire (%) 19.9 7.1 7.1 6.7 0 < 0.0001
Durée de l’hospitalisation initiale (j) 15.8 21.5 25.2 28.1 36.1 < 0.0001
Dialyse en urgence (%) 29.1 38.8 57.1 83.3 85.2 < 0.0001
Cathéter temporaire (%) 30.6 41.1 57.1 81.7 92.6 < 0.0001
Oedème pulmonaire (%) 13.4 21.2 23.8 35 25.9 0.0016
Albumine (g/dl) 3.5 3.3 3.3 3.2 2.9 < 0.0001
Cholestérol (mg/dl) 190 230 190 180 170 < 0.0001
Comparaisons de 5 groupes de patients incidents pour la dialyse
Kessler M. AJKD 2003
Précoce Intermédiaire Tardive ≤≤≤≤ 1 m
> 12 m 1
≤≤≤≤ 12 m > 4 m 2
≤≤≤≤ 4 m > 1 m 3
IRC > 1 m 4
IRC ≤≤≤≤ 1 m 5
p
n = 261 n = 85 n = 42 n = 60 n = 54
Délai IRC –IRT (m) 55.8 20.7 12.6 35.2 0.2 < 0.0001
Aucune prise en charge primaire (%) 0.8 2.3 14.6 17 43.4 0.0001
Age (années) 61.5 61.2 65.9 69.1 62.9 0.0098
Co-morbidités (%)
Diabète 29.1 40 45.2 36.7 18.5 0.0175
Affections cardiaques 54.1 58.8 59.5 66.6 29.6 0.0645
Cancer évolutif 3.4 7.1 1.2 3.3 14.8 0.0021
Traitement de suppléance (%)
Dialyse péritonéale 20.7 18.8 23.8 11.7 1.9 < 0.0001
Transplantation d’emblée 3.4 2.4 0 0 0 < 0.0001
Modalités d’initiation du traitement
Ambulatoire (%) 19.9 7.1 7.1 6.7 0 < 0.0001
Durée de l’hospitalisation initiale (j) 15.8 21.5 25.2 28.1 36.1 < 0.0001
Dialyse en urgence (%) 29.1 38.8 57.1 83.3 85.2 < 0.0001
Cathéter temporaire (%) 30.6 41.1 57.1 81.7 92.6 < 0.0001
Oedème pulmonaire (%) 13.4 21.2 23.8 35 25.9 0.0016
Albumine (g/dl) 3.5 3.3 3.3 3.2 2.9 < 0.0001
Cholestérol (mg/dl) 190 230 190 180 170 < 0.0001
Comparaisons de 5 groupes de patients incidents pour la dialyse
12%

19/04/2018
22
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 90 180 270 360 450 540 630 720 810 900 990 1080 1170 1260
time (days)
surv
ival
rate
G1: Early referral > 12months
G2: Intermediate <= 12m > 4m
G3: Intermediate <= 4m > 1m
G4: Late <= 1m Chronic renal failure > 1m
G5: Late <= 1m Chronic renal failure <= 1m
1 an 2 ans 3 ans
Excès de mortalité…
Kessler M. AJKD 2003
Précoce Intermédiaire Intermédiaire Tardive Tardive p>12 mois 4 à 12 mois 1 à 4 mois IRC >1mois IRC<1mois
SF36 Rôle physique 19,0 13,6 8,6 6,8 21,2 .03
Rôle émotionnel 27,0 23,9 14,7 15,9 21,9
Vitalité 33,6 32,4 29,8 29,6 29,6
Santé perçue générale 39,8 35,9 39,7 40,6 45,1
Douleurs 48,7 47,0 48,5 42,7 46,3
Fonctionnement physique 48,7 41,4 42,6 32,8 51,0 .007
Santé mentale 51,8 47,8 43,2 45,9 43,3 .03
Fonctionnement social 57,6 54,7 66,4 51,5 49,4 .04
Score résumé physique 34,9 33,0 34,4 31,7 36,9 .07
Score résumé mental 38,0 36,4 35,9 35,9 33,0 .08
KDQoL Travail 21,3 22,9 16,7 20,0 23,1
Sexualité 45,2 48,3 34,4 38,0 38,8
Fardeau 46,4 41,0 42,2 40,6 38,1
Sommeil 52,5 54,4 53,9 51,1 55,3
Effet maladie 59,9 58,8 59,1 56,9 59,3
Cognition 64,4 63,5 58,3 60,6 67,7
Symptômes 66,4 68,2 63,7 66,1 64,7
Soutien social 66,8 67,7 67,7 67,0 67,9
Détérioration de la qualité de vie…
Qualité de vie initiale selon le type de prise en charge
Frimat L. Néphrologie & Thérapeutique 2007

19/04/2018
23
Précoce Intermédiaire Intermédiaire Tardive Tardive p>12 mois 4 à 12 mois 1 à 4 mois IRC >1mois IRC<1mois
SF36 Rôle physique 19,0 13,6 8,6 6,8 21,2 .03
Rôle émotionnel 27,0 23,9 14,7 15,9 21,9
Vitalité 33,6 32,4 29,8 29,6 29,6
Santé perçue générale 39,8 35,9 39,7 40,6 45,1
Douleurs 48,7 47,0 48,5 42,7 46,3
Fonctionnement physique 48,7 41,4 42,6 32,8 51,0 .007
Santé mentale 51,8 47,8 43,2 45,9 43,3 .03
Fonctionnement social 57,6 54,7 66,4 51,5 49,4 .04
Score résumé physique 34,9 33,0 34,4 31,7 36,9 .07
Score résumé mental 38,0 36,4 35,9 35,9 33,0 .08
KDQoL Travail 21,3 22,9 16,7 20,0 23,1
Sexualité 45,2 48,3 34,4 38,0 38,8
Fardeau 46,4 41,0 42,2 40,6 38,1
Sommeil 52,5 54,4 53,9 51,1 55,3
Effet maladie 59,9 58,8 59,1 56,9 59,3
Cognition 64,4 63,5 58,3 60,6 67,7
Symptômes 66,4 68,2 63,7 66,1 64,7
Soutien social 66,8 67,7 67,7 67,0 67,9
Détérioration de la qualité de vie…
Qualité de vie initiale selon le type de prise en charge
Frimat L. Néphrologie & Thérapeutique 2007
12%
Conclusion• L’IRA est une pathologie fréquente, très
hétérogène.
• Son pronostic est très réservé.
• Le RIFLE est validé pour prédire :– la mortalité hospitalière– les besoins de dialyse– la durée de l’hospitalisation– la récupération de la fonction rénale.
Il n’est pas validé pour prédire la mortalité à 90 jours et 6 mois.