Imagerie des troubles de l’olfaction...l’olfaction. Favorise la collectivisation humaine Sens à...
29
Imagerie des troubles de l’olfaction JL Sarrazin, F Benoudiba, S Hibat, D Ducreux Hôpital Américain de Paris CHU de Bicêtre
Transcript of Imagerie des troubles de l’olfaction...l’olfaction. Favorise la collectivisation humaine Sens à...

Imagerie des troubles
de l’olfaction JL Sarrazin, F Benoudiba, S Hibat, D Ducreux
Hôpital Américain de Paris
CHU de Bicêtre
GÉNÉRALITÉS
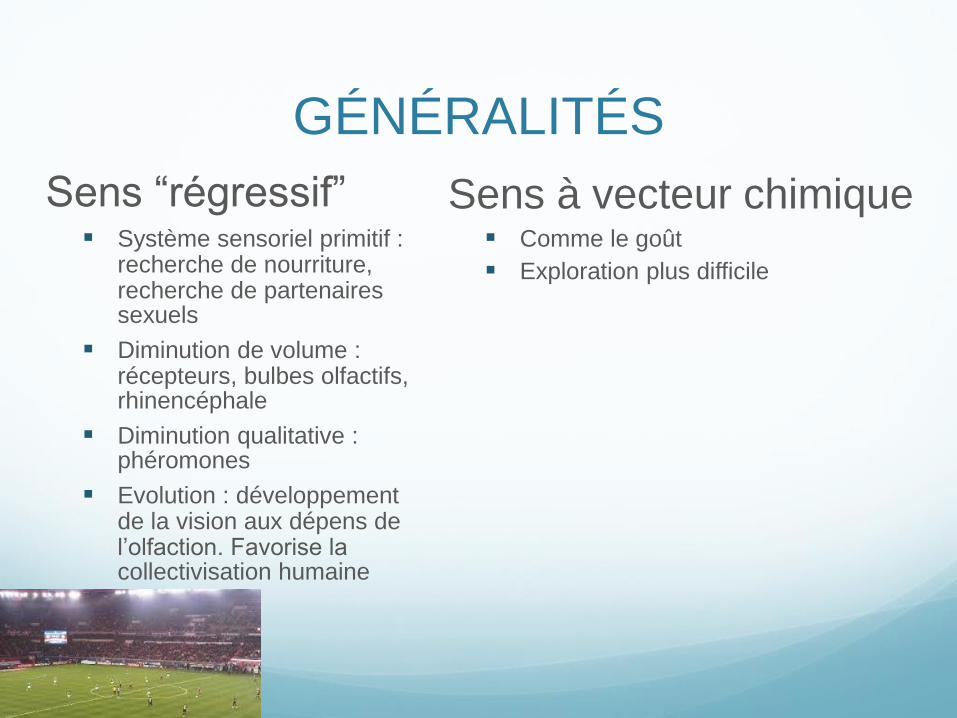
Sens “régressif” Système sensoriel primitif :
recherche de nourriture, recherche de partenaires sexuels
Diminution de volume : récepteurs, bulbes olfactifs, rhinencéphale
Diminution qualitative : phéromones
Evolution : développement de la vision aux dépens de l’olfaction. Favorise la collectivisation humaine
Sens à vecteur chimique Comme le goût
Exploration plus difficile

Anatomie
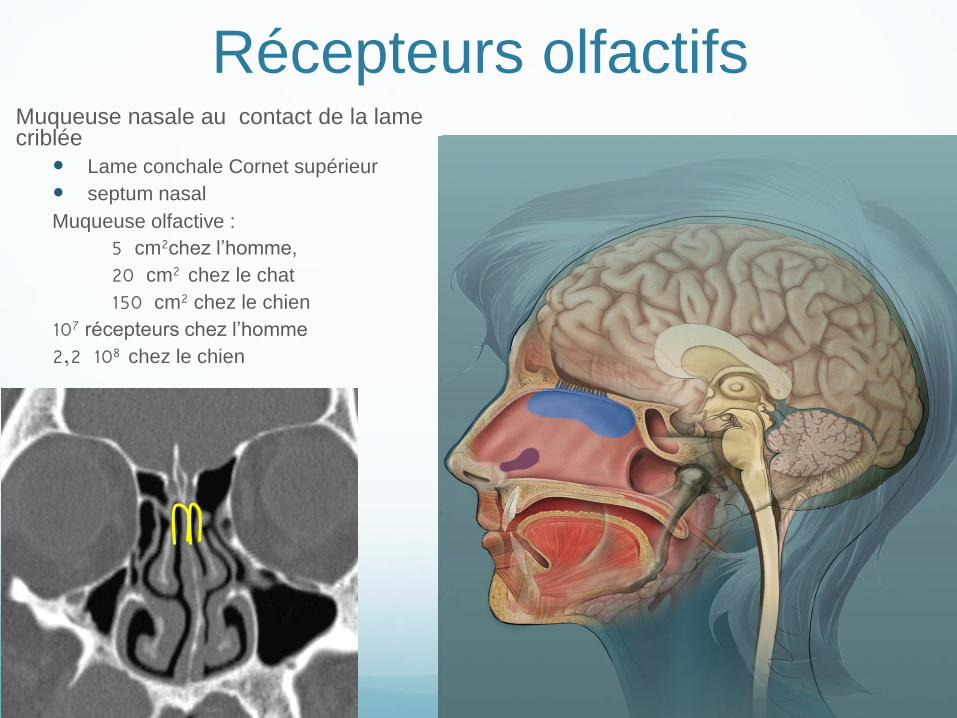
Récepteurs olfactifs Muqueuse nasale au contact de la lame criblée
Lame conchale Cornet supérieur septum nasal Muqueuse olfactive :
5 cm2chez l’homme,
20 cm2 chez le chat
150 cm2 chez le chien 107 récepteurs chez l’homme
2,2 108 chez le chien
Orthonasale Rétronasale

Muqueuse et Bulbes olfactifs Muqueuse
Neurones olfactifs bipolaires
Prolongement basal dans la muqueuse (8 à 20 cils)
Prolongement apical se regroupe par 10 à 100
Faisceaux d’axones myélinisés par des cellules de Schwann
Traverse la lame criblée pour entrer dans le crâne
Durée de vie 2 mois environ renouvellement constant
Bulbes
Longueur 12mm (6 -16 mm). Volume 58 mm3 avant 45 ans, 46 mm3 après 45 ans
Glomérules
Cellules périglomérulaires, cellules de grain, cellules en panache
Cellules mitrales (neurones)
dendrite : glomérule
axone : bandelette olfactive latérale
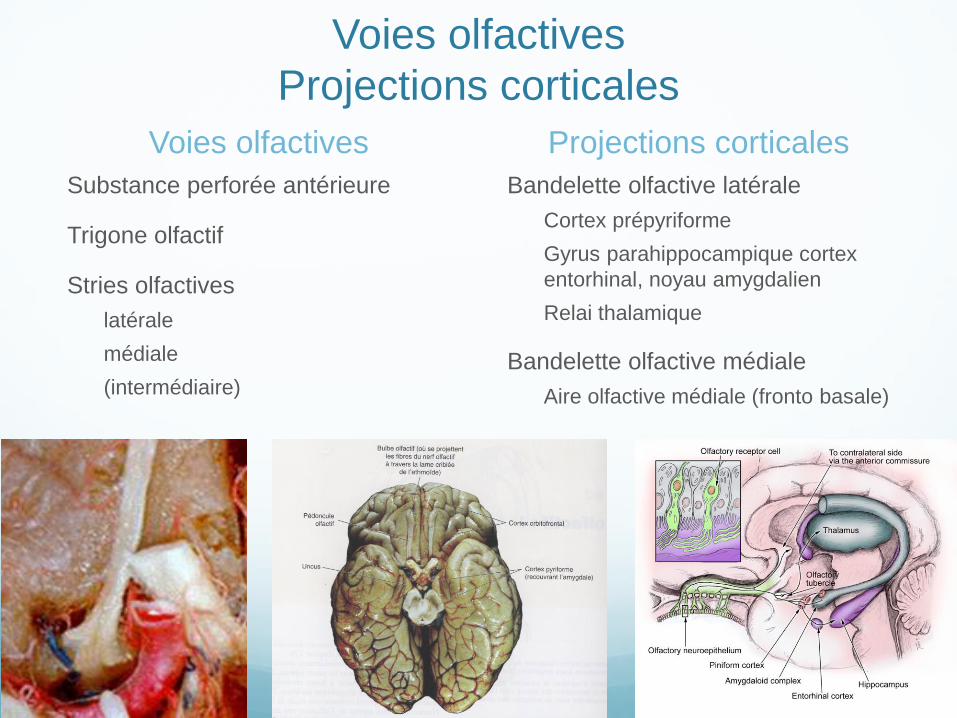
Voies olfactives
Projections corticales
Voies olfactives
Substance perforée antérieure
Trigone olfactif
Stries olfactives
latérale
médiale
(intermédiaire)
Projections corticales
Bandelette olfactive latérale
Cortex prépyriforme
Gyrus parahippocampique cortex
entorhinal, noyau amygdalien
Relai thalamique
Bandelette olfactive médiale
Aire olfactive médiale (fronto basale)

Qualitatif Quantitatif
Cacosmie
Parosmie
Hallucinations olfactives
Hyposmie
Anosmie
Hyperosmie
Classification des troubles de l’olfaction

EXPLORATION Fonctionnelle
Olfactométrie
Seuil de détection avec une concentration croissante (butanol)
Test de discrimination qualitative
Test de mémoire et de reconnaissance
Test d’identification
Examen ORL
Imagerie
TDM
IRM
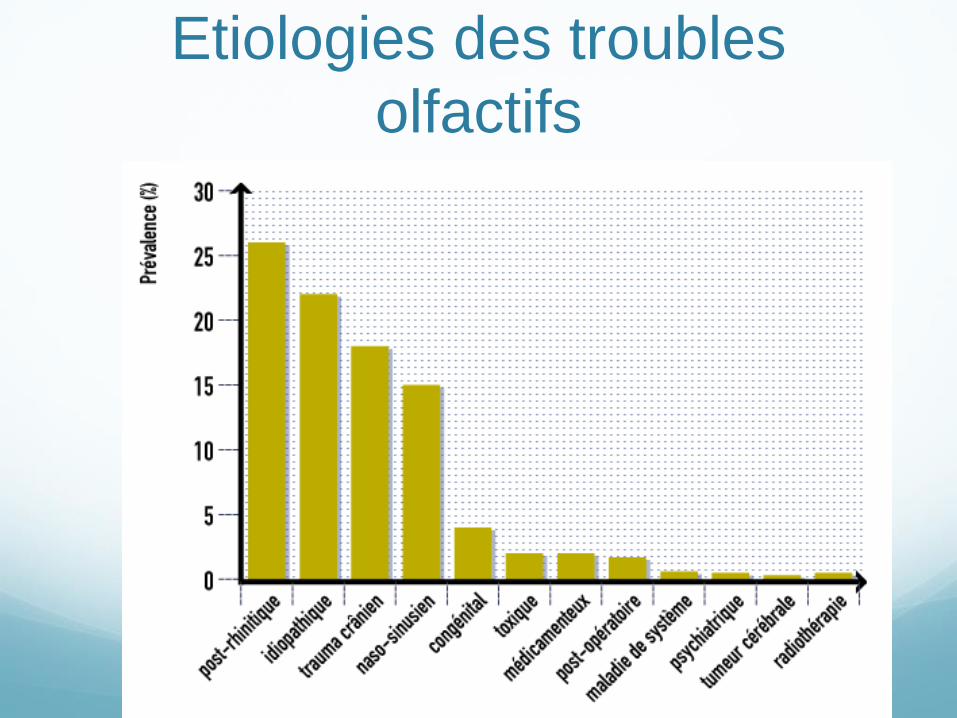
Etiologies des troubles
olfactifs
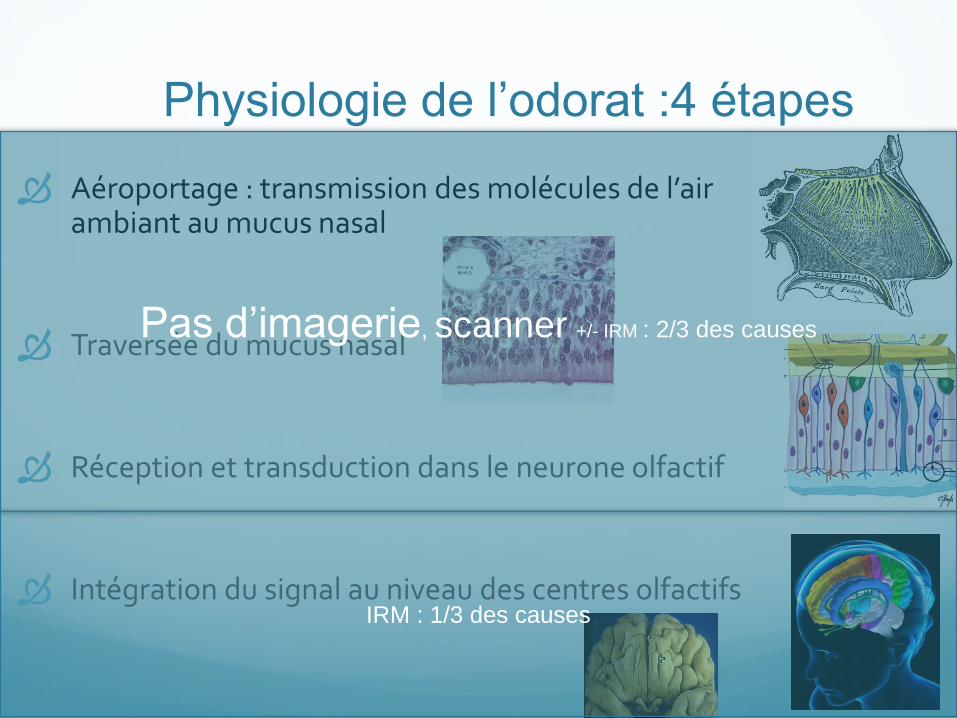
Physiologie de l’odorat :4 étapes
Aéroportage : transmission des molécules de l’air ambiant au mucus nasal
Traversée du mucus nasal
Réception et transduction dans le neurone olfactif
Intégration du signal au niveau des centres olfactifs
Pas d’imagerie, scanner +/- IRM : 2/3 des causes
IRM : 1/3 des causes
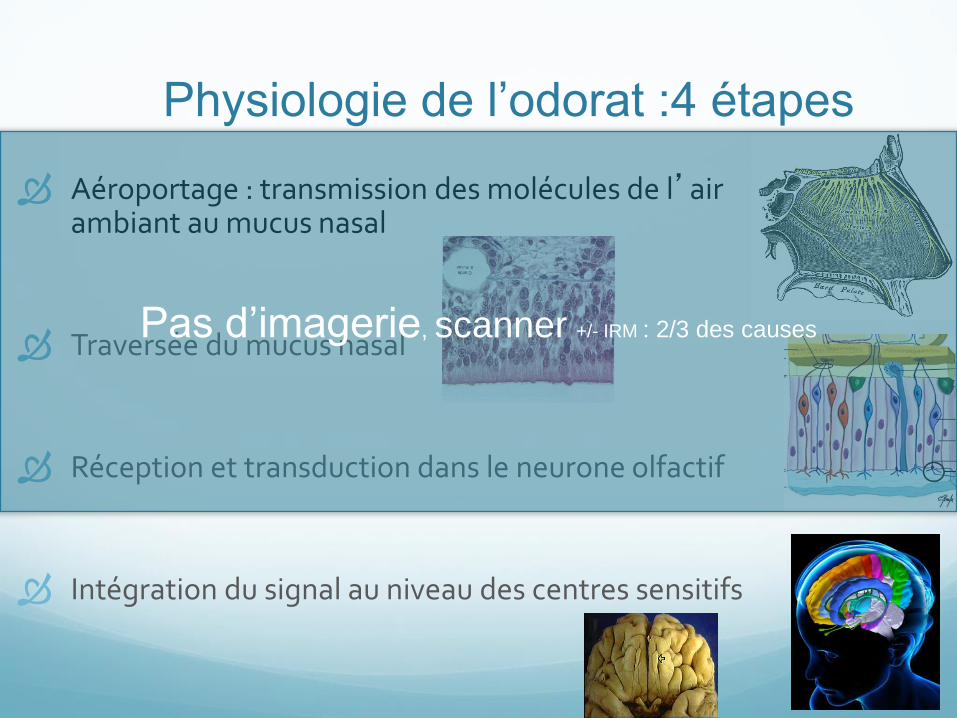
Physiologie de l’odorat :4 étapes
Aéroportage : transmission des molécules de l’air ambiant au mucus nasal
Traversée du mucus nasal
Réception et transduction dans le neurone olfactif
Intégration du signal au niveau des centres sensitifs
Pas d’imagerie, scanner +/- IRM : 2/3 des causes
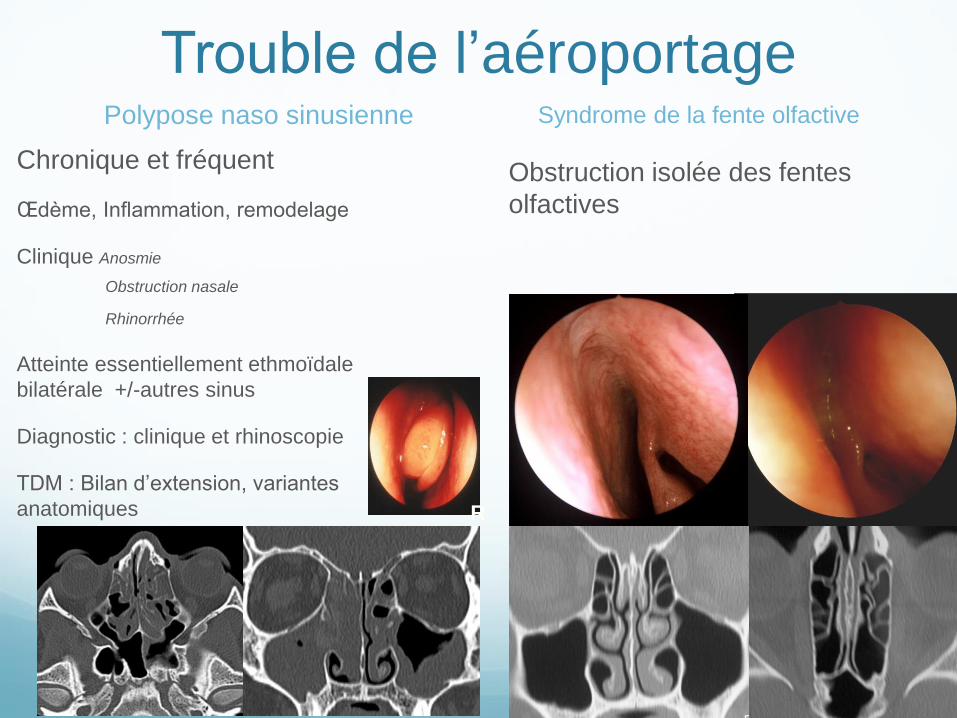
Trouble de l’aéroportage
Chronique et fréquent
Œdème, Inflammation, remodelage
Clinique Anosmie
Obstruction nasale
Rhinorrhée
Atteinte essentiellement ethmoïdale
bilatérale +/-autres sinus
Diagnostic : clinique et rhinoscopie
TDM : Bilan d’extension, variantes
anatomiques
Syndrome de la fente olfactive
Obstruction isolée des fentes
olfactives
R
Polypose naso sinusienne
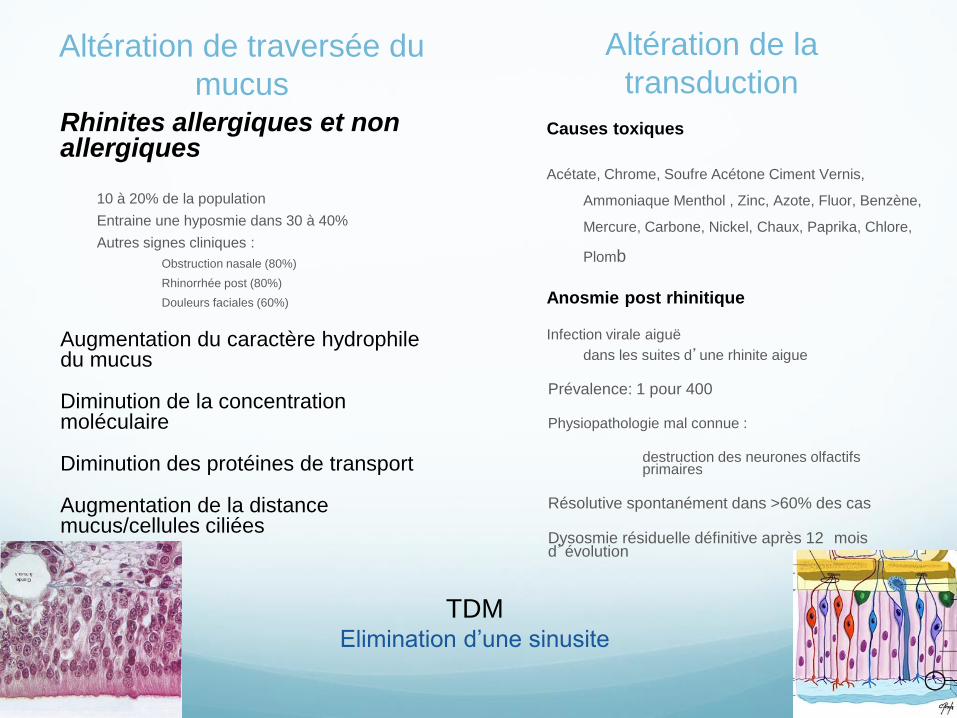
Altération de traversée du
mucus Rhinites allergiques et non allergiques
10 à 20% de la population
Entraine une hyposmie dans 30 à 40%
Autres signes cliniques :
Obstruction nasale (80%)
Rhinorrhée post (80%)
Douleurs faciales (60%)
Augmentation du caractère hydrophile du mucus
Diminution de la concentration moléculaire
Diminution des protéines de transport
Augmentation de la distance mucus/cellules ciliées
Causes toxiques
Acétate, Chrome, Soufre Acétone Ciment Vernis,
Ammoniaque Menthol , Zinc, Azote, Fluor, Benzène,
Mercure, Carbone, Nickel, Chaux, Paprika, Chlore,
Plomb
Anosmie post rhinitique
Infection virale aiguë
dans les suites d’une rhinite aigue
Prévalence: 1 pour 400
Physiopathologie mal connue :
destruction des neurones olfactifs primaires
Résolutive spontanément dans >60% des cas
Dysosmie résiduelle définitive après 12 mois d’évolution
TDM Elimination d’une sinusite
Altération de la
transduction

Femme de 70 ans
Céphalées
Anosmie
TTT corticoïdes AB
ESTHÉSIONEUROBLASTOME
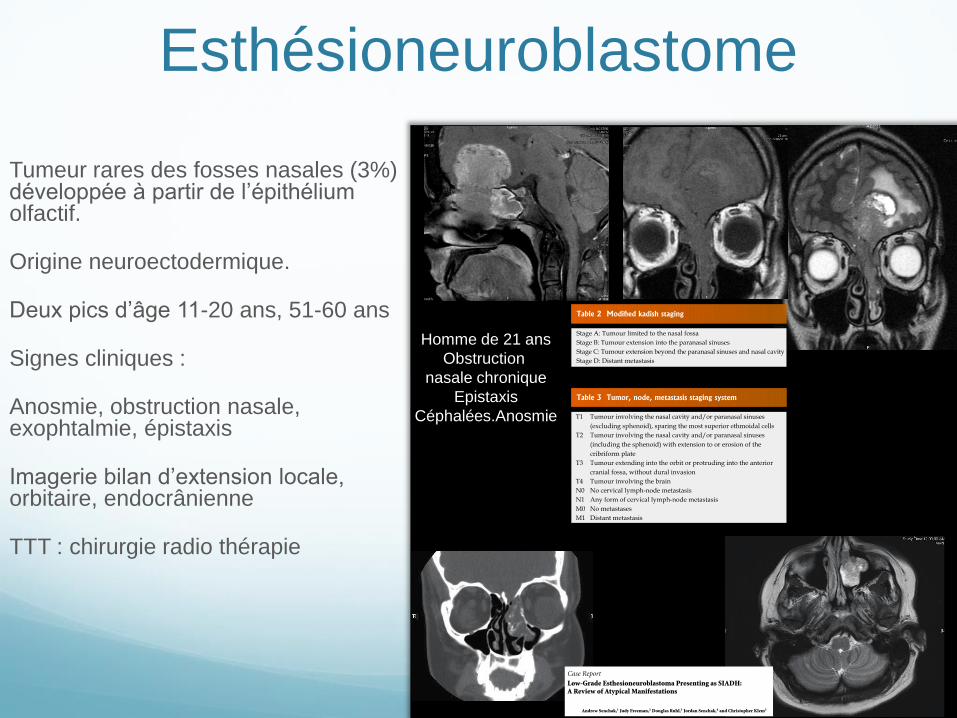
Esthésioneuroblastome
Tumeur rares des fosses nasales (3%) développée à partir de l’épithélium olfactif.
Origine neuroectodermique.
Deux pics d’âge 11-20 ans, 51-60 ans
Signes cliniques :
Anosmie, obstruction nasale, exophtalmie, épistaxis
Imagerie bilan d’extension locale, orbitaire, endocrânienne
TTT : chirurgie radio thérapie
Homme de 21 ans
Obstruction
nasale chronique
Epistaxis
Céphalées.Anosmie
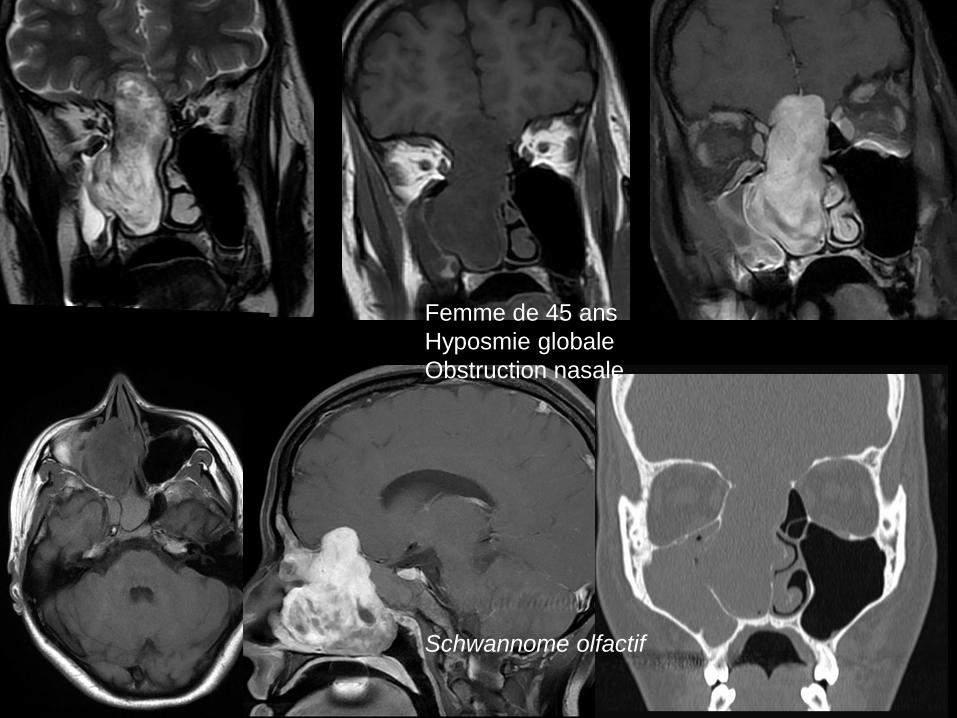
Femme de 45 ans
Hyposmie globale
Obstruction nasale
Schwannome olfactif
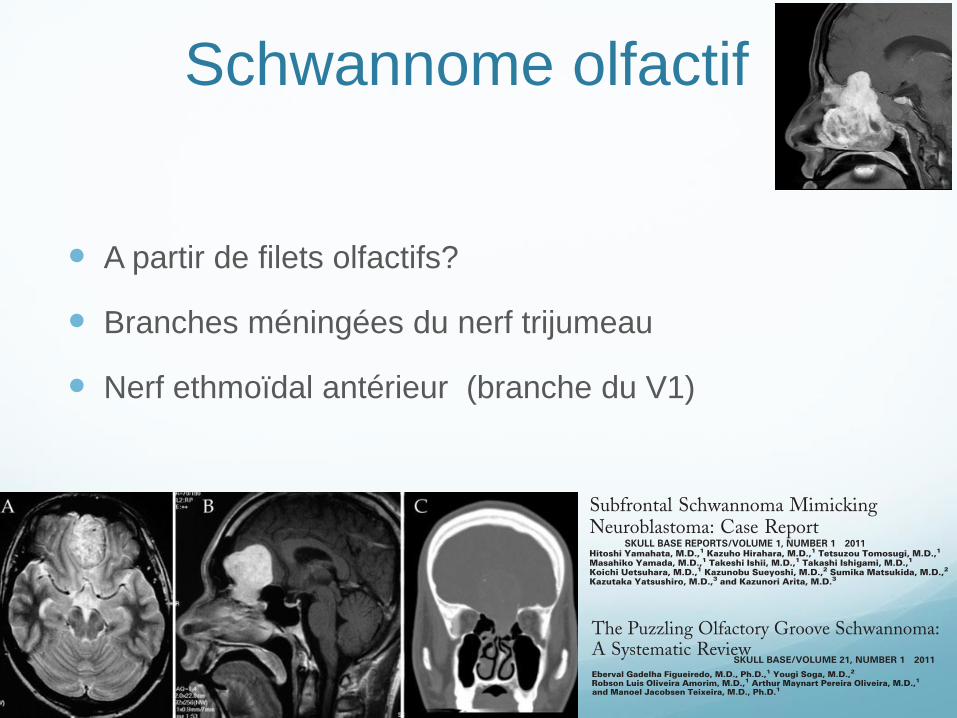
Schwannome olfactif
A partir de filets olfactifs?
Branches méningées du nerf trijumeau
Nerf ethmoïdal antérieur (branche du V1)

Physiologie de l’odorat :4 étapes
Aéroportage : transmission des molécules de l’air ambiant au mucus nasal
Traversée du mucus nasal
Réception et transduction dans le neurone olfactif
Intégration du signal au niveau des centres sensitifs
IRM : 1/3 des causes
Altération des voies et centres
olfactifs Exploration IRM
Encéphalique
Flair, T2*, diffusion
Massif facial
Frontale T2
Echo de spin : coupes max de 2mm
T2 HR (Ciss, Fiesta, Drive,)
Volume T2 (cube, space..)
Injection si nécessaire
les Causes
Malformations
Traumatismes
Tumeurs
Pathologie dégénérative ou
inflammatoire

SYNDROME DE KALLMANN Hypogonadisme hypogonadotrope
par déficit en GnRH
micropénis et cryptorchidie chez le jeune garçon
Anosmie ou hyposmie
(avec hypoplasie ou aplasie des bulbes olfactifs)
Défaut du développement embryonnaire du système
olfactif
Prédominance des cas sporadiques
3 modes de transmission familiale : Récessif lié à l’X;
autosomique récessif , autosomique dominant
1 gène identifié : KAL-1, responsable de la forme récessive
liée à l’X
1 protéine : l’anosmine 1
Disponible en ligne sur
ScienceDirectwww.sciencedirect.com
Annales d’Endocrinologie 78 (2017) 455–461
Original article
Reconsidering olfactory bulb magnetic resonance patterns in
Kallmann syndrome
La neuroradiologie des bulbes olfactifs dans le syndrome de Kallmann revisitée
Thomas Hacquart a,b, Aïcha Ltaief-Boudrigua b, Cécile Jeannerod c, Salem Hannoun d,
Gérald Raverot e, Michel Pugeat e, Aude Brac de la Perriere e, Véronique Lapras f,
Frédérique Nugues g, Catherine Dode h, Francois Cotton a,f,i,∗
a Département universitaire d’anatomie de Rockefeller, UFR médecine Lyon-Est, 8, avenue Rockefeller, 69373 Lyon, Franceb Radiologie ostéo-articulaire et neuroradiologie, groupement hospitalier Edouard-Herriot, hospices civils de Lyon, 5, place d’Arsonval, 69437 Lyon, France
c UFR médecine Lyon-Est, 8, avenue Rockefeller, 69373 Lyon, Franced Abu-Haidar neuroscience institute, faculty of medicine, american university of Beirut, 11-0236 Riad-El-Solh, 1107 2020 Beirut, Lebanon
e Fédération d’endocrinologie, groupement hospitalier Est, hospices civils de Lyon, 59, boulevard Pinel, 69500 Bron, Francef Service de radiologie, centre hospitalier Lyon-Sud, hospices civils de Lyon, 165, chemin du Grand-Revoyet, 69495 Pierre-Bénite, France
g Imagerie pédiatrique, hôpital couple-enfant, CHU de Grenoble, boulevard de la Chantourne, 38700 La Tronche, Franceh Laboratoire de biochimie et génétique moléculaire, hôpital Cochin, APHP, université Paris-Descartes, 27, rue du Faubourg Saint-Jacques,
75014 Paris, Francei CREATIS, CNRS UMR 5220 Inserm U1044, université Lyon 1, 7, avenue Jean-Capelle, 69621 Villeurbanne, France
Abstract
Objective. – The aim of this retrospective study was to perform magnetic resonance imaging assessment of olfactory pathway and skull base
abnormalities in Kallmann syndrome (KS) patients with hypogonadotropic hypogonadism and olfaction disorder. Methods. – Magnetic resonance
brain patterns were retrospectively studied in 19 patients clinically classified as KS. Qualitative assessment of olfactory bulb region comprised bulb
atrophy and rectus and medial orbital gyrus ptosis; quantitative assessment measured olfactory fossa depth and width, sulcus depth and ethmoid
angle. Results were compared to an age- and sex-matched control population (n = 19) with no impairment in the region of interest. Sixteen of
the 19 KS patients were genetically screened for mutations associated with KS. Results. – On the above qualitative criteria, 15 of the 19 patients
presented either unilateral (n = 2) or bilateral (n = 13) olfactory bulb agenesis; 16 showed tract agenesis and 16 showed gyrus malformation (ptosis
or absence). On the quantitative criteria, 18 of the 19 patients showed abnormal sulcus depth and/or olfactory fossa malformation and/or abnormal
ethmoid angle. Conclusion. – The presence of malformation abnormalities in the olfactory fossae of 18 of the 19 patients appears to be a key factor
for etiological diagnosis of hypogonadotropic hypogonadism, and should enable targeted study of genes involved in KS.
© 2017 Elsevier Masson SAS. All rights reserved.
Keywords: Kallmann syndrome; Hypogonadism; Olfactory bulb; Olfaction Disorder; Magnetic resonance imaging
Résumé
Objectif. – L’objectif de cette étude rétrospective était d’évaluer par l’imagerie par résonance magnétique (IRM) les anomalies des voies olfactives
et de la base du crâne chez les patients atteints d’hypogonadisme hypogonadotrope avec anosmie dans le cadre du syndrome de Kallmann.
Méthodes. – Nous avons réalisé une relecture des IRM cérébrales de 19 patients atteints cliniquement d’un syndrome de Kallmann avec une
évaluation qualitative (atrophie des bulbes, ptose de gyri-orbitaire médian et rectus) et quantitative (largeur et hauteur des fosses olfactives, angles
ethmoïdaux, profondeur des sulci olfactifs) de la région des bulbes olfactifs en comparaison avec une population contrôle appariée pour l’âge et le
sexe et sans atteinte de cette région (n = 19). Une étude génétique a pu être réalisée chez 16/19 des patients Kallmann. Résultats. – Sur les 19 patients,
∗ Corresponding author. Service de radiologie, centre hospitalier Lyon-Sud – hospices civils de Lyon, 165, chemin du Grand-Revoyet, 69495 Pierre-Bénite,
France.
E-mail address: [email protected] (F. Cotton).
http://dx.doi.org/10.1016/j.ando.2016.12.003
0003-4266/© 2017 Elsevier Masson SAS. All rights reserved.
Disponible en ligne sur
ScienceDirectwww.sciencedirect.com
Annales d’Endocrinologie 78 (2017) 455–461
Original article
Reconsidering olfactory bulb magnetic resonance patterns in
Kallmann syndrome
La neuroradiologie des bulbes olfactifs dans le syndrome de Kallmann revisitée
Thomas Hacquart a,b, Aïcha Ltaief-Boudrigua b, Cécile Jeannerod c, Salem Hannoun d,
Gérald Raverot e, Michel Pugeat e, Aude Brac de la Perriere e, Véronique Lapras f,
Frédérique Nugues g, Catherine Dode h, Francois Cotton a,f,i,∗
a Département universitaire d’anatomie de Rockefeller, UFR médecine Lyon-Est, 8, avenue Rockefeller, 69373 Lyon, Franceb Radiologie ostéo-articulaire et neuroradiologie, groupement hospitalier Edouard-Herriot, hospices civils de Lyon, 5, place d’Arsonval, 69437 Lyon, France
c UFR médecine Lyon-Est, 8, avenue Rockefeller, 69373 Lyon, Franced Abu-Haidar neuroscience institute, faculty of medicine, american university of Beirut, 11-0236 Riad-El-Solh, 1107 2020 Beirut, Lebanon
e Fédération d’endocrinologie, groupement hospitalier Est, hospices civils de Lyon, 59, boulevard Pinel, 69500 Bron, Francef Service de radiologie, centre hospitalier Lyon-Sud, hospices civils de Lyon, 165, chemin du Grand-Revoyet, 69495 Pierre-Bénite, France
g Imagerie pédiatrique, hôpital couple-enfant, CHU de Grenoble, boulevard de la Chantourne, 38700 La Tronche, Franceh Laboratoire de biochimie et génétique moléculaire, hôpital Cochin, APHP, université Paris-Descartes, 27, rue du Faubourg Saint-Jacques,
75014 Paris, Francei CREATIS, CNRS UMR 5220 Inserm U1044, université Lyon 1, 7, avenue Jean-Capelle, 69621 Villeurbanne, France
Abstract
Objective. – The aim of this retrospective study was to perform magnetic resonance imaging assessment of olfactory pathway and skull base
abnormalities in Kallmann syndrome (KS) patients with hypogonadotropic hypogonadism and olfaction disorder. Methods. – Magnetic resonance
brain patterns were retrospectively studied in 19 patients clinically classified as KS. Qualitative assessment of olfactory bulb region comprised bulb
atrophy and rectus and medial orbital gyrus ptosis; quantitative assessment measured olfactory fossa depth and width, sulcus depth and ethmoid
angle. Results were compared to an age- and sex-matched control population (n = 19) with no impairment in the region of interest. Sixteen of
the 19 KS patients were genetically screened for mutations associated with KS. Results. – On the above qualitative criteria, 15 of the 19 patients
presented either unilateral (n = 2) or bilateral (n = 13) olfactory bulb agenesis; 16 showed tract agenesis and 16 showed gyrus malformation (ptosis
or absence). On the quantitative criteria, 18 of the 19 patients showed abnormal sulcus depth and/or olfactory fossa malformation and/or abnormal
ethmoid angle. Conclusion. – The presence of malformation abnormalities in the olfactory fossae of 18 of the 19 patients appears to be a key factor
for etiological diagnosis of hypogonadotropic hypogonadism, and should enable targeted study of genes involved in KS.
© 2017 Elsevier Masson SAS. All rights reserved.
Keywords: Kallmann syndrome; Hypogonadism; Olfactory bulb; Olfaction Disorder; Magnetic resonance imaging
Résumé
Objectif. – L’objectif de cette étude rétrospective était d’évaluer par l’imagerie par résonance magnétique (IRM) les anomalies des voies olfactives
et de la base du crâne chez les patients atteints d’hypogonadisme hypogonadotrope avec anosmie dans le cadre du syndrome de Kallmann.
Méthodes. – Nous avons réalisé une relecture des IRM cérébrales de 19 patients atteints cliniquement d’un syndrome de Kallmann avec une
évaluation qualitative (atrophie des bulbes, ptose de gyri-orbitaire médian et rectus) et quantitative (largeur et hauteur des fosses olfactives, angles
ethmoïdaux, profondeur des sulci olfactifs) de la région des bulbes olfactifs en comparaison avec une population contrôle appariée pour l’âge et le
sexe et sans atteinte de cette région (n = 19). Une étude génétique a pu être réalisée chez 16/19 des patients Kallmann. Résultats. – Sur les 19 patients,
∗ Corresponding author. Service de radiologie, centre hospitalier Lyon-Sud – hospices civils de Lyon, 165, chemin du Grand-Revoyet, 69495 Pierre-Bénite,
France.
E-mail address: [email protected] (F. Cotton).
http://dx.doi.org/10.1016/j.ando.2016.12.003
0003-4266/© 2017 Elsevier Masson SAS. All rights reserved.

TRAUMATISME
3ème cause de dysosmie
30% des traumatisés crâniens graves
5% des traumatisés crâniens légers.
Prévalence augmente si TC sévère, si
TC associé à un trauma maxillo-facial
Peut être lié à un trauma occipital
Lésions de cisaillement ou section des
axones au niveau de la lame criblée
Lésions des bulbes olfactifs.
Contusions frontales inférieures

Méningiome olfactif

Bulbes olfactifs, HPN, HTIC Structural Olfactory Nerve Changes in Patients Sufferingfrom Idiopathic Intracranial Hypertension
Christoph Schmidt1. , Edzard Wiener1. , Jan Hoffmann2, Randolf Klingeb iel1, Fel ix Schmidt 2,
Tobias Hofmann3, Lutz Harms2, Hagen Kunte2*
1 Institute of Radiology, Charit e-Universitatsmedizin Berlin, Berlin, Germany, 2 Department of Neurology, Charite-Universitatsmedizin Berlin, Berlin, Germany,
3 Department of Psychosomatic Medicine, Charite-Universitatsmedizin Berlin, Berlin, Germany
Abst ract
Background: Complications of idiopathic intracranial hypertension (IIH) are usually caused by elevated intracranial pressure(ICP). In a similar way as in the optic nerve, elevated ICP could also compromise the olfactory nerve system. On the otherside, there is growing evidence that an extensive lymphatic network system around the olfactory nerves could be disturbedin cerebrospinal fluid disorders like IIH. The hypothesis that patients with IIH suffer from hyposmia has been suggested inthe past. However, this has not been proven in clinical studies yet. This pilot study investigates whether structural changesof the olfactory nerve system can be detected in patients with IIH.
Methodology/Principal Findings: Twenty-three patients with IIH and 23 matched controls were included. Olfactory bulbvolume (OBV) and sulcus olfactorius (OS) depth were calculated by magnetic resonance techniques. While mean values oftotal OBV (128.76 38.4 vs. 130.06 32.6 mm3, p = 0.90) and mean OSdepth (8.56 1.2 vs. 8.66 1.1 mm, p = 0.91) were similar inboth groups, Pearson correlation showed that patients with a shorter medical history IIH revealed a smaller OBV (r = 0.53,p, 0.01). In untreated symptomatic patients (n = 7), the effect was greater (r = 0.76, p, 0.05). Patients who suffered from IIHfor less than one year (n = 8), total OBV was significantly smaller than in matched controls (116.66 24.3 vs. 149.36 22.2 mm3,p= 0.01). IIH patients with visual disturbances (n = 21) revealed a lower OS depth than patients without (8.36 0.9 vs.10.86 1.0 mm, p, 0.01).
Conclusions/Significance: The results suggest that morphological changes of the olfactory nerve system could be presentin IIH patients at an early stage of disease.
Citat ion: Schmidt C, Wiener E, Hoffmann J, Klingebiel R, Schmidt F, et al. (2012) Structural Olfactory Nerve Changes in Patients Suffering from IdiopathicIntracranial Hypertension. PLoS ONE 7(4): e35221. doi:10.1371/journal.pone.0035221
Editor: Kewei Chen, Banner Alzheimer’s Institute, United States of America
Received October 29, 2011; Accepted March 13, 2012; Published April 6, 2012
Copyright : ß 2012 Schmidt et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: No current external funding sources for this study.
Compet ing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
. These authors contributed equally to this work.
Int roduct ion
Idiopathic intracranial hypertension (IIH) is characterized by
increased intracranial pressure (ICP) and isaffecting mainly obese
women of childbearing age. The aetiology of the disorder is not
well understood but disturbed cerebrospinal fluid (CSF) dynamics
are assumed to be an important factor. Affected patients mostly
suffer from chronic disabling headache and other symptoms of
elevated ICP like visual disturbance, tinnitus and diplopia.
Impairment of visual function is often progressive and permanent
in up to 25% of all cases [1,2,3].
Similar to the optic nerve, the olfactory nerve (ON) is covered
by a meningeal sheath enclosing the subarachnoidal space.
Elevated intracranial pressure (ICP) is a characteristic feature of
IIH and could damage the olfactory nerves (ONs) directly by
mechanical impact. There are also case reports about nasal liquor
leakage in IIH patients [4,5]. The authors argue that an increased
ICP may break the nerve sheaths around the olfactory nerves that
allow for liquor passage via the cribriform plate. In addition, there
is growing evidence that an extensive lymphatic network system
around the ONs could play a role in CSF absorption. The
pathway of CSF absorption leads along the ONs and the
absorbing acting system is located in the submucosal space
associated with the nasal olfactory and respiratory epithelium [6].
The hypothesis that patients with IIH suffer from hyposmia has
been suggested by Kapoor [7]. Giuseffi and colleagues reported
that up to 25% of IIH patients complain about decreased smell
[8]. This assumption is clinically relevant, since undetected and
therefore untreated olfactory disordersare associated with reduced
quality of life and problems with daily life situations [9,10].
Furthermore, patients with hyposmia are at higher risk to develop
depression [11]. However, to the best of our knowledge, clinical
studies investigating the ON system in patients with IIH have not
been reported in the literature.
Decreased olfactory function is mostly associated with reduced
olfactory bulb volume (OBV) [12,13,14,15]. Buschhuter et al.
investigated a large cohort of normal volunteers and defined
normative values for minimal-normal OBV as 58 mm3 in people
, 45 years and as 46 mm3 in people . 45 years [15]. The
importance of the determination of the depth of olfactory sulcus
PLoS ONE | www.plosone.org 1 April 2012 | Volume 7 | Issue 4 | e35221
Structural Olfactory Nerve Changes in Patients Sufferingfrom Idiopathic Intracranial Hypertension
Christoph Schmidt1. , Edzard Wiener1. , Jan Hoffmann2, Randolf Klingebiel1, Felix Schmidt 2,
Tobias Hofmann3, Lutz Harms2, Hagen Kunte2*
1 Institute of Radiology, Charite-Universitatsmedizin Berlin, Berlin, Germany, 2 Department of Neurology, Charite-Universitatsmedizin Berlin, Berlin, Germany,
3 Department of Psychosomatic Medicine, Charite-Universitatsmedizin Berlin, Berlin, Germany
Abstract
Background: Complications of idiopathic intracranial hypertension (IIH) are usually caused by elevated intracranial pressure(ICP). In a similar way as in the optic nerve, elevated ICP could also compromise the olfactory nerve system. On the otherside, there isgrowing evidence that an extensive lymphatic network system around the olfactory nerves could be disturbedin cerebrospinal fluid disorders like IIH. The hypothesis that patients with IIH suffer from hyposmia has been suggested inthe past. However, this has not been proven in clinical studies yet. This pilot study investigates whether structural changesof the olfactory nerve system can be detected in patients with IIH.
Methodology/Principal Findings: Twenty-three patients with IIH and 23 matched controls were included. Olfactory bulbvolume (OBV) and sulcus olfactorius (OS) depth were calculated by magnetic resonance techniques. While mean values oftotal OBV(128.76 38.4 vs. 130.06 32.6 mm3, p=0.90) and mean OSdepth (8.56 1.2 vs. 8.66 1.1 mm, p=0.91) were similar inboth groups, Pearson correlation showed that patients with a shorter medical history IIH revealed a smaller OBV (r=0.53,p, 0.01). In untreated symptomatic patients (n=7), the effect was greater (r=0.76, p, 0.05). Patients who suffered from IIHfor less than one year (n= 8), total OBVwassignificantly smaller than in matched controls (116.66 24.3 vs. 149.36 22.2 mm3,p=0.01). IIH patients with visual disturbances (n= 21) revealed a lower OS depth than patients without (8.36 0.9 vs.10.86 1.0 mm, p, 0.01).
Conclusions/Significance: The results suggest that morphological changes of the olfactory nerve system could be presentin IIH patients at an early stage of disease.
Citation: Schmidt C, Wiener E, Hoffmann J, Klingebiel R, Schmidt F, et al. (2012) Structural Olfactory Nerve Changes in Patients Suffering from IdiopathicIntracranial Hypertension. PLoSONE7(4): e35221. doi:10.1371/journal.pone.0035221
Editor: Kewei Chen, Banner Alzheimer’s Institute, United States of America
Received October 29, 2011; Accepted March 13, 2012; Published April 6, 2012
Copyright: ß 2012 Schmidt et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: No current external funding sources for this study.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
. These authors contributed equally to this work.
Introduction
Idiopathic intracranial hypertension (IIH) is characterized by
increased intracranial pressure (ICP) and isaffecting mainly obese
women of childbearing age. The aetiology of the disorder is not
well understood but disturbed cerebrospinal fluid (CSF) dynamics
are assumed to be an important factor. Affected patients mostly
suffer from chronic disabling headache and other symptoms of
elevated ICP like visual disturbance, tinnitus and diplopia.
Impairment of visual function isoften progressive and permanent
in up to 25% of all cases [1,2,3].
Similar to the optic nerve, the olfactory nerve (ON) is covered
by a meningeal sheath enclosing the subarachnoidal space.
Elevated intracranial pressure (ICP) is a characteristic feature of
IIH and could damage the olfactory nerves (ONs) directly by
mechanical impact. There are also case reportsabout nasal liquor
leakage in IIH patients [4,5]. Theauthorsargue that an increased
ICP may break thenerve sheathsaround theolfactory nervesthat
allow for liquor passage via thecribriform plate. In addition, there
is growing evidence that an extensive lymphatic network system
around the ONs could play a role in CSF absorption. The
pathway of CSF absorption leads along the ONs and the
absorbing acting system is located in the submucosal space
associated with the nasal olfactory and respiratory epithelium [6].
The hypothesis that patients with IIH suffer from hyposmia has
been suggested by Kapoor [7]. Giuseffi and colleagues reported
that up to 25% of IIH patients complain about decreased smell
[8]. This assumption is clinically relevant, since undetected and
thereforeuntreated olfactory disordersareassociated with reduced
quality of life and problems with daily life situations [9,10].
Furthermore, patientswith hyposmia are at higher risk to develop
depression [11]. However, to the best of our knowledge, clinical
studies investigating the ON system in patients with IIH have not
been reported in the literature.
Decreased olfactory function is mostly associated with reduced
olfactory bulb volume (OBV) [12,13,14,15]. Buschhuter et al.
investigated a large cohort of normal volunteers and defined
normative values for minimal-normal OBV as 58 mm3 in people
, 45 years and as 46 mm3 in people . 45 years [15]. The
importance of the determination of the depth of olfactory sulcus
PLoSONE | www.plosone.org 1 April 2012 | Volume 7 | Issue 4 | e35221
(OS) is less well known. Previous work has indicated a correlation
between reduced olfactory function and smaller depth of OS in
patients with olfactory dysfunction since birth or early childhood
[16]. Wang and colleagues have demonstrated that the OS depth
is reduced in patients with Parkinson disease [17].
The aim of our pilot study was to investigate OBV and OS
depth to verify if the ON system is affected in IIH.
Methods
Patients fulfilling the modified Dandy criteria for IIH [18] and
an age over 18 years were screened using the hospital’s electronic
medical records system. Patients with any secondary cause of
intracranial hypertension were not eligible for inclusion in the
study. Screening period was from November 2005 until May
2010. Approval for this study was obtained from the institutional
ethics committee (Ethikausschuss 1, Charite Campus Mitte).
Written informed consent was obtained from all participants
before enrolment in the study. All clinical investigations have been
conducted according to theprinciplesexpressed in theDeclaration
of Helsinki. Seventy-one patients were potentially eligible to be
included in the study. Altogether 15 patients were excluded by the
exclusion criteria shunt surgery (n = 6), body weight over 180 kg
(n = 3), pregnancy (n = 1), and magnetic resonance imaging (MRI)
phobia (n = 4). One patient fulfilled the criteria for major
depression (diagnosed by the Becks Depression Inventory andHamilton Rating Scale for Depression) and was excluded.
Eighteen patients could not be reached by phone, eight patients
refused because effort of participation in the study wastoo high for
them, and seven subjects objected to participation without
specifying any reasons. All participants underwent clinical
examination to detect olfactory disorders with a different genesis
(e.g. post-infectious, post-traumatic, current sinunasal or upper
respiratory tract infections, tumors treated with radiation orchemotherapy, allergies, depression) at the Special Consulting
Service for Olfactory Disorders at the ENT-Department of the
Charite University in Berlin, Germany. Altogether, 23 patients
could be included in the study.
Each patient with IIH was matched with a control patient for
sex, age and body massindex (BMI). Controlswereselected from a
local obesity center and from the hospital staff. Subjects with
known history of CNS disease or episodes of continuous orrecurring headache syndromes were not eligible to be included in
the control group.
MRI was performed with a 1.5 T scanner (Siemens, Magne-
tom). MRI was obtained to exclude intracranial pathology andsinusvein thrombosisasa secondary cause of IIH. A commerciallyavailable surface coil (Siemens) with a diameter of 7 cm was used
in addition to the normal circularly polarized head coil. Thesurface coil wasplaced over one eye within the head coil and fixedwith tape. T2-weighted high-resolution coronal images were
acquired with the surface coil. A fast spin echo (FSE) sequencewith a relaxation time of 6960 msec, an echo time of 99 msec, a
field of view of 856 85 mm2, a matrix size of 2566 256 mm2 (inplane resolution 3326 332 mm2) and a slice thickness of 2 mm
were performed. The measured time scale was 7 minutes and20 seconds. The OBV as well as the OS depth were determined
using a standardized method [19]. Computer software Amira 3.2was used to calculate quantitative morphological parameters.
OBV was investigated by circumnavigating the bulb contours ofall coronal slices starting from the anterior to the posterior border
of the olfactory bulb. The slice thickness was 2 mm, therefore theOBV could be calculated using the surface areas of each coronal
section through the olfactory bulb (surface area of each coronalsection in mm26 count of sections6 2 mm). The OS depth was
identified at the level of the last coronal slice through the rearmostpart of the eyeball. The depth of the OS was then calculated by
drawing a straight line tangent to the borders of the straight gyrusand internal orbital gyrus. From this line an intergyral line to the
deepest point of the OSdetermined the OSdepth (Figure 1). MRIstudy readerswere blinded to the status and clinical characteristics
of the participating subjects to prevent observer-dependent bias.
Data were presented asmean 6 standard deviation (range) or asmedian (range), if they were not normally distributed. The chi-
square test and independent t-test were used to analyse differencesbetween IIH patients and controls. To determine age-dependent
normal OBV, data proposed by Buschhuter et al. ($ 58 mm3 inpeople , 45 years and $ 46 mm3 in people . 45 years) were used
[15]. Relationships among clinical features of IIH patients, theOBV, and the depth of OS were examined by using Pearsoncorrelation coefficient r. A difference was considered significant at
a p-value of , 0.05.
Figure 1. T2-weighted high-resolut ion coronal images of the olfactory bulb and sulcus olfactorius. Figure 1A and 1Bshow T2-weightedfast spin echo (FSE) sequences. In Figure 1A the white arrows indicate the normal dimensioned right and left bulb olfactorius. Figure 1Bdemonstratesthe calculation of the olfactory sulcus (OS) depth. The distance of the deepest point of the OSwas determined using a tangent line from the border ofthe gyrus rectus to the internal orbital gyrus.doi:10.1371/journal.pone.0035221.g001
Structural Olfactory Nerve Changes in IIH Patients
PLoS ONE | www.plosone.org 2 April 2012 | Volume 7 | Issue 4 | e35221
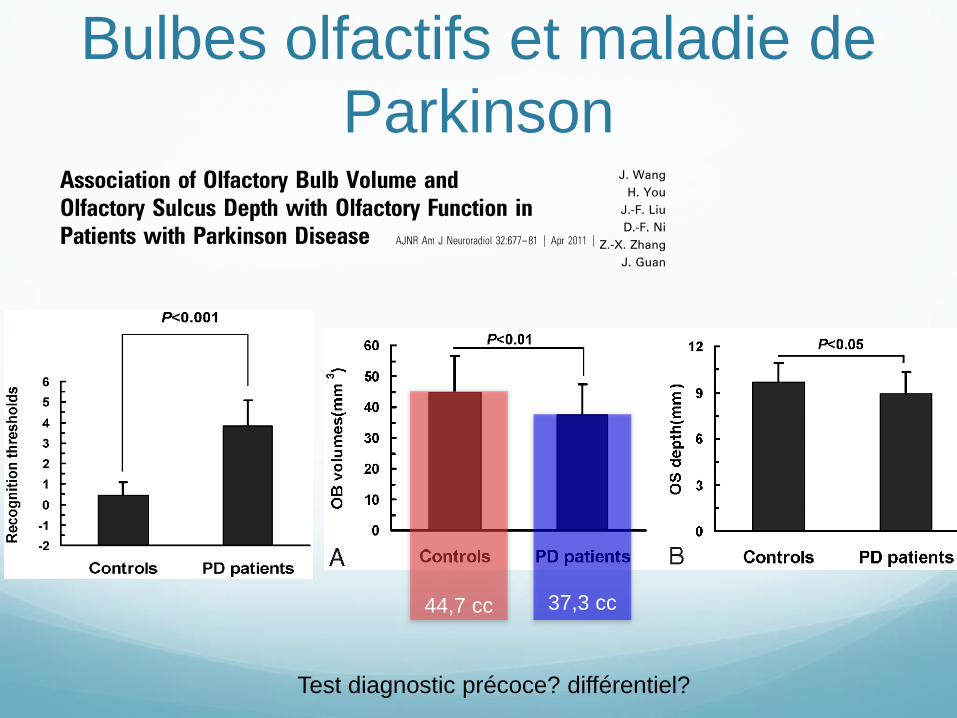
Bulbes olfactifs et maladie de
Parkinson
44,7 cc
37,3 cc
Test diagnostic précoce? différentiel?
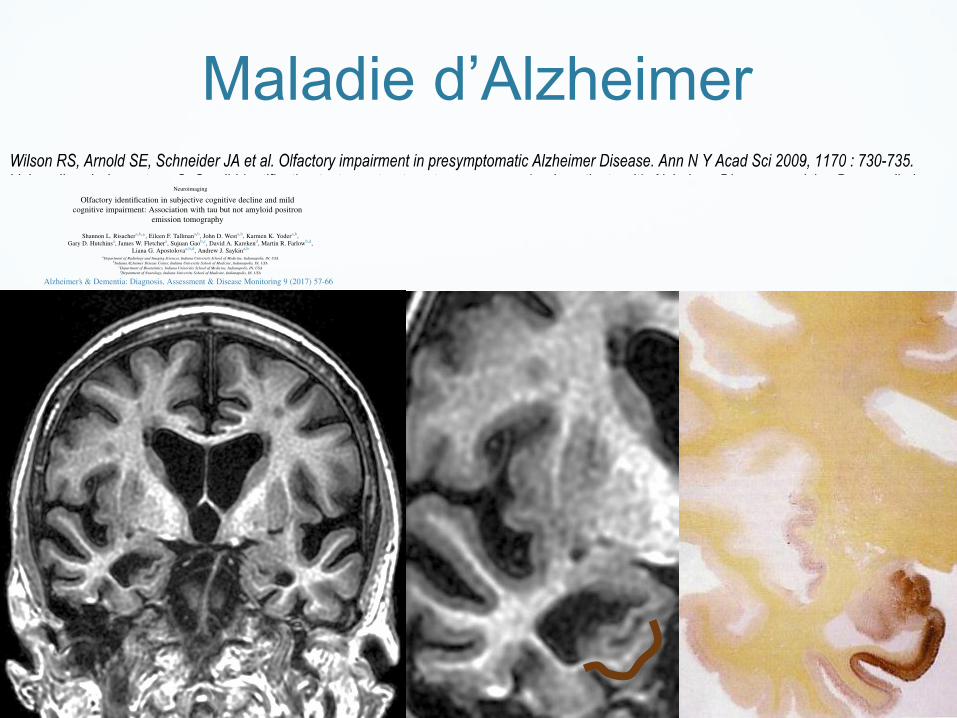
Maladie d’Alzheimer

Epilepsie
HOMME DE 27 ANS
Crises olfactives
Cacosmie.
Gangliogliome Sclérose mésiale

Olfaction et dépression
EVALUATION OF OLFACTORY FUNCTIONAL MRI IN MAJOR
DEPRESSIVE PATIENTS BEFORE AND AFTER TREATMENT
Hibat-Allah S., Tran Dong K., Skeif H., Gressier F., Corruble E., Coui llet A., Ducreux D.
Neuroradiology department, Kremlin Bicêtre Hospital, 94, France.
ABSTRACT
Introduction. Olfactory disorders have been shown in major depressive patients with
increase sensitivity to unpleasant odors. The aim of our study is to evaluate patients with
major depression after 3 months of treatment using olfactory functional MRI.
Materials and methods. 10 subjects with major depression according to DSM-V criteria
were included during 15 months. Olfactory functional MRI (using BOLD method) was
performed before and after 3 months of treatment. 3 scents were used: spearmint for pleasant
odor, sandalwood for neutral odor and wine lee for unpleasant odor. Data processing and
statistical analysis was executed using matlab software (linear regression and t student test).
We performed individual analysis for every scent for the limbic lobe and for every cluster,
and global analysis.
Results.10 patients were including during 15 months. There were 80% of women with a
medium age of 36.7 years old ± 14.9 (18-65). For the global analysis, 100% of patients show
activation for wine lee versus 80% for spearmint and sandalwood with high Zscore superior to
2. For the individual analysis, after 3 months of treatment, we observe a significant difference
of activation for wine lee scent, for anterior cingulum and para-hippocampic gyrus (p‹0.05
and Zscore › 2).
Conclusion. Olfactory functional MRI shows a significant difference of activation for
unpleasant odors in patients with major depression after 3 months of treatment. The structures
mostly involved in this mechanism seem to be the cingular gyrus with the anterior cingulum.
Pr Denis Ducreux
Figure 5. Difference of activation between spearmint (left) and wine lee (right) in major depressive (21)
Courtesy Pr Ducreux Denis www.fmritools.com/teaching-files/limec-teaching-files/isipca/
10 Patients dépréssifs majeurs
Stimulation par 3 odeurs
menthe : agréable
Bois de santal : neutre
Lie de vin : désagréable
IRMf
Suivi avant et après 3 mois de ttt
Modification des activations
Cingulum antérieur
Menthe Lie de vin

Conclusion
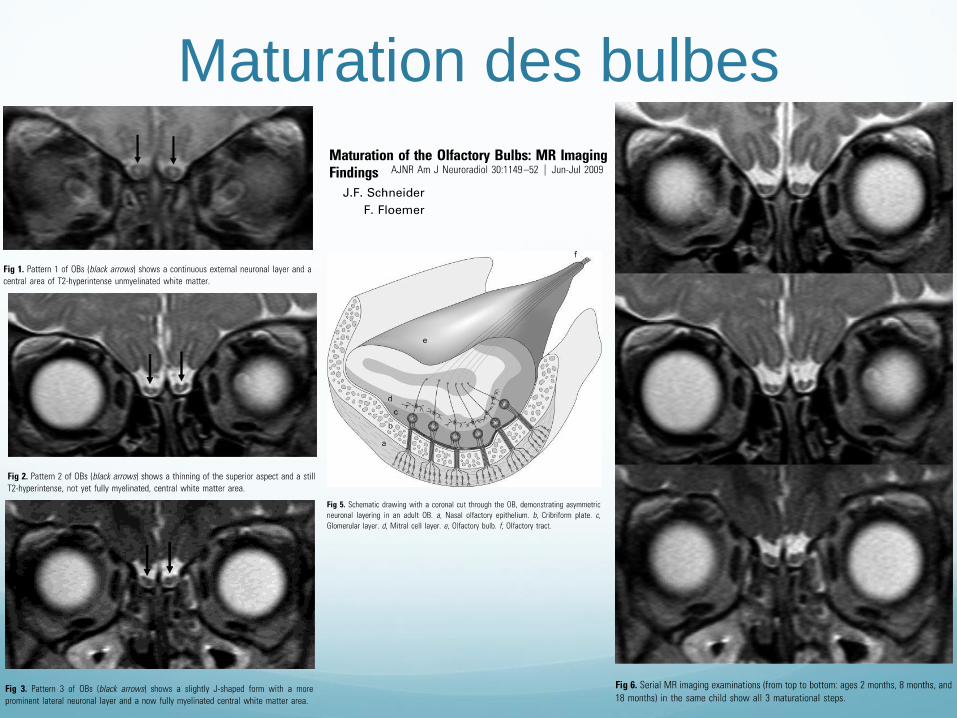
Maturation des bulbes