EP quoi de neuf en 2013 COPACAMU€¦ · UTILITE Age > 65 ans > 85 ans cancer Actif – rémission...
48
Quoi de neuf en 2013 sur le diagnos3c et le traitement de l’embolie pulmonaire au SU ? Pierre-Marie Roy L’UNAM Université d’Angers Département de Médecine d’Urgence CHU Angers
Transcript of EP quoi de neuf en 2013 COPACAMU€¦ · UTILITE Age > 65 ans > 85 ans cancer Actif – rémission...

Quoi de neuf en 2013 sur le diagnos3c et le traitement de l’embolie pulmonaire au SU ?
Pierre-Marie Roy
L’UNAM Université d’Angers Département de Médecine d’Urgence
CHU Angers

Disclosure statement of interest (loi du 4 mars 2002)
2
1 – Titulaire de brevets/Porteur de parts sociales ou membre d’une structure de gouvernance ou salarié
Ø………………………............................ non................
2 – Consultant ou membre d’un Conseil scientifique Ø Sanofi-Aventis, Lilly, Biomérieux, Boehringer-
Ingelheim, GlaxoSmithKline, Bayer Shering Pharma
3 – Conférencier ou auteur/rédacteur rémunéré d’articles ou documents
ØBayer Shering Pharma, Biomérieux, Boehringer-Ingelheim, GlaxoSmithKline, LFB biomédicaments, Lilly, Sanofi-Aventis
4 – Prise en charge de frais de voyages, d’hébergement ou d’inscription à des congrès ou autres manifestations
ØBayer Shering Pharma, Biomérieux, Boehringer-Ingelheim, GlaxoSmithKline, LFB biomédicaments, Lilly, Sanofi-Aventis
5 – Investigateur principal d’une recherche ou d’une étude clinique
ØSanofi-Aventis, Bayer Shering Pharma, GlaxoSmithKline,
6 – Co-Investigateur d’une étude clinique ØGlaxoSmithKline, Bayer Shering Pharma, Boehringer-Ingelheim, LFB biomédicaments, Sanofi-Aventis, Daiichi-Sankyo
Maladie thromboembolique veineuse

Embolie pulmonaire
• Une pathologie fréquente – MTEV : 1,8 / 1000 habitants (Europe et USA) – EP : 0,6 / 1000 habitants
• Une pathologie potenDellement grave
– Evènements cliniques graves à 1 mois : 7,4% (5,5-‐9,8) – Décès à 1 mois : 4,6% (3,1 – 6,6%)
• Un diagnosDc difficile – 70% des décès par EP = diagnosDc non posé
• Un traitement dangereux – 4.9 -‐13,4 % hémorragies graves / paDent-‐année – 0.8 % accidents mortels
Oger E et al. Thromb Haemost 2000 Sanchez O et al. AJRCCM 2010 Stein et al. Am J Cardiol 2004
Linkins et al. Ann Intern Med 2003 Pouyanne et al. BMJ 2000

Des progrès considérables
– Démarche diagnosDque • Probabilité clinique • tests non invasifs • Stratégies combinées simplifiées
– Démarche thérapeuDque • Analyse de risque • Nouveaux traitements
• Stratégies thérapeuDques et d’orientaDon

Des progrès considérables au SU
• Beaucoup de monde… • Beaucoup de symptômes thoraciques • Beaucoup de possibilités • Beaucoup de pression • Peu de temps • Peu de lits

EP ?
D-dimères
Probabilité Echographie veineuse
Scintigraphie
Angioscanner
Echographie cardiaque Angio MR
Capnographie
Fonction rénale
Antécédents
Âge Coût
Place
Radiologue Pneumologue
Cardiologue
Temps Biologiste
EPP accréditation
Irradiation
Ma femme
clinique
RP
Représentante
hémorragies
HBPM
NACO
HNF
Fibrinolyse

Évaluation de la probabilité Clinique
Pas Traitement
CT scan
+
Traitement +Pas Traitement
-
-
Faible Modérée Élevée
D-dimères
Démarche diagnostique
Task Force ESC Eur Heart J 2008

Évaluation de la probabilité Clinique
Pas Traitement
CT scan
+
Traitement +Pas Traitement
-
-
Faible Modérée Élevée
D-dimères
Quoi de neuf en 2013
Task Force ESC Eur Heart J 2008

• Quand suspecter une EP ? • Quid de la probabilité clinique ? • Quand ne pas faire un dosage des D-‐dimères ? • Que faire en dehors du scanner ? • Que faire dans le doute ?
Quoi de neuf en 2013 ?

Quand suspecter une EP ?
RISQUE

Patients Suspects Europe (n=3174)
USA (n=7940)
p
Age (ans) 62.4 49.0 <0.001
Sexe (%F) 58.8 67.1 <0.001
TAS mmHg 141.2 131 <0.001
FC ( /min) 89.9 92.2 <0.001
FR ( /min) 21.7 20.8 <0.001
Sat O2 (%) 94.5 96.5 <0.001
PCO2 (mmHg) 35.6 39.3 <0.001
Malaise (%) 21.1 6 <0.001
Hémoptysie (%) 4.0 2.9 <0.001
Antcd Perso MTE (%) 19.1 10.8 <0.001
Ins cardiaque (%) 13.9 7.3 <0.001
Cancer (%) 7.6 6.2 0.005
EP = diagnostic le + probable(%) 34.5 16.8 <0.001
Diagnostic final EP (%) 26,3 7 <0.001
Pts suspects EP Européens plus de signes de gravité que pts Américain Seuil de suspicion + élevé en Europe
Pénaloza et al. J Thromb Haemost 2011

Pulmonary Embolism Rule out Criteria
Kline JA et al. J Thromb Haemost 2004 Kline JA et al. J Thromb Haemost 2008 Wolf SJ et al. Am J Emerg Med 2008
1 % (0,6 – 1,6)
Règle de PERC Age <50 ans FC <100/’ Saturation O2> 94% Pas de gonflement unilatéral MI Pas hémoptysie Pas chirurgie ou trauma. <4 sem. Pas antcds de MTE Pas de traitement hormonal PO

Pulmonary Embolism Rule out Criteria
Kline JA et al. J Thromb Haemost 2004 Kline JA et al. J Thromb Haemost 2008 Wolf SJ et al. Am J Emerg Med 2008
1 % USA
Règle de PERC Age <50 ans FC <100/’ Saturation O2> 94% Pas de gonflement unilatéral MI Pas hémoptysie Pas chirurgie ou trauma. <4 sem. Pas antcds de MTE Pas de traitement hormonal PO
> 5 % Europe
Hugli et al. J Thromb Haemost 2011

Régle N (%)
Prévalence EP (95%CI)
Suspicion d’EP 929 29.8%
PERC- et suspicion d’EP
74 (7.7%)
5.4% (1.4-12.7)
PERC- et faible suspicion clinique (jugement implicite)
58 (6.0)
(0-5.0) 0%
Penaloza et al. Thromb Research 2012
PERC en Europe

Score de Wells Signes et symptômes de TVP (gonflement et d+) +3.0
Diagnostic différentiel est moins probable que d’EP +3.0
Rythme cardiaque > 100 / min +1.5
Immobilisation ou chirurgie < 4 sem. +1.5
Antcd de TVP et/ou EP +1.5
Hémoptysies +1.0
Cancer actif (traitement en cours, < 6mois ou palliatif) +1.0
Score révisé de Genève (SRG) Age>65 ans +1
Antcd de TVP et/ou EP +3
Immobilisation ou chirurgie < 4 sem +2
Cancer actif (actien , résolu< 1an) +2
Douleur jambe unilatérale +3
Hémoptysies +2
Rythme cardiaque 75-94/’ +3
Rythme cardiaque ≥ 95/’ +5
Douleur à la palpation et œdème unilatéral de jambe +4
Score révisé simplifié de Genève (SRSG) Age>65 ans +1
Antcd de TVP et/ou EP +1
Immobilisation ou chirurgie < 4 sem +1
Cancer actif (actien , résolu< 1an) +1
Douleur jambe unilatérale +1
Hémoptysies +1
Rythme cardiaque 75-94/’ +1
Rythme cardiaque ≥ 95/’ +2
Douleur à la palpation et œdème unilatéral de jambe +1
<2: PC faible 2-6 : PC modérée >6: PC élevée
<2: PC faible 2-4 : PC modérée ≥ 5: PC élevée 0-3: PC faible 4-10:PC modérée ≥ 11: PC élevée
Évaluation Empirique (jugement implicite)
Comment évaluer la PC ?

AUC [95% CI]
Jugement implicite 0.81 [0.78-0.84]
Score de Wells 0.71 [0.68-0.75]
Score révisé de Genève 0.66 [0.63-0.70]
Comment évaluer la PC ?
Penaloza et al. Ann Emerg Med 2012 Roy PM et al. ISTH 2009

PC oui mais pourquoi ?
0% 100%
Kearon et al. ACCP Chest 2012
Probabilité faible
Probabilité modérée
Probabilité forte
6% - 12% 25% - 35% 50% - 75%

Décider d’un traitement d’attente
0% 100%
Kearon et al. ACCP Chest 2012
Probabilité faible
Probabilité modérée
Probabilité forte
6% - 12% 25% - 35% 50% - 75%
Traitement d’attente
systématique
Traitement si délai
> 4 heures
Pas de traitement d’attente

Interpréter le résultat d’un test
0% 100%
Kearon et al. ACCP Chest 2012
Probabilité faible
Probabilité modérée
Probabilité forte
6% - 12% 25% - 35% 50% - 75%
Non décisionnel (FN 10-30%)
Exclusion Possible (FN 3-7%)
Exclusion certaine
(FN 1-3 %)
D-‐dimères NEGATIF (RVN 0,1 – 0,3)

3) Faut-‐il faire (toujours) des D-‐dimères ?
• Pas lorsque la PC est forte ! • Pas lorsque la PC est moyenne et le test est de performance moyenne (RVN> 0,2)
• Pas lorsque le paDent est anDcoagulé • Pas en l’absence de suspicion d’EP
Roy et al. BMJ 2005 ; 331 : 259 Stein et al. Ann Intern Med 2004

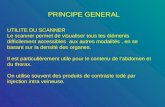
UTILITE
Age > 65 ans > 85 ans
cancer Actif – rémission < 1an multimétastatique
chirurgie mineure majeure
traumatisme mineur majeur
grossesse 2ème trimestre 3ème trimestre
sepsis mineur majeur
Traitement anticoagulant
Righini et al. J Am Geriatr Soc 2005 Righini et al. Thromb Haemost 2006
Nijkeuter et al. Crit Care Med 2006
Faut-‐il faire (toujours) des D-‐dimères ?
Pas lorsque la PC est forte ! Pas lorsque la PC est moyenne et le test est de performance moyenne (RVN> 0,2)
Pas d’étude – pas de seuil validé

Score de per3nence des D-‐dimères
Score D-dimer usefulness Points Sex Female +1 Age 65-84 years +4 Age ≥ 85 years +8 Heart rate ≥ 95/’ +1 O2 saturation <95% +2 Temperature (C°) ≥ 38°5 +3 Personal history of VTE +1 Surger(y (under general anesthesia) within 4w4 week
+2
Active malignancy +3 Pregnancy or Postpartum within 4 week +4 Score≤6: proportion of D-dim (NEG) ≥ 20% Score≤8: proportion of D-dim (NEG) ≥ 10% Score≤10: proportion of D-dim (NEG) ≥ 5%
Penaloza , Roy et al. Submitted

Douma et coll. BMJ 2010
Ideal cut-‐off
overall (n=4383)
51-65 y (n=1031)
66-75 y (n=424)
>75 y (n=552)
DD < 500 % FN (IC95%)
0.6 (0.3 -1)
0.2 (0- 0.9)
3.4 (1.1- 8)
1.5 (0.1- 7.0)
NNT 1.9 1.9 3.5 8.1
DD< Age x 10 % FN (IC95%)
0.8 (0.5 -1.2)
0.2 (0- 0.8)
3.4 (1.4-6.9)
3.9 (1.6- 7.9)
NNT 1.8 1.7 2.4 3.6
Penaloza et coll JTH 2012
Borne adaptée : Age x 10 ?

Le scanner est-‐il (toujours) fiable ?
• LA nouvelle REFERENCE diagnosDque – Valeur d’exclusion > scinDgraphie – Valeur de confirmaDon > angiographie
• PerDnence clinique ? – EP sous segmentaire – EP découverte fortuite
• UDlisaDon dans la « vraie » vie ?

4) Le scanner est-‐il (toujours) fiable ?
• Sur la garde. • Radiologue « digesDf » • Protocole non explicite • InterprétaDon succinte

Discordance clinique et CT PC faible et CT + PC élevée et CT –
1) Considérer une 2de lecture du CT: Qualité et fiabilité? Si examen sous-optimal : considérer répétition CT ou Scinti V/P (pts jeunes et sans antcd pulmonaire). Si résultat fiable => 2) 2) Considérer le niveau des artères obstruées 2) Considérer examen des veines MI
(Echo ou phléboCT) Si EP centrale: Traitement anticoagulant
TVP proximale ou pelvienne signe FN au CT → Démarrer anticoagulant
Si EP distale (sous-segmentaires): Echo MI, si négatif: pas de traitement
( Stein et al, 2012 Clin Appl Thromb Hem)
En absence de TVP Exclus patho cliniquement significative → Pas de traitement anticoagulant

En dehors du scanner ?
Risque de démarche inadéquate
• Age > 75 ans • Insuffisance rénale • Insuffisance cardiaque • Pathologie respiratoire • Grossesse et post-‐partum
Intérêt des aides à la décision • RecommandaDons et
protocoles locaux adaptés
• Aide informaDséé à la décision
Risque d’accident thromboembolique et
mort subite inexpliquée x 6
+ 6 %
+ 31 %
Roy et al.. Ann Intern Med 2009
Roy et al.. Ann Intern Med 2006

Stratégie thérapeu3que
Task force Eur Heart J 2008
Thrombolyse USIC Réa
HNF
HBPM Fondaparinux
Hospitalisation

Quoi de neuf en 2013 ?
• Analyse de gravité clinique – biologique -‐ morphologique systémaDsée ?
• Fibrinolyse des EP intermédiaires ? • Place des NACOs ? • Traitement ambulatoire ?

l Données démographiques - Age en années N points - Sexe masculin 10 points
l Comorbidités - Cancer 30 points
- Insuffisance cardiaque 10 points - Pathologie respiratoire chronique 10 points
l Données cliniques - Pression artérielle < 100 / min 30 points - Fréquence cardiaque > 110 / min 20 points
- Fréquence respiratoire > 30 / min 20 points - Saturation en oxygène < 90% 20 points - Température < 36°c 20 points - Confusion – désorientation 60 points
Risque DC 1m Validation ext. à 3 mois
I : Très faible (≤65) 0 % II : Faible (66-85) 3,1 % III : Intermédiaire (86-105) 6,5 % IV : Fort (106-125) 13,1% V : Très fort (>125) 24,4 %
Aujesky et al. AJRCCM 2005 Aujesky et al. Eur Heart J 2006
Risque DC 1m Dérivation Validation Int. Validation Ext. I : Très faible (≤65) 1,1% 1,6% 0% II : Faible (66-85) 3,1% 3,6% 1,8% III : Intermédiaire (86-105) 6,5% 7,5% 3,1% IV : Fort (106-125) 10,4% 11,4% 3,4% V : Très fort (>125) 24,5% 23,9% 8,7%
Pulmonary Embolism Severity Index

Simplified PESI • Age > 80 1 point • Cancer 1 point • Insuffisance cardiaque ou respiratoire chronique 1 point • Pression artérielle < 100 / min 1 point • Fréquence cardiaque > 110 / min 1 point • SaturaDon en oxygène < 90% 1 point
Risque DC 1m Faible (0 point) 1 % (0-2,1)
Elevé (1 point ou plus) 10,9 % (8,5-13,2)
Jiminez et al. Arch Intern Med 2010 Righini et al. JTH 2011

Combinaison PESI et Tropo
• ProspecDve study, 567 PE stable paDents
• AddiDon of normal troponin to PESI did not improve prognosDc accuracy, irrespecDve of the risk class
• Validates the use of PESI
• PESI higher predicDve power than troponin for outpaDents selecDon
n PESI + Tropo I Mortality
149 I-‐II + <0.1 1.3%
232 III-‐V + <0.1 14.2%
43 I-‐II + ≥0.1 0%
143 III-‐V + ≥0.1 15.4%
Moores et al, JTH 2010

sPESI vs. Tropo – analyse VD
• RetrospecDve analysis of prospecDvely collected data • 526 paDents • Comparison simplified PESI vs. Tropo(-‐) and RVD(-‐) (ESC criteria)
-‐ 31% low risk -‐ 39% low risk -‐ 0% death -‐ 3.4% death
-‐ 1.8% complicaDons -‐ 5.8% complicaDons (recurrence, bleeding)
Conclusions -‐ Simplified PESI more accurately idenDfies outpaDents low-‐risk than Tropo.(-‐) /DVD(-‐)
-‐ Without need for any addiDonal laboratory or imaging tesDng
Lankeit et al, Chest 2011

Règle PREP
Sanchez et al. AJRCCM 2010
Risque événement grave à 1 mois I : Faible (<7) 2,5 % II : Intermédiaire (7-17) 11,6 % III : Fort (>17) 43,2 %

Orientation et traitement Stratification du risque
Hypotension Choc
Taille VD normale
Dilatation VD
BNP troponine
Pas de choc sPESI =0
Examen clinique
Pas de choc sPESI > 1
BNP troponine Biomarqueurs
Taille VD
Elevé Inter. fort Faible Intermédiaire faible Stratification
du risque
1- Age > 80 ans 1- Cancer 1- Insf. cardiaque ou respiratoire 1- PAs < 100 mmHg 1- FC > 110 /min 1- SaO2 < 90%

Stratification du risque et prise en charge
Hypotension Choc
Taille VD normale
Dilatation VD
BNP Troponine
Pas de choc sPESI =0
Examen clinique
Pas de choc PESI > 0
BNP Troponine Biomarqueurs
Taille VD
Elévé Int. fort Faible Intermédaire faible Stratification
du risque
Prise en charge initiale
Thrombolyse USIC Réa Thrombolyse ? Ambulatoire ? NACOs ?

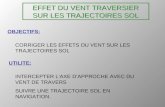
Day 2 Day 7 Day 30
R
DOUBLE BLIND
VKA
Sec
onra
y O
utom
es, S
AE
Prim
ary
Out
com
e, S
econ
dary
Out
com
es
Confirmed acute
symptoma3c PE
Absence of hemodynamic
collapse
Confirmed RV dysfunc3on + myocardial
injury
UFH infusion UFH, LMWH or Fondaparinux
UFH infusion
TNK
Placebo
VKA UFH bolus i.v.
<2 h
UFH, LMWH or Fondaparinux
S Konstantinides for the PEITHO Steering Committee. Am Heart J 2012;163:33-38.e1
PEITHO: Overview of study design
ClinicalTrials.gov # NCT00639743 EudraCT # 2006-005328-18

38
Tenecteplase 100UI/Kg
506
Placebo
499 UFH 2d UFN 2d
All-‐cause mortality or hemodynamic collapse 2.6% 5,6% HR = 0.44
[ 0.23 – 0.88 ]
Major bleedings (non intracranial) 6.3% 1.5% P<0.001
Stroke all causes 2.4% 0.2% P=0.003
Tenecteplase : PEITHO

1.00 0
0.12 0.33
2.00 Odds raDo
0.85
1.00 0
0.23 0.63
2.00 Odds raDo
1.66
PEITHO: Primary end point according to age
Age ≤ 75 years
Age >75 years
ITT population The PEITHO Investigators

DVT and/or PE
D-3 D0
screening 72 h
warfarin INR 2-3 dabigatran placebo
6 months
warfarin placebo dabigatran 150 mg bid
≥J5
initial parenteral treatment UFH - LMWH - fondaparinux
Schulman et al. N Engl J Med 2009; 361.
warfarine è 2 x INR > 2
warfarin placebo
double-blind study R
Dabigatran PRADAXA® : RE-‐COVER

41
Dabigatran 150 mg 1274
Warfarine
1265 Axer 15d
NFH-‐LWMH-‐Fx BID
With 5-‐10d NFH-‐LWMH-‐Fx
OD
Recurence TE events & related deaths 2.35% 2.13% HR = 1.10
[ 0.7 - 1.84 ]
Clin. Relevant bleedings 5.6% 8.8% HR = 0.63
[ 0.5 - 0.8 ]
Major bleedings 1.6% 1.9%
HR = 0.82 [ 0.45 - 1.48 ]
Dabigatran PRADAXA® : RE-‐COVER

PE +/_ DVT
D-2 D0
screening 48 h
VKA* : INR 2-3
3 – 6 – 12 months
Rivaroxaban 20 mg od
3 – 6 – 12 months
Büller et al. N Engl J Med 2012;366:1287-97.
Hep. or fonda ≥ 5 days
VKA* è 2 x INR > 2
Rivaroxaban 15 mg x 2 / d
during 21 days
open study R
D5 D21
Follow-up 1 month
D90 D180 D360
* Warfarin or acenocoumarol
Rivaroxaban XARELTO® : EINSTEIN PE
88 events needed - non inferiority margin: 2

43
Rivaroxaban
2419
Warfarine
2413 15 mg BID 15d 20 mg OD
With 5-‐10d NFH-‐LWMH-‐Fx
Recurence TE events & related deaths
2.1% 1.8% HR = 1.12
Clinically relevant bleedings & major
10.1% 11.4% HR = 0.90 [0.76 – 1.07]
Major bleedings
1.1% 2.2% HR = 0.49 (0.31–0.79)
Rivaroxaban XARELTO® : EINSTEIN PE
Buller H. et al. N Engl J Med 2012; 366:1287-97.

Articles
www.thelancet.com Published online June 23, 2011 DOI:10.1016/S0140-6736(11)60824-6 1
Published OnlineJune 23, 2011DOI:10.1016/S0140-6736(11)60824-6
See Online/CommentDOI:10.1016/S0140-6736(11)60932-X
Bern University Hospital, Bern, Switzerland (Prof D Aujesky MD); LUNAM University and University of Angers, Angers, France (Prof P-M Roy MD); University of Louvain, Brussels, Belgium (F Verschuren MD); University of Geneva, Geneva, Switzerland (M Righini MD, Prof A Perrier MD); Cantonal Hospital of St Gallen, St Gallen, Switzerland (J Osterwalder MD); Cantonal Hospital of Baden, Baden, Switzerland (M Eglo! MD, Prof H-J Beer MD); University Hospital Henri Mondor, Créteil, France (B Renaud MD, A N’gako MD); University of Leuven, Leuven, Belgium (P Verhamme MD); VA Center for Health Equity Research and Promotion, VA Pittsburgh Healthcare System and The Division of General Internal Medicine, School of Medicine (Prof M J Fine MD), Department of Biostatistics (Prof R A Stone PhD, N A Pugh BS), and Department of Emergency Medicine (Prof D M Yealy MD), University of Pittsburgh, PA, USA; University of Argenteuil, Argenteuil, France (C Legall MD); Hôpital Européen Georges Pompidou, Paris, France (O Sanchez MD); and University of Lausanne, Lausanne, Switzerland (Prof J Cornuz MD, O Hugli MD)
Correspondence to:Prof Drahomir Aujesky, Universitätsklinik für Allgemeine Innere Medizin, Inselspital, Bern University Hospital, 3010 Bern, [email protected]
Outpatient versus inpatient treatment for patients with acute pulmonary embolism: an international, open-label, randomised, non-inferiority trialDrahomir Aujesky, Pierre-Marie Roy, Franck Verschuren, Marc Righini, Joseph Osterwalder, Michael Eglo! , Bertrand Renaud, Peter Verhamme, Roslyn A Stone, Catherine Legall, Olivier Sanchez, Nathan A Pugh, Alfred N’gako, Jacques Cornuz, Olivier Hugli, Hans-Jürg Beer, Arnaud Perrier, Michael J Fine, Donald M Yealy
SummaryBackground Although practice guidelines recommend outpatient care for selected, haemodynamically stable patients with pulmonary embolism, most treatment is presently inpatient based. We aimed to assess non-inferiority of outpatient care compared with inpatient care.
Methods We undertook an open-label, randomised non-inferiority trial at 19 emergency departments in Switzerland, France, Belgium, and the USA. We randomly assigned patients with acute, symptomatic pulmonary embolism and a low risk of death (pulmonary embolism severity index risk classes I or II) with a computer-generated randomisation sequence (blocks of 2–4) in a 1:1 ratio to initial outpatient (ie, discharged from hospital ≤24 h after randomisation) or inpatient treatment with subcutaneous enoxaparin (≥5 days) followed by oral anticoagulation (≥90 days). The primary outcome was symptomatic, recurrent venous thromboembolism within 90 days; safety outcomes included major bleeding within 14 or 90 days and mortality within 90 days. We used a non-inferiority margin of 4% for a diff erence between inpatient and outpatient groups. We included all enrolled patients in the primary analysis, excluding those lost to follow-up. This trial is registered with ClinicalTrials.gov, number NCT00425542.
Findings Between February, 2007, and June, 2010, we enrolled 344 eligible patients. In the primary analysis, one (0·6%) of 171 outpatients developed recurrent venous thromboembolism within 90 days compared with none of 168 inpatients (95% upper confi dence limit [UCL] 2·7%; p=0·011). Only one (0·6%) patient in each treatment group died within 90 days (95% UCL 2·1%; p=0·005), and two (1·2%) of 171 outpatients and no inpatients had major bleeding within 14 days (95% UCL 3·6%; p=0·031). By 90 days, three (1·8%) outpatients but no inpatients had developed major bleeding (95% UCL 4·5%; p=0·086). Mean length of stay was 0·5 days (SD 1·0) for outpatients and 3·9 days (SD 3·1) for inpatients.
Interpretation In selected low-risk patients with pulmonary embolism, outpatient care can safely and eff ectively be used in place of inpatient care.
Funding Swiss National Science Foundation, Programme Hospitalier de Recherche Clinique, and the US National Heart, Lung, and Blood Institute. Sanofi -Aventis provided free drug supply in the participating European centres.
IntroductionOutpatient treatment of symptomatic deep vein thrombosis with low-molecular-weight heparin is regarded as usual care.1–3 Despite practice guideline recommendations to extend outpatient care to selected, haemodynamically stable patients with pulmonary embolism, management of symptomatic pulmonary embolism is predominantly inpatient based.4–6
Previous studies of outpatient care after pulmonary embolism were restricted by small sample sizes,7–12 retrospective designs,13–15 and the absence of a randomised control group for comparison with inpatient care.7–18 One randomised trial that compared medical outcomes of patients with pulmonary embolism who were assigned to inpatient versus outpatient care was stopped prematurely because mortality was unacceptably high in both treatment groups.19 We designed the Outpatient Treatment of Pulmonary Embolism (OTPE) trial to
compare the eff ectiveness, safety, and effi ciency of outpatient versus inpatient care for low-risk patients with acute, symptomatic pulmonary embolism as established with a validated clinical prognostic model.20
MethodsStudy design and participantsWe undertook an open-label, randomised, non-inferiority clinical trial at 19 emergency departments in Switzerland, France, Belgium, and the USA. Consecutive adults aged 18 years of age or older with acute, symptomatic, and objectively verifi ed pulmonary embolism who were at low risk of death based on the pulmonary embolism severity index (risk classes I or II; table 1) were eligible to participate.20 The pulmonary embolism severity index is a clinical prognostic model that was derived and validated in more than 16 000 patients with pulmonary embol-ism (C statistic for overall mortality 0·77–0·87).20–23 We
Lancet, July 2011
• Prospective Study: 339 PE randomized - PESI I ou II - max 24h in ED
Outpatients treatment(n=168) vs Inpatients treatment (n=171)
- Mortality 0.6% - Mortality 0.6% - Recurrence 0.6% - Recurrence MTE 0% - Major bleeding 1.8% - Major bleeding 0% - Mean time in hospital 0.5d - Mean time in hospital 3.9d
Conclusions: Outpatient treatment of low-risk patients is as safe as effective than inpatient treatment

Stratification du risque et prise en charge
Hypotension Choc
Taille VD normale
Dilatation VD
BNP
Pas de choc PESI < 85
Examen clinique
Pas de choc PESI > 85
BNP Biomarqueurs
Taille VD
Elévé Int. fort Faible Intermédaire faible Stratification
du risque
Prise en charge initiale
Thrombolyse USIC Réa
HNF ou Fib USC
idem UHtCD
HBPM ou Fx ou NACO hospitalisation

Quoi de neuf aux Urgences ? • DéfiniDon de la suspicion d’EP
dans le doute > PERC • EvaluaDon de la probabilité clinique
Score <> jugement implicite • Dosage des D-‐dimères
PerDnence <> AdaptaDon à l’âge • Angioscanner et ces limites
Analyse <> aides à la décision • StraDficaDon du risque
Clinique PESI <> biologie <> imagerie • Traitement et orientaDon
Fibrinolyse <> NACO en ambulatoire

Quoi de neuf après les SU ?
• Analyse des facteurs favorisant ? • Risque thromboDque / risque hémorragique ? • EducaDon thérapeuDque ? • Durée du traitement ? • Suivi ?

Quoi de neuf après les SU ?