ENTÉROCOLITES GRAVES INFECTIEUSES - Infectiologie
69
ENTÉROCOLITES GRAVES INFECTIEUSES Chez l’adulte et chez l’enfant Julie Toubiana, MCUPH Service de Pédiatrie générale et maladies infectieuses DESC Paris Avril 2015
Transcript of ENTÉROCOLITES GRAVES INFECTIEUSES - Infectiologie

ENTÉROCOLITES GRAVES INFECTIEUSES Chez l’adulte et chez l’enfant Julie Toubiana, MCUPH Service de Pédiatrie générale et maladies infectieuses DESC Paris Avril 2015

Définitions • Inflammation de l’intestin grêle et du colon • D’origine infectieuse
• « grave » = hospitalisation (+/- réa) • EC majoritairement peu sévères : syndrome dysentérique isolé • Complication locale : Colite pseudomembraneuse, mégacolon
toxique, perforation colique • Complication extradigestive
• Perturbations hydroélectrolytiques , IRA fonctionnelle • Choc septique • Syndrome hémolytique et urémique • Atteinte systémique: Tuphos, myocardite..
• Terrain
• Formes communautaires, retour de voyage, nosocomial et ID • Particularités pédiatriques • Formes du nouveau né • Flore pédiatrique différente?

Aspects cliniques • Diarrhée : au moins 3 selles/jour de consistance anormale • Douleurs abdominales + • Syndrome cholérique
• Diarrhée sécrétoire : Selles liquides profuses, douleurs abdominales, pas de fièvre (ou modérée)
• Activation AMPc

Active l’adényl cyclase intra-entérocytaire • Augmente l’AMPc intracellulaire : sécrétion immédiate d’électrolytes (Na+ et Cl-) et d’eau vers la lumière intestinale • Diarrhée aqueuse afécale du choléra Mais l’absorption du Na couplée au glucose n’est pas bloquée : Donc REHYDRATATION ORALE POSSIBLE (SRO)
Diapos OMS
Exemple de diarrhée sécrétoire : La toxine cholérique

Aspects cliniques • Diarrhée : au moins 3 selles/jour de consistance anormale • Douleurs abdominales • Syndrome cholérique
• Diarrhée sécrétoire : Selles liquides profuses, douleurs abdominales, pas de fièvre (ou modérée)
• Activation AMPc
• Syndrome dysentérique • Diarrhée invasive ‘afécale’ composée de sang, glaires ou pus • Épreintes (coliques violentes avant évacuation), ténesme (tension
douloureuse dans la région de l’anus) • Fièvre en général élevée sauf en cas d’amoebose • Mécanisme entéro-invasif

Envahissement, réplication, destruction, inflammation
Flore commensale
Sansonetti, 2011
Flore invasive Complication: sepsis, perforation digestive

Formes sévères locales, risque de perforation • Mégacolon toxique
• Dilatation > 7 cm colon transverse • SIRS
• Entérocolite neutropénique = typhlite • Colite aigue ulcéreuse coecum, iléon terminal • Septicémie par translocation associée++

Anamnèse importante • Prise récente d’antibiotiques • Cas dans l’entourage • Voyage étranger • Conduites à risque (eau non potable…) • Durée présumée d’incubation • Animaux • Comorbidités (MICI++) • Immunodépression

Agents infectieux bactériens principaux Agent infectieux Incidence/an (USA) Forme clinique Anamnèse
C. difficile >250 000/an hospitalisés
D. invasive Mégacolon toxique
ATB et FDR
Shigella 450 000 D. invasive Contagiosité++
Salmonelle non typhi 1,4 millions D. sécrétoire Sepsis chez nourrisson
Transmission alimentaire
Campylobacter jejuni 1,4-2,4 millions Souvent D. invasive
Alimentaire, voyage
EHEC 100 000 D. Sécrétoire puis sanglante
Alimentaire Epidémies
Cholera 50 D. sécrétoire Régions endémiques
E. Coli enterotoxique D. sécrétoire Alimentaire, voyage
Typhoide paratyphoide 800 Signes systémiques+ dleur/diarrhée/ileus
Voyage, eau contaminée
Yersinia enterocolitica 96 000 D. sécrétoire +/- D. invasive si pseudoappendiculaire
Réservoir animaux d’élevage Rare ds pays dév
S. Aureus C. Perfringens B. cereus
185000 250 000 27 000
D. sécrétoire incubation courte
Alimentaire Epidémie
D’après Dupont LD NEJM 2009

Contexte plus particulier • Entérocolites non-bactériennes
• Gastroentérites virales (enfant+++, Rotavirus+++) • Tuberculose digestive • Enterocolites de l’immunodéprimé
• Clostridium difficile • Parasites opportunistes : Cryptosporidium, Microsporidium, Giardia,
Isospora • CMV, EBV • Candida spp., Mucomycose, cryptocoque, Pneumocytis jiroveci • Mycobacteriose atypique (complexe avium+++)
• Colites de réanimation • C. difficile • K. oxytoca (?) Responsabilité discutée • CMV

Dupont LD NEJM 2014

Diagnostic • Microbiologique:
• Coproculture++ sur selles fraiches • Toxines selon contexte (PCR) • Hémocultures dans formes septiques • EPS: Amoebose ou chez l’ID • PCR ou IF : virus++
• Endoscopie et biopsies coliques : oriente étiologie et DD • Coloscopie complète sur colon préparé • Inflammation muqueuse, pseudomembranes, ulcérations • Localisation • Biospises étagées
Makharia GK et al. 2010, Gouin P, 2008
C. Difficile (colon)
Tuberculose (ileo-cecal)

Anatomopathologie Pseudomembranes Granulome Inclusions
C. difficile Yersinia CMV/HSV
EHEC Mycobacterie Champignons
Shigella (rare) Champignons Amibe
Yersinia: granulome EHEC Tuberculose : granulome
Pseumomembrane ICD

Attention, diagnostic différentiel MICI
« Crohn » « RCH » « Colite ischémique »
Salmonelle Salmonelle EHEC
Shigelle Shigelle CMV
Yersinia Syphilis Mucorales
Campylobacter E. histolytica
Aeromonas C. difficile
E. histolytica C. perfringens
CMV
Mycobactérie

Diagnostic • Imagerie
• Evaluation de la gravité • ASP: niveaux, pneumopéritoine, pneumatose • Echographie: ascite, épaississement des membranes de la colite
pseudomembraneuse • Scanner avec PDC: GRAVITE
• Extension des lésions • Mégacolon toxique • Pneumatose pariétale • Elimination de DD
cryptococcose Colite pseudomembraneuse
Gouin P, 2008

Dupont LD NEJM 2009
Formes systémiques et FDR: - Nourrisson - Déficit immunitaire

• Hawa 6 ans pas d’ATCD, Frère: diarrhée glairo-sanglante
il y a 3 jours • HDM:
• Diarrhée non glairosanglante, fièvre, Somnolente • Vient aux Urgences:
• Fatiguée++ • Pas de signes de déshydratation clinique ou biologique,
Retour à domicile • Convulsion le soir tonicoclonique, avec syndrome pyramidal
postcritique • CRP 150mg/l, PL négative, pas d’insuffisance rénale, iono
normale, thrombopénie • Coproculture=> A quoi vous attendez vous? Traitement?
Cas clinique n°1

• Sécrétion de la shiga toxine responsable de la diarrhée sécrétoire
• Atteinte neurologique chez l’enfant • Traitement per os première intention
• AZITHROMYCINE 5 jours : 20 mg / kg /j
• Alternative : ciprofloxacine 5 jours • Forme sévère : ceftriaxone ou ciprofloxacine
injectable 5 jours
Shigellose Recommandations ESPID / ANSM

Cas clinique , Loane 3 ans • Aucun antécédent personnel ou familial • Diarrhées glairo-sanglantes pendant 3 jours traitée par
azithromycine • Puis apparition d’hallucinations visuelles, propos
incohérents, euphorie inhabituelle, puis crise convulsvie • Biologie
• Hb 16,8 g/dl puis 10,8 g/dl, Plaquettes 26 000/mm3, PNN 32 000/mm3
• Créatininémie = 200 µmol/l, Urée = 27 mM
• CRP 285

IRM séquence FLAIR

Pendant ce temps, son frère de 7 mois • Aucun antécédent personnel • Diarrhées glairo-sanglantes apparues le 16/11 • Insuffisance rénale aiguë et anémie hémolytique
• DIAGNOSTIC?

Syndrome hémolytique et urémique • Post diarrhéique • E. coli O-121 sécréteur de shiga-toxine
• Apparition d’un iléus, contracture abdominale et fièvre • Exploration chirurgicale • Péritonite sur perforation sigmoïdienne haute • Résection colon gauche 19 cm, double colostomie gauche • Anapath : nécrose ischémique, vascularite
Image from Ullrich et al. Plos one 2013

Infections à E. coli producteurs de Shigatoxines (EHEC, STEC)
• France: 80 à 100 cas/ an de SHU STEC+ < 15 ans • +++< 3 ans
• Toxi-infection alimentaire le plus souvent • Cas sporadiques ou petites épidémies surtout collectivités • Formes cliniques variées :
• Diarrhée parfois sanglante • Colite hémorragique • Syndrome hémolytique et urémique
• principale cause IRA chez l’enfant < 3 ans • Complications neurologiques et séquelles rénales • Létalité : 1 à 6 %
• Préoccupation de santé publique dans les pays industrialisés

Mode de transmission
• Ingestion d’aliments contaminés 60% • Produits animaux (bovins) • Végétaux crus • Jus de fruits non pasteurisés
• Transmission interhumaine 20% • Crèche, hôpitaux, famille
• Eau contaminée 12% • Contact direct avec animaux d’élevage

Ecosse 1996, 400 cas,18 décès
France : 2005, 2011
Japon 1996, 9000 cas, 100 SHU, 9 décès (Enfants)
Allemagne 2011 4320 infections 852 SHU (90% Adultes) 82 décès
Etats-Unis 1982-2002 350 épidémies 8598 cas dont 17% hospitalisations, 4% SHU, 0.5% décès

En France : nombre de SHU

E coli producteur de shiga-toxine
The Lancet 2005

Physiopathologie • Adhésion
• Vérotoxines ou shigatoxine like • Exotoxines protéiques (Intimin) • Récepteurs glycolipidiques Gb3 des cellules intestinales et
endothelium vasculaire • Mort cellulaire par arrêt de la synthèse protéique
• Cellules endothéliales du rein humain, glomérules des nourrissons < 2 ans, masqué chez l’adulte
• Endothélium pancréas et SNC • Induction de l’inflammation locale • Diffusion des toxines vers le rein et SNC • Lésions endothéliales, microthrombi MAT

Diagnostic STEC • Recueil des selles • OU prélèvement rectal : ne pas attendre++ • Portage bref jusqu’à 4 à 7 jours après les symptômes
• Culture • E. coli O157:H7
• Caractéristiques biochimiques (Sorbitol-, rhamnose -, résistance intermédiaire au Cefixime et tellurite
• Culture dans une boite spéciale CT-S-MacConkey agar, puis confirmation par test agglutination
• Recherche de toxine stx1 et stx 2 par immunoassay ou PCR
Tarr et al. CID, 1995

Epidémie atypique en 2011 E. coli O104:H4 • 4320 infections • 852 SHU
• 90% chez des Adultes
• 82 décès
• 2/3 de femmes : régime alimentaire • Incubation moyenne : 8 jours vs 3-4 jours pour les EHEC • Virulence inhabituelle : ¼ des formes évoluant vers des
formes graves (vs 1/10) Ullrich Plos one 2013

Nouveau pathovar : E.coli entero-aggregant enterohemorragique (EAHEC)
• Plasmide de virulence aat, aac, aag • MLST séquence type: ST678 • BLSE CTX-M-15 • Shiga toxine 2 (STX2) • Intimin nég (eae)
• autre mécanisme d’adhésion

Place des traitements dans le SHU de l’enfant?
• Antibiothérapie NON • Correction des troubles HE, et HTA OUI • Dialyse péritonéale OUI • Hémodiafiltration (formes sévères) OUI • Perfusion / échange plasma: Pas d’intérêt dans SHU typique NON
• Corticoïdes: Effets minimes sur la créatinine NON • Anti-C5 : basé sur un taux élevé de C5 chez certains enfants au début infection …
Loirat et al. 2012

Eculizumab.. Pas d’étude randomisée!
correspondence
n engl j med 364;26 nejm.org june 30, 2011 2561
The author replies: Miller and colleagues are correct that pharmacists can be a valuable re-source for teaching physicians about medica-tions and appropriate prescribing. Pharmacists currently serve important educational roles in many medical centers and integrated health care systems and are the most widely used outreach educators in academic detailing programs. How-ever, outside these settings, pharmacists’ knowl-edge of drugs remains badly underused, because the rest of the health care system is not yet con-figured in a way that can take full advantage of this potentially important resource. Most phar-macists in routine community practice rarely get
to use even a small fraction of their considerable pharmacologic knowledge, and they do not have enough time to provide the interactions with pa-tients that could be so helpful. We can look to the day when nonphysician health professionals — particularly including pharmacists — can as-sume the larger role they deserve in educating practitioners and patients about optimal medica-tion use.
Jerry Avorn, M.D. Harvard Medical School Boston, MA
Since publication of his article, the author reports no further potential conflict of interest.
Eculizumab in Severe Shiga-Toxin–Associated HUS
To the Editor: The hemolytic–uremic syndrome (HUS), a thrombotic microangiopathy, most com-monly occurs secondary to infection with Shiga-toxin–producing Escherichia coli (STEC-HUS), al-though rare, atypical forms are associated with abnormalities in complement-regulating proteins. The inhibition of terminal complement complex formation by the monoclonal C5 antibody eculi-zumab has recently been reported as a treatment for atypical HUS.1
We report on three 3-year-old patients with severe STEC-HUS that required hemodialysis. In Patient 1, plasma exchanges were performed because of low C3 and elevated C3d serum con-centrations, which suggested complement acti-vation. Plasma exchange was also performed in Patient 2 because of severe central nervous sys-tem involvement, a rare complication that often leads to death or permanent neurologic dam-age.2 Progressive involvement of the central ner-vous system developed in both patients despite 5 consecutive days of plasma exchange.
Given the devastating prognosis, we adminis-tered eculizumab to these two patients, as well as to a third patient with a similar disease course, at 7-day intervals, twice in Patients 1 and 3 and four times in Patient 2. The neurologic status in all three patients improved dramatically within 24 hours after the first eculizumab infusion. Clinical improvement was associated with rapid normalization of markers of disease activity: plate-
let counts normalized, and lactate dehydrogenase levels decreased within 5 days in all patients (Fig. 1, and the Supplementary Appendix, available with the full text of this letter at NEJM.org).
Dialysis was discontinued after 3 days in Pa-tient 1, after 16 days in Patient 2, and after 13 days in Patient 3, and the patients were discharged with apparently normal neurologic status 9, 35, and 20 days, respectively, after the administration of the first dose of eculizumab. Renal function fully recovered, with mild residual proteinuria and hypertension in Patients 1 and 3. All patients have remained in full remission for the past 6 months. Screening for mutations in the genes encoding complement regulatory proteins (CFH, CFI, MCP, C3, CFB, and THBD) and testing for anti-CFH anti-bodies were negative in all patients.
In the cases reported here, spontaneous recov-ery seemed unlikely, given the rapidly progressive course of the disease. The rapid clinical response to eculizumab in all three children supports the concept that Shiga toxin may activate comple-ment directly,3 providing a rationale for thera-peutic complement blockade in STEC-HUS with severe complications. Complement hyperactiva-tion was recently demonstrated in STEC-HUS,4 and a mutation in the complement-regulating gene MCP was reported in a fatal case of STEC-HUS.5 The dramatic resolution of symptoms after eculizumab administration in the cases reported here suggests that STEC-HUS is an area deserv-
The New England Journal of Medicine Downloaded from nejm.org at ASSISTANCE PUBLIQUE HOPITAUX PARIS on December 6, 2012. For personal use only. No other uses without permission.
Copyright © 2011 Massachusetts Medical Society. All rights reserved.
The n
ew
en
gl
an
d jo
ur
na
l of m
ed
icin
e
n en
gl j m
ed 364;26
nejm
.org
ju
ne 30, 2011
2562
Plas
ma
Cre
atin
ine
(mg/
dl)
6
2
4
0
3
5
1
100
20
806040
010 108 866 4 42 2 20181614120 22
Plat
elet
Cou
nt (×
10−3
/µl)
Leuk
ocyt
e C
ount
(×10
−3/µ
l)La
ctat
e D
ehyd
roge
nase
(U/l
iter)
500
300
200
100
400
0
350
250
150
450
50
3500
1500
1000
500
3000
2500
2000
010 108 866 4 42 2 20181614120 22
Day of TreatmentDay beforeTreatment
A Patient 1
Plas
ma
Cre
atin
ine
(mg/
dl)
5
21
43
0
5
21
43
0
100
20
806040
05 0 40355 10 3015 2520 45
5 0 40355 10 3015 2520 45
Plat
elet
Cou
nt (×
10−3
/µl)
Leuk
ocyt
e C
ount
(×10
−3/µ
l)La
ctat
e D
ehyd
roge
nase
(U/l
iter)
5 0 40355 10 3015 2520 45
5 0 40355 10 3015 2520 45
0
500
300
200
100
400
0
350
250
150
450
50
2500
1500
1000
500
2000
0
Day of TreatmentDay beforeTreatment
B Patient 2
Plas
ma
Cre
atin
ine
(mg/
dl)
100
20
806040
0
Plat
elet
Cou
nt (×
10−3
/µl)
Leuk
ocyt
e C
ount
(×10
−3/µ
l)La
ctat
e D
ehyd
roge
nase
(U/l
iter)
500
300
200
100
400
0
350
250
150
450
50
3000
1500
1000
500
2500
2000
0
Day of TreatmentDay beforeTreatment
C Patient 3
Eculizumabinfusions
Plasmaexchange
Eculizumabinfusions
Plasmaexchange
Eculizumabinfusions
Hemodialysis Hemodialysis Hemodialysis
4 Day
s befo
re
Trea
tmen
t
2 Day
s befo
re
Trea
tmen
t
1 Day
befor
e
Trea
tmen
t
Day 8
of
Trea
tmen
t
Lactatedehydrogenase
Plasma creatininePlasma creatinine
Plasma creatinine
Platelet
Leukocyte LeukocyteLeukocyte
Platelet
Platelet
Lactate dehydrogenaseLactate dehydrogenase
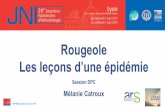
Figure 1. Response to Eculizumab Therapy in Three Children with STEC-HUS and Progressive Central Nervous System Involvement.
Shown are data indicating rapid clinical improvement after the administration of monoclonal C5 antibody eculizumab in three children with the hemolytic–uremic syndrome associ-ated with infection with Shiga-toxin–producing Escherichia coli (STEC-HUS), resulting in central nervous system involvement (as shown in Patient 1 in Panel A). In all three children, there was a rapid normalization in plasma creatinine levels and leukocyte counts, as well as in platelet counts and lactate dehydrogenase levels.
The New
England Journal of Medicine
Dow
nloaded from nejm
.org at ASSISTA
NCE PU
BLIQU
E HO
PITAU
X PA
RIS on Decem
ber 6, 2012. For personal use only. No other uses w
ithout permission.
Copyright © 2011 M
assachusetts Medical Society. A
ll rights reserved.
The n
ew
en
gl
an
d jo
ur
na
l of m
ed
icin
e
n en
gl j m
ed 364;26
nejm
.org
ju
ne 30, 2011
2562
Plas
ma
Cre
atin
ine
(mg/
dl)
6
2
4
0
3
5
1
100
20
806040
010 108 866 4 42 2 20181614120 22
Plat
elet
Cou
nt (×
10−3
/µl)
Leuk
ocyt
e C
ount
(×10
−3/µ
l)La
ctat
e D
ehyd
roge
nase
(U/l
iter)
500
300
200
100
400
0
350
250
150
450
50
3500
1500
1000
500
3000
2500
2000
010 108 866 4 42 2 20181614120 22
Day of TreatmentDay beforeTreatment
A Patient 1
Plas
ma
Cre
atin
ine
(mg/
dl)
5
21
43
0
5
21
43
0
100
20
806040
05 0 40355 10 3015 2520 45
5 0 40355 10 3015 2520 45
Plat
elet
Cou
nt (×
10−3
/µl)
Leuk
ocyt
e C
ount
(×10
−3/µ
l)La
ctat
e D
ehyd
roge
nase
(U/l
iter)
5 0 40355 10 3015 2520 45
5 0 40355 10 3015 2520 45
0
500
300
200
100
400
0
350
250
150
450
50
2500
1500
1000
500
2000
0
Day of TreatmentDay beforeTreatment
B Patient 2
Plas
ma
Cre
atin
ine
(mg/
dl)
100
20
806040
0
Plat
elet
Cou
nt (×
10−3
/µl)
Leuk
ocyt
e C
ount
(×10
−3/µ
l)La
ctat
e D
ehyd
roge
nase
(U/l
iter)
500
300
200
100
400
0
350
250
150
450
50
3000
1500
1000
500
2500
2000
0
Day of TreatmentDay beforeTreatment
C Patient 3
Eculizumabinfusions
Plasmaexchange
Eculizumabinfusions
Plasmaexchange
Eculizumabinfusions
Hemodialysis Hemodialysis Hemodialysis
4 Day
s befo
re
Trea
tmen
t
2 Day
s befo
re
Trea
tmen
t
1 Day
befor
e
Trea
tmen
t
Day 8
of
Trea
tmen
t
Lactatedehydrogenase
Plasma creatininePlasma creatinine
Plasma creatinine
Platelet
Leukocyte LeukocyteLeukocyte
Platelet
Platelet
Lactate dehydrogenaseLactate dehydrogenase
Figure 1. Response to Eculizumab Therapy in Three Children with STEC-HUS and Progressive Central Nervous System Involvement.
Shown are data indicating rapid clinical improvement after the administration of monoclonal C5 antibody eculizumab in three children with the hemolytic–uremic syndrome associ-ated with infection with Shiga-toxin–producing Escherichia coli (STEC-HUS), resulting in central nervous system involvement (as shown in Patient 1 in Panel A). In all three children, there was a rapid normalization in plasma creatinine levels and leukocyte counts, as well as in platelet counts and lactate dehydrogenase levels.
The New
England Journal of Medicine
Dow
nloaded from nejm
.org at ASSISTA
NCE PU
BLIQU
E HO
PITAU
X PA
RIS on Decem
ber 6, 2012. For personal use only. No other uses w
ithout permission.
Copyright © 2011 M
assachusetts Medical Society. A
ll rights reserved.
The n
ew
en
gl
an
d jo
ur
na
l of m
ed
icin
e
n en
gl j m
ed 364;26
nejm
.org
ju
ne 30, 2011
2562
Plas
ma
Cre
atin
ine
(mg/
dl)
6
2
4
0
3
5
1
100
20
806040
010 108 866 4 42 2 20181614120 22
Plat
elet
Cou
nt (×
10−3
/µl)
Leuk
ocyt
e C
ount
(×10
−3/µ
l)La
ctat
e D
ehyd
roge
nase
(U/l
iter)
500
300
200
100
400
0
350
250
150
450
50
3500
1500
1000
500
3000
2500
2000
010 108 866 4 42 2 20181614120 22
Day of TreatmentDay beforeTreatment
A Patient 1
Plas
ma
Cre
atin
ine
(mg/
dl)
5
21
43
0
5
21
43
0
100
20
806040
05 0 40355 10 3015 2520 45
5 0 40355 10 3015 2520 45
Plat
elet
Cou
nt (×
10−3
/µl)
Leuk
ocyt
e C
ount
(×10
−3/µ
l)La
ctat
e D
ehyd
roge
nase
(U/l
iter)
5 0 40355 10 3015 2520 45
5 0 40355 10 3015 2520 45
0
500
300
200
100
400
0
350
250
150
450
50
2500
1500
1000
500
2000
0
Day of TreatmentDay beforeTreatment
B Patient 2
Plas
ma
Cre
atin
ine
(mg/
dl)
100
20
806040
0
Plat
elet
Cou
nt (×
10−3
/µl)
Leuk
ocyt
e C
ount
(×10
−3/µ
l)La
ctat
e D
ehyd
roge
nase
(U/l
iter)
500
300
200
100
400
0
350
250
150
450
50
3000
1500
1000
500
2500
2000
0
Day of TreatmentDay beforeTreatment
C Patient 3
Eculizumabinfusions
Plasmaexchange
Eculizumabinfusions
Plasmaexchange
Eculizumabinfusions
Hemodialysis Hemodialysis Hemodialysis
4 Day
s befo
re
Trea
tmen
t
2 Day
s befo
re
Trea
tmen
t
1 Day
befor
e
Trea
tmen
t
Day 8
of
Trea
tmen
t
Lactatedehydrogenase
Plasma creatininePlasma creatinine
Plasma creatinine
Platelet
Leukocyte LeukocyteLeukocyte
Platelet
Platelet
Lactate dehydrogenaseLactate dehydrogenase
Figure 1. Response to Eculizumab Therapy in Three Children with STEC-HUS and Progressive Central Nervous System Involvement.
Shown are data indicating rapid clinical improvement after the administration of monoclonal C5 antibody eculizumab in three children with the hemolytic–uremic syndrome associ-ated with infection with Shiga-toxin–producing Escherichia coli (STEC-HUS), resulting in central nervous system involvement (as shown in Patient 1 in Panel A). In all three children, there was a rapid normalization in plasma creatinine levels and leukocyte counts, as well as in platelet counts and lactate dehydrogenase levels.
The New
England Journal of Medicine
Dow
nloaded from nejm
.org at ASSISTA
NCE PU
BLIQU
E HO
PITAU
X PA
RIS on Decem
ber 6, 2012. For personal use only. No other uses w
ithout permission.
Copyright © 2011 M
assachusetts Medical Society. A
ll rights reserved.

Place de l’antibiothérapie? Encore expérimental
Souches O104:H4 Souche O157:H7
ATB bactéricide: effet délétère car relargage des toxines+++ Intérêt des agents bactériostatiques, inhibiteurs de synthèse protéique

Manganèse
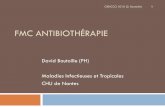
Manganese Blocks IntracellularTrafficking of Shiga Toxin andProtects Against Shiga ToxicosisSomshuvra Mukhopadhyay and Adam D. Linstedt*
Infections with Shiga toxin (STx)–producing bacteria cause more than a million deaths eachyear and have no definitive treatment. To exert its cytotoxic effect, STx invades cells throughretrograde membrane trafficking, escaping the lysosomal degradative pathway. We foundthat the widely available metal manganese (Mn2+) blocked endosome-to-Golgi trafficking ofSTx and caused its degradation in lysosomes. Mn2+ targeted the cycling Golgi protein GPP130,which STx bound in control cells during sorting into Golgi-directed endosomal tubules thatbypass lysosomes. In tissue culture cells, treatment with Mn2+ yielded a protection factor of 3800against STx-induced cell death. Furthermore, mice injected with nontoxic doses of Mn2+ werecompletely resistant to a lethal STx challenge. Thus, Mn2+ may represent a low-cost therapeuticagent for the treatment of STx infections.
Shiga toxin (STx)–producing bacteria ofthe Shigella genus and enterohemorrhagicEscherichia coli (EHEC) species infect
more than 150 million individuals each yearand cause more than a million deaths (1). Thereis no definitive medical treatment. Indeed, treat-ment with antibiotics is contraindicated becauseit increases the risk of STx release and life-threatening disease (1–3). STx consists of a cat-alytically toxic A subunit bound to a B subunit
that mediates its membrane trafficking fromthe cell surface through endosomes, the Golgiapparatus, and the endoplasmic reticulum (ER),where the toxin translocates to the cytosol and in-activates ribosomes (4). Direct trafficking of STxfrom early endosomes to the Golgi, bypassing lateendosomes and lysosomes, is a crucial step thatallows STx to avoid degradation. Small-moleculeinhibitors targeting this step hold therapeutic prom-ise, but the STx interactions responsible for itsendosomal sorting remain unclear.
Exposure of cells to 50 to 500 mM manga-nese (Mn2+) induces degradation of GPP130 (5, 6),a membrane protein that cycles between the Golgiand endosomes (7, 8). Because GPP130 plays
a role, albeit undefined, in endosome-to-Golgitrafficking of STx (9), we asked whether Mn2+
acts as a small-molecule inhibitor of STx. Toinvestigate the effect of Mn2+ on STx trafficking,we used a fluorescently tagged version of the Bsubunit of STx (STxB) that exhibits transportkinetics identical to the holotoxin (10, 11). Where-as STxB efficiently trafficked from the cell sur-face to the Golgi in control cells, cells exposed to500 mM Mn2+ lacked GPP130, and STxB accu-mulated in peripheral punctate structures resem-bling endosomes (Fig. 1, A and B). We confirmedthat STxB did not reach the ER (fig. S1) by usinga STxB version with a KDEL tag, which increasesits retention in the ER (12).
The Mn-induced block in STxB traffickingwas specific. There was no difference betweenMn2+-treated and control cells in cholera toxinB subunit (CTxB) trafficking (Fig. 1C and fig.S2), which follows the same route as STx to theGolgi (13). Moreover, Mn2+ did not affect epi-dermal growth factor (EGF) internalization anddegradation (fig. S3) or ER-to-cell-surface traf-ficking of vesicular stomatitis virus G protein(fig. S4). Further, Mn2+ did not alter the localiza-tion or trafficking of GP73 and TGN46, endog-enous proteins that constitutively cycle betweenthe Golgi and endosomes, or Lamp2, which traf-fics from the Golgi to lysosomes (fig. S5). Fi-nally, 500 mM Mn2+ did not affect cell viability(Fig. 1D).
The accumulation of STxB in intracellularpunctae implies that Mn2+ blocks STxB afterinternalization. Indeed, STxB moved to Rab5-positive early endosomes and, instead of exit-ing to the Golgi, trafficked to Rab7-positive
Department of Biological Sciences, Carnegie Mellon Univer-sity, Pittsburgh, PA 15213, USA.
*To whom correspondence should be addressed. E-mail:[email protected]
Fig. 1. Manganese specifically blocks STxB trafficking. (A) STxB transportfor the indicated times in HeLa cells untreated or pretreated with 500 mMMn2+ for 4 hours. Scale bar, 10 mm. (B and C) Percentage of cellular STxBor CTxB in the Golgi at the indicated times postinternalization (mean T SE;20 cells per point). See fig. S2 for CTxB images. (D) Normalized cell viabilityby methylthiazolylphenyl-tetrazolium bromide (MTT) assay. Mn2+ was 500 mMfor 12 hours (mean T SE; n = 3 experiments).
20 JANUARY 2012 VOL 335 SCIENCE www.sciencemag.org332
REPORTS
on
Dec
embe
r 6, 2
012
ww
w.s
cien
cem
ag.o
rgD
ownl
oade
d fro
m DOI: 10.1126/science.1215930
, 332 (2012);335 ScienceSomshuvra Mukhopadhyay and Adam D. LinstedtProtects Against Shiga ToxicosisManganese Blocks Intracellular Trafficking of Shiga Toxin and
This copy is for your personal, non-commercial use only.
clicking here.colleagues, clients, or customers by , you can order high-quality copies for yourIf you wish to distribute this article to others
here.following the guidelines
can be obtained byPermission to republish or repurpose articles or portions of articles
): December 6, 2012 www.sciencemag.org (this information is current as of
The following resources related to this article are available online at
http://www.sciencemag.org/content/335/6066/332.full.htmlversion of this article at:
including high-resolution figures, can be found in the onlineUpdated information and services,
http://www.sciencemag.org/content/suppl/2012/01/19/335.6066.332.DC2.html http://www.sciencemag.org/content/suppl/2012/01/19/335.6066.332.DC1.html
can be found at: Supporting Online Material
http://www.sciencemag.org/content/335/6066/332.full.html#relatedfound at:
can berelated to this article A list of selected additional articles on the Science Web sites
http://www.sciencemag.org/content/335/6066/332.full.html#ref-list-1, 14 of which can be accessed free:cites 27 articlesThis article
http://www.sciencemag.org/content/335/6066/332.full.html#related-urls2 articles hosted by HighWire Press; see:cited by This article has been
http://www.sciencemag.org/cgi/collection/cell_biolCell Biology
subject collections:This article appears in the following
registered trademark of AAAS. is aScience2012 by the American Association for the Advancement of Science; all rights reserved. The title
CopyrightAmerican Association for the Advancement of Science, 1200 New York Avenue NW, Washington, DC 20005. (print ISSN 0036-8075; online ISSN 1095-9203) is published weekly, except the last week in December, by theScience
on
Dece
mbe
r 6, 2
012
www.
scie
ncem
ag.o
rgDo
wnlo
aded
from

Evolution de Loane
• Digestive : Colite inflammatoire • Apparition de rectorragies, fièvre, vomissements • ATBthérapie large Méropénème Vancomycine amikacine (AAC 2012) • Clostridium nég (co-infections) • Exploration chirurgicale
• Péritonite sur perforation sigmoïdienne: Résection colon double colostomie gauche - Anapath : vascularite
• Prélèvement : Persistance de la sécrétion de toxine • Manganèse • Azithromycine
• Neurologique : lentement favorable • Rénale: récupération lente, sevrage de la dialyse

Cas N°2 • Femme de 75 ans, insuffisance respiratoire chronique sur
BPCO, angor, HTA • Pas d’allergie connue • Décompensation respiratoire aigue sur infections
respiratoire • Mise sou amox/Ac Clav • A J4 de l’ATB: diarrhée 8-10 selles par jour
• Diagnostic?

FDR d’ICD • Antibiothérapie
• Céphalosporines, et beta-lactamines large spectre • Amx/Ac. Clav • Clindamycine • FQ
• ATCD d’ICD • Age : incidence multipliée par 10 si plus de 65 ans • Hospitalisation prolongée • Prise d’anti-ulcéreux • Immunodépression
Derling SN, Clin Infect Dis 2004

Evolution récente des ICD

Evolution récente des ICD • Augmentation de la sévérité des ICD
• Complications (CS, perforation, colectomie): 6% (1993) vs 18.2% (2003)
• Mortalité à 30 j : 5% (1994) vs 13% (2003) • Moins bonne réponse au métronidazole
• Plus d’échecs thérapeutiques: 9.6% en 2002 vs 25.7% en 2004 • Plus de rechutes
• Fluoroquinolone: nouveau facteur de risque d’infection • Dissémination du clone 027 (3.1% des souches en
France) • Des USA et Canada • Clone hypervirulent, hyperproducteur de toxine, infections sévères y
compris chez le jeune • FQ R
Pépin J et al, CMAJ 2004, Aslam et al. Lancet Inf. Dis , 2005

Particularités de l’enfant • Fréquence élevée de porteurs asymptomatiques
• Surtout < 3ans • Passe de 2,5% chez l’adulte à 35% chez les nourrissons <6
mois. A
• FDR • Exposition aux antibiotiques • Durée d’hospitalisation prolongée • Immunodéficience (traitement immunosuppresseur,
chimiothérapie, hypo- ou agammaglobulinémie) • Maladies chroniques du tube digestif (MICI, maladie de
Hirschsprung).
Loo VG, NEJM 2011

Diagnostic • Diarrhée Bristol 5-7 • Au moins 3 selles par jour • OU ileus • OU mégacolon toxique
• + Confirmation • Microbiologique • OU endosocopique • OU histologique

Diagnostic • Recherche d’un antigènes : GDH (Glutamate
déshydrogénase) • par immunochromatographie • VPN +++ >90%
• Si positive: • Recherche de la toxine B de CD par PCR sur la selle • PCR: possibilité de rechercher la souche hyper virulente
• Pas d’intérêt en France de réaliser un antibiogramme: sont toutes sensibles au metronidazole et vancomycine

Critères de sévérité

Marqueurs de sévérité : Procalcitonine?
Rao K, PlOS one Mars 2013
PCT <0,2Valeur prédictive négative de 90%

Gravité chez l’enfant • Infection « bénigne » : diarrhée aqueuse « simple » (< 4 selles
molles /jour, sans toxicité systémique
• Infection modérée : diarrhée ≥ 4 selles molles /jour, sans toxicité systémique
• Maladie grave : diarrhée avec présence de signes de toxicité systémique (fièvre > 38.5°C, frissons..)
• Maladie grave compliquée : colite sévère avec signes de toxicité systémique : • admission en unité de soins intensifs pour la prise en charge de la
colite à CD • hypotension • état de choc

Adulte
Situations Recommandation Grade Colite non grave Métronidazole per os 500 mg x 3 /jour
pendant 10 jours Vancomycine per os 125 mg x 4 /jour pendant 10 jours
AI BI
Colite grave Vancomycine per os AI
Colite grave compliquée avec distension abdominale importante
Vancomycine per os + metronidazole IV +/- discussion chirurgicale
AI
Debast SB, Clin Microbiol Infect 2014 (ESCMID)

Définition de la sévérité: > ou =2 points -Age>60 ans : 1 pt -T>38°3 : 1 pt -Alb. <2.5 mg/dl 1 pt -Leuco > 15000/mm3 1p -CPM : 2 pts -ICU 2 pts
P=0.02

Récidive • Réapparition de l’infection à Clostridium difficile dans les 8
semaines suivant un précédent épisode résolutif sous traitement.
• Taux de récidive: ` • 19-20% après 1er épisode, 45% > 2 épisodes
• Modification du microbiome • Réponse immunitaire • Spore
1ere récidive Alternative
Vancomycine per os ou Métronidazole per os Fidaxomicine per os 200 mg x 2 /jour 10 jours
BI C1 B1
Récidives multiples (supérieure à 1)
Vancomycine per os OU Fidaxomicine per os
BII BII
Multiples récidives réfractaires: TF?

Chez l’enfant
COMAI Necker 2014
Schutze GE, Pediatrics. 2013

Cas n°3 • David 9 mois • Pas d’antécédent, vaccinations: Hexavalent, Prevenar 13 • Diarrhée (6-8 selles acqueuses) depuis 48h • Pas de fièvre • Urgences: pèse 7 kg (poids antérieur 7,7kg) • FC 160/min, TA 120/60mmHg
• Diagnostic et prise en charge?

Gastroentérites sévères virales de l’enfant • Rotavirus+++, adénovirus, norovirus • Déshydratation rapide et sévère
• 2 500 000 morts/an dans les pays en développement : plus des 2/3 sont de jeunes enfants
• En France, mortalité faible chez l’enfant (< 40 cas / an) mais deuxième cause d’hospitalisa2on en pédiatrie
• Tous les enfants sont infectés < 5 ans
Cet enfant est en choc hypovolémique


Déshydrata2on sévère (>10%)
à Correc2on rapide des troubles hémodynamiques à sérum physiologique 20 ml/kg débit max,
renouvelable
Le traitement de la déshydrata2on extracellulaire repose sur les cristalloïdes puisque le déficit hydrosodé en est la cause. L’apport de cristalloïdes doit être au moins équivalent aux pertes. Ce n’est qu’en cas de choc persistant que le recours aux colloïdes s’impose (recommanda2ons ANAES).

1- Trocart immobile dans l'os 2- Injection facile de NaCl 0,9% 3- Aspiration de sang +/- moelle 4- Absence de diffusion sous cutanée des solutés
Différents sites sont possibles : ! TIBIA +++ - partie supéro-interne au-dessous
de la grosse tubérosité (âge <ou= 3 ans) - au-dessus malléole interne (âge > 3 ans) ! CONDYLE EXTERNE FEMUR
Ou remplir? Place de l’intra-osseuse « Chaque fois qu'une voie veineuse ne peut être obtenue dans les 5 premières minutes d'une détresse vitale »�

REHYDRATATION ORALE SRO : 1 sachet pour 200 ml d’eau � En principe « ad libitum »: laisser l ’enfant boire ce qu’il veut de la solution du SRO. � En fait, le laisser boire progressivement, par fraction de 50 à 100 ml toutes les 10 à 15 minutes. � Théoriquement, SRO pendant les 4 premières heures : Ê 40 à 50 ml/kg (déshydratation modérée) Ê 50 à 100 ml/kg (déshydratation moyenne) Ê 100 à 150 ml/kg (déshydratation sévère)
Après correction hémodynamique

Cas N° • Prématuré 33 SA, 1,9kg • Reprise alimentation entérale progressive • A J10: T°C 37,4°C, Pâle, Dextro à 13mM, FC 190/min,
abdomen ballonné, arrêt des matières et des gaz • CRP 80/min, PL négative, ECBU négatif, hémoculture +
E. coli • Votre diagnostic?

Forme particulière d’entérocolite grave chez le nouveau né • Entérocolite ulcéronécrosante • Prévalence chez les <1500g: 7% (1-3% total) • 100 plus fréquente chez le pré-terme • Mortalité: 20-30% • Chirurgie fréquente+++ • Complication systémiques majeures
• Répercussion sur développement neuro (25%)

Aspect macroscopique • Atteinte multifocale extensive du grêle et/ou du colon
• Faite de plage de nécrose ischémique et hémorragique à point de départ muqueux " Ulcérations voire perforations digestives
• + pneumatose = infiltration gazeuse sous muqueuse et/ou sous séreuse et/ou dans vaisseaux portes

Physiop thologie ECUN
Neu J NEJM 2011

61
Facteurs favorisants • Prématurité • RCIU • Asphyxie • Détresse respiratoire • Hypotension artérielle • Hypothermie • Cardiopathies cyanogènes. • PCA • KT VO et/ou AO • Polyglobulie • ATB • Anti-acides
• EST • Transfusions sanguines • Infections néonatales • Alimentation hyperosmolaire • Augmentation trop rapide des
rations alimentaires • Indométhacine/ibuprofène • Cocaïne chez la mère • Drogues modifiant la motricité
intestinale
Neu J NEJM 2011 Rôle protecteur du lait maternel

62
Clinique
Signes digestifs : • Intolérance (RG). • Vomissements, Diarrhée. • Distension abdominale • Abdomen tendu • Abdomen DOULOUREUX • Rectorragies • Arrêt du transit • Masse abdominale palpée. • Cellulite pariétale.
Signes généraux : • Détérioration brutale de
l’état général • Apnée, malaise • Détresse espiratoire. • Instabilité thermique. • Hypotonie. • Hypotension artérielle. ⇒ ETAT SEPTIQUE. ⇒ URGENCE MEDICALE
Attention! Évolution très rapide possible, avec passage d’un stade I à un stade III en qq heures

63
Pneumatose intestinale

Attention diagnostic différentiel • ECUN stade II-III
§ Perforation digestive isolée ( = pneumopéritoine SANS pneumatose, peu de s. généraux et dig au début)
§ Volvulus du grêle ( = occlusion à ventre plat, état de choc,
abdomen opaque sans pneumatose) § Sur mésentère commun

65
Score de Bell modifié (Walsh et Kliegman Pediatric Clin North Am 1986;33: 179-201) Stade Signes cliniques et radiologiques
Stade 1a ("pré-
entérite")
Signes généraux: enfant "fatigué", bradycardies, apnées, instabilité thermique Signes digestifs: résidus, vomissements, distension abdominale ASP : normal ou simple dilatation anses
Stade 1b Signes généraux: idem Signes digestifs: idem + Rectorragies ASP: idem 1a
Stade 2a Signes généraux: idem 1b Signes digestifs: idem 1b + absence de bruits intestinaux ASP: distension des anses, iléus, pneumatose
Stade 2b Signes généraux: idem + acidose et thrombopénie modérées Signes digestifs: distension abdominale marquée, paroi inflammatoire ASP: idem 2a + pneumatose portale
Stade 3a
Signes généraux: idem 2b + Choc, apnées-bradycardies sévères, acidose mixte sévère, CIVD Signes digestifs: idem 2b + signes de péritonite, distension abdominale majeure ASP: idem 2b + ascite
Stade 3b Signes généraux: idem 3a Signes digestifs: idem 3a ASP: idem 2b + Pneumopéritoine

66
Traitement médical Dès la suspicion d’ECUN
• Arrêt de l’alimentation + SNG en aspiration douce • Voie veineuse périphérique, puis centrale si ECUN confirmée • Bilan infectieux:CRP, hémocultures aéro-anaérobie et NFS • Antibiothérapie (C3G, Aminosides, Métronidazole) au moins 48h
puis arrêt en fonction du bila, • ASP très régulières les 1eres 48 heures. • Traitement antalgique • Traitement des complications
• Intubation + VAC • Remplissage, amines
• Nutrition parentérale pendant 10 jours si ECUN confirmée • Puis reprise progressive (1/2 ration, LM jusqu’à 100ml/kg/j)
• NB: dans les entéropathies peu sévères (Stade Ia), arrêt alimentation 48h (= période de repos digestif) et reprise à ½ ration

67
Traitement chirurgical • Indications
• Perforations prouvées. • Aggravation de l’état général sous traitement médical. • Occlusion intestinale sur masse.
• Techniques selon la gravité des lésions : • Pas de résections étendues et mutilantes. • Dérivations sans résections. • Résections localisées + entérostomies.
• Rétablissement de la continuité : • 4 à 6 semaines après.

68
Complications secondaires
Court terme • Mortalité ++ • Sténoses intestinales séquellaires
• Cholestase • Fréquente (≈ 30% des
survivants)
• Infraclinique • Risque neurologique
Moyen et Long terme • Troubles du transit • Retard de croissance • Occlusion sur brides avec risque de volvulus
• Risque neuro-développemental

Merci de votre attention