
CONTRAT DE CONSORTIUM OCFIA Réf. … · version code-source et code-objet), les dossiers, plans,...
60
CONTRAT DE CONSORTIUM OCFIA Réf. N°08716A10 ENTRE : La société ASA - Advanced Solutions Accelerator, Société par actions simplifiée (SAS), immatriculée au RCS PARIS B 775 685 019, au capital social de 48 000 euros, N° SIRET 48942238600016, dont le siège est situé 199 Rue de l'Oppidum, 34170, CASTELNAU-LE-LEZ, représentée par son Président et Responsable du Développement, Monsieur Frédéric VIART. Ci-après désignée par la « Société », De première part ET : L'Institut National de la Santé et de la Recherche Médicale, Etablissement Public à caractère Scientifique et Technologique, dont le siège est situé 101 rue de Tolbiac, 75013 - PARIS, représenté par son Directeur Général, Monsieur André SYROTA, et par délégation, par son Administratrice Déléguée Régionale pour la région de Toulouse, Madame Mireille BLANC. Ci après désigné par « INSERM», Agissant au nom et pour le compte de l’Institut de Médecine Moléculaire de Rangueil (I2MR) – U 858 – dirigé par Monsieur Angelo PARINI, Ci-après désigné par l’ « I2MR » De deuxième part ET : L’Université Montpellier 2, Etablissement Public National à caractère Scientifique, Culturel et Professionnel, située Place Eugène Bataillon – 34095 Montpellier Cedex 05, N° SIREN 193 410 883 000 14, code APE 803Z, représentée par sa Présidente, Madame Danièle HERIN, Ci après désignée par « UM2 », ET : Le Centre National de la Recherche Scientifique, Etablissement Public à caractère Scientifique et Technologique dont le siège est 3 rue Michel-Ange 75794 PARIS Cedex 15, N° SIREN 180 089 013 003 95, code APE 7220Z, représenté par son Directeur Général Monsieur Arnold MIGUS lequel a consenti une délégation de signature à Monsieur Bernard JOLLANS, Délégué Régional Languedoc-Roussillon, Ci-après désigné par le « CNRS » L’UM2 et le CNRS agissant tant en leurs propres noms qu’au nom et pour le compte de l’Institut de Mathématiques et de Modélisation de Montpellier (IM3) – UMR 5149 – dirigé par Monsieur Claude CIBILS, Ci-après désigné par l’ « I3M » De troisième part
Transcript of CONTRAT DE CONSORTIUM OCFIA Réf. … · version code-source et code-objet), les dossiers, plans,...
CONTRAT DE CONSORTIUM OCFIA
Réf. N°08716A10
ENTRE : La société ASA - Advanced Solutions Accelerator, Société par actions simplifiée (SAS), immatriculée au RCS PARIS B 775 685 019, au capital social de 48 000 euros, N° SIRET 48942238600016, dont le siège est situé 199 Rue de l'Oppidum, 34170, CASTELNAU-LE-LEZ, représentée par son Président et Responsable du Développement, Monsieur Frédéric VIART.
Ci-après désignée par la « Société »,
De première part ET : L'Institut National de la Santé et de la Recherche Médicale, Etablissement Public à caractère Scientifique et Technologique, dont le siège est situé 101 rue de Tolbiac, 75013 - PARIS, représenté par son Directeur Général, Monsieur André SYROTA, et par délégation, par son Administratrice Déléguée Régionale pour la région de Toulouse, Madame Mireille BLANC.
Ci après désigné par « INSERM»,
Agissant au nom et pour le compte de l’Institut de Médecine Moléculaire de Rangueil (I2MR) – U 858 – dirigé par Monsieur Angelo PARINI,
Ci-après désigné par l’ « I2MR »
De deuxième part ET : L’Université Montpellier 2, Etablissement Public National à caractère Scientifique, Culturel et Professionnel, située Place Eugène Bataillon – 34095 Montpellier Cedex 05, N° SIREN 193 410 883 000 14, code APE 803Z, représentée par sa Présidente, Madame Danièle HERIN,
Ci après désignée par « UM2 », ET : Le Centre National de la Recherche Scientifique, Etablissement Public à caractère Scientifique et Technologique dont le siège est 3 rue Michel-Ange 75794 PARIS Cedex 15, N° SIREN 180 089 013 003 95, code APE 7220Z, représenté par son Directeur Général Monsieur Arnold MIGUS lequel a consenti une délégation de signature à Monsieur Bernard JOLLANS, Délégué Régional Languedoc-Roussillon,
Ci-après désigné par le « CNRS » L’UM2 et le CNRS agissant tant en leurs propres noms qu’au nom et pour le compte de l’Institut de Mathématiques et de Modélisation de Montpellier (IM3) – UMR 5149 – dirigé par Monsieur Claude CIBILS,
Ci-après désigné par l’ « I3M »
De troisième part
Consortium OCFIA
2/60
Ci-après individuellement désignés par la « Partie » et collectivement par les « Parties » TABLE DES MATIERES
ARTICLE PRELIMINAIRE – DEFINITIONS.................................................................................................. 3 ARTICLE 1 – OBJET ET NATURE DU CONTRAT........................................................................................ 4 ARTICLE 2 - DUREE DU CONTRAT................................................................................................................ 4 ARTICLE 3 - MODALITES FINANCIERES .................................................................................................... 5 ARTICLE 4 - MISE EN ŒUVRE DU PROJET................................................................................................. 5 ARTICLE 5 - ORGANISATION DU PROJET .................................................................................................. 5
5.1 COORDONNATEUR ................................................................................................................................. 5 5.2 COMITE DE PILOTAGE ............................................................................................................................ 6
ARTICLE 6 - CONFIDENTIALITE ................................................................................................................... 8 ARTICLE 7 - PUBLICATIONS ET COMMUNICATIONS ............................................................................ 9 ARTICLE 8 - PROPRIETE ................................................................................................................................ 10
8.1 CONNAISSANCES PROPRES................................................................................................................... 10 8.2 RESULTATS PROPRES ........................................................................................................................... 10 8.3 RESULTATS COMMUNS ........................................................................................................................ 10
ARTICLE 9 - EXPLOITATION ........................................................................................................................ 11 9.1 UTILISATION ET EXPLOITATION DES CONNAISSANCES PROPRES ......................................................... 11 9.2 UTILISATION ET EXPLOITATION DES RESULTATS ................................................................................. 12
ARTICLE 10 – RESPONSABILITE AU TITRE DE L’EXECUTION DU PROJET .................................. 13 10.1 RESPONSABILITES ENVERS L’ANR ...................................................................................................... 13 10.2 RESPONSABILITES DES PARTIES ENTRE ELLES ..................................................................................... 14
ARTICLE 11 – RESPONSABILITE EN CAS DE DOMMAGES - ASSURANCES .................................... 14 11.1 DOMMAGES AU PERSONNEL................................................................................................................. 14 11.2 DOMMAGES AUX BIENS........................................................................................................................ 14 11.3 DOMMAGES AUX TIERS ........................................................................................................................ 14 11.4 RESPONSABILITE DU FAIT DES CONNAISSANCES TRANSMISES ............................................................. 14
ARTICLE 12 – DEFAILLANCE D’UN LABORATOIRE.............................................................................. 14 ARTICLE 13 - RESILIATION DU CONTRAT............................................................................................... 15
13.1 RESILIATION PARTIELLE ...................................................................................................................... 15 13.2 RESILIATION TOTALE ........................................................................................................................... 16 13.3 ROLE DU COORDONNATEUR EN CAS DE RESILIATION PARTIELLE OU TOTALE...................................... 16 13.4 DISPOSITIONS COMMUNES ................................................................................................................... 16
ARTICLE 14 - DISPOSITIONS DIVERSES.................................................................................................... 16 14.1 INTUITU PERSONAE.............................................................................................................................. 16 14.2 SOUS-TRAITANCE ................................................................................................................................ 17 14.3 CORRESPONDANCE .............................................................................................................................. 17 14.4 INDEPENDANCE DES PARTIES............................................................................................................... 17 14.5 INTEGRALITE DU CONTRAT.................................................................................................................. 17 14.6 RENONCIATION .................................................................................................................................... 17 14.7 NULLITE D’UNE CLAUSE ...................................................................................................................... 17 14.8 FORCE MAJEURE .................................................................................................................................. 18
ARTICLE 15 – REGLEMENT DES LITIGES ................................................................................................ 18 ANNEXE 1 - PROJET DE RECHERCHE........................................................................................................ 19
ANNEXE 2 - CONNAISSANCES PROPRES DES PARTIES……………………………………………… 20
Consortium OCFIA
3/60
ANNEXE 3 - LISTE DES REPRESENTANTS AU COMITE ………………………………………………21 ETANT PREALABLEMENT RAPPELE QUE Les Parties disposent chacune d’une expérience et de compétences avérées et susceptibles d’être utilisées dans le domaine du calcul scientifique et du traitement des images appliqués à la médecine et à l’industrie. Compte tenu de leur complémentarité dans ce domaine, les Parties ont élaborée le projet OCFIA Optimised Computational Functional Imaging for Arteries (ci-après désigné « PROJET ») afin de répondre à l’appel à Projets CIS 2007 lancé par l’Agence Nationale de la Recherche (ANR). Ce Projet ayant été retenu par l’ANR, les Parties entendent désormais fixer les modalités relatives à l’exécution du Projet ainsi que leurs droits et obligations respectifs en résultant. EN CONSEQUENCE DE QUOI, LES PARTIES ONT CONVENU DE CE QUI SUIT ARTICLE – DEFINITIONS
Dans le présent Contrat, les termes suivants commençant par une lettre majuscule ont les significations respectives suivantes : « ANR » : L’Agence Nationale de la Recherche. « Comité de Pilotage » : Le Comité de Pilotage est défini à l’article 5.2 du présent Contrat. « Connaissances Propres » : Toutes les informations et connaissances techniques et/ou scientifiques, et notamment le savoir-faire, les secrets de fabrique, les secrets commerciaux, les données, logiciels (sous leur version code-source et code-objet), les dossiers, plans, schémas, dessins, formules et/ou tout autre type d’informations, sous quelque forme qu’elles soient, brevetables ou non ,et/ou brevetées ou non et tous les droits y afférents, nécessaires à l’exécution du Projet et appartenant à une Partie ou détenue par elle avant la date d’entrée en vigueur du Contrat et/ou développée ou acquise par elle en parallèle à l’exécution du Contrat et dont elle a le droit de disposer. Les Connaissances Propres des Parties à la date d’entrée en vigueur du Contrat sont précisées de façon exhaustive à l’Annexe 2. Il appartiendra à chacune des Parties d’informer les autres par écrit de l’identification, en cours d’exécution du Contrat, d’autres Connaissances Propres et de justifier, le cas échéant, de l’indépendance de celles-ci vis-à-vis du Contrat. « Contrat » : Le présent contrat et ses annexes. « Coordonnateur » : Le coordonnateur du Projet est défini à l’article 5.1 du présent Contrat. « Informations Confidentielles » : Toutes informations et/ou toutes données sous quelque forme et de quelque nature qu’elles soient incluant notamment tous documents écrits ou imprimés, tous échantillons, modèles et/ou connaissances brevetables ou non, et/ou brevetées et divulguées par une Partie à une ou plusieurs autres Parties au titre du Contrat et sous réserve que la Partie qui divulgue ait indiqué de manière claire et non équivoque leur caractère confidentiel ou, dans le cas d’une divulgation
Consortium OCFIA
4/60
orale, que la Partie qui divulgue, ait fait connaître oralement leur caractère confidentiel au moment de la divulgation et ait confirmé, par écrit, ce caractère dans un délai de trente (30) jours. Les Parties s’accordent pour affirmer que les Résultats constituent bien des Informations Confidentielles. « Laboratoire » : Le ou les laboratoire(s) de recherche rassemblant les moyens humains et matériels destinés à l’exécution du Projet à savoir I2MR et I3M. « Projet » : Le projet de recherche intitulé « Optimised Computational Functional Imaging for Arteries » (OCFIA) et décrit en Annexe 1. « Résultats » : Toutes les informations et connaissances techniques et/ou scientifiques, brevetées ou non, brevetables ou non, y compris les savoir-faire, secrets de fabrique, les secrets commerciaux, les données, logiciels (sous leur version code-source et code-objet), les dossiers, plans, schémas, dessins, formules ou tout autre type d’informations, sous quelque forme qu’elles soient, et tous les droits y afférents, développées par une ou plusieurs Parties dans le cadre du Projet. « Résultats Communs » : Les Résultats développés en commun par plusieurs Parties au titre du Projet et dont les caractéristiques sont telles qu'il n'est pas possible de séparer la contribution de chacune des Parties concernées. « Résultats Propres » : Les Résultats obtenus au cours du Projet par une Partie seule, sans participation financière, scientifique, technique, intellectuelle, matérielle ou autre d’une autre Partie. « Part du Projet » : Les travaux menés par chacune des Parties dans le cadre de la réalisation du Projet et détaillés dans l’Annexe 1.
Les mots au pluriel peuvent s’entendre au singulier et inversement.
ARTICLE 1 - OBJET ET NATURE DU CONTRAT Le présent Contrat a pour objet de définir les modalités d’exécution du Projet et de fixer les droits et obligations respectifs des Parties au regard notamment des droits de propriété intellectuelle portant sur les Résultats. La nature juridique du groupement formé par les Parties au titre du Projet est celle d’un groupement temporaire sans personnalité morale. Les Parties déclarent que le Contrat ne peut en aucun cas être interprété ou considéré comme constituant un acte de société, l’affectio societatis est formellement exclu.
ARTICLE 2 - DUREE DU CONTRAT 2.1 Le Contrat entre en vigueur à sa dernière date de signature.
Il est conclu pour une durée de trente-six (36) mois et prendra rétroactivement effet à la date du 1er janvier 2008.
2.2 Le Contrat peut être prolongé par voie d’avenant, sous réserve d’avoir obtenu l’accord de l’ANR
avant le terme du Projet. 2.3 Nonobstant l’expiration ou la résiliation partielle dans les conditions prévues à l’article 13 du
Contrat, les Parties demeurent liées par les engagements souscrits aux articles 6, 7, 8 et 9.
Consortium OCFIA
5/60
ARTICLE 3 - MODALITES FINANCIERES
Chaque Partie reçoit de l’unité support mandatée par l’ANR, l’aide correspondant à sa Part du Projet, conformément aux dispositions de la décision attributive d’aide notifiée à chaque Laboratoire impliqué. Ces contributions ont fait l’objet de conventions bipartites entre chaque Partie(s) et l’ANR. Les Parties supporteront individuellement le complément de financement nécessaire à l’exécution de la Part du Projet qui leur incombe.
ARTICLE 4 - MISE EN ŒUVRE DU PROJET L’objet du Projet, les objectifs recherchés, la Part du Projet de chacune des Parties, les conséquences attendues aux plans scientifiques et économiques ainsi que le lieu et le calendrier d’exécution du Projet sont détaillés en Annexe 1. Chaque Partie est responsable de l’exécution de sa Part du Projet mis à sa charge, conformément à l’Annexe 1. Pour les besoins du Projet, les Parties s’échangent toutes informations utiles concernant l’état d’avancement de leur Part du Projet qu’elles exécutent et mettent à jour le calendrier général en conséquence. Les Parties décident d’un commun accord de toute modification nécessaire à la bonne exécution du Projet. Les demandes de modification du Projet sont adressées par le Coordonnateur à l’ANR. Les modifications du Projet nécessitant une modification du Contrat feront l’objet d’un avenant au présent Contrat. Les Parties devront se conformer au « Règlement relatif aux modalités d’attribution des Aides de l’Agence Nationale pour la Recherche » du 9 mars 2006.
ARTICLE 5 - ORGANISATION DU PROJET
Le Projet est coordonné par le Coordonnateur et toute décision relative à l’exécution du Projet est prise en Comité de Pilotage.
5.1 Coordonnateur
D’un commun accord entre les Parties, la coordination du Projet est attribuée à l’INSERM (ci-après désigné par le « Coordonnateur ») et l’INSERM désigne Monsieur Hervé ROUSSEAU, pour le représenter dans ses tâches de Coordonnateur. Dans le cas où un empêchement interdirait au Coordonnateur de remplir les obligations qui lui incombent au terme du présent Contrat, les Parties rechercheraient d’un commun accord une solution de substitution. 5.1.1 Rôle du Coordonnateur
Le rôle du Coordonnateur est de coordonner l'action des Parties dans le cadre du Projet et de prendre, après avoir obtenu leur accord via notamment le Comité de Pilotage, toutes les dispositions utiles pour coordonner l'exécution du Projet. Dans le cadre du présent Contrat, le Coordonnateur est l’interlocuteur privilégié entre les Parties et l’ANR et assure, à ce titre, les missions suivantes :
Consortium OCFIA
6/60
- il transmet aux autres Parties les correspondances d’intérêt commun émanant de l’ANR dans un délai raisonnable pour le bon déroulement du Projet ;
- il gère l’archivage et la diffusion des documents logistiques, légaux et administratifs relatifs au Projet ;
- il centralise les comptes-rendus intermédiaires des Parties et les transmet à l’ANR, accompagnés d’une synthèse, tous les six (6) mois.
- il établit, diffuse et met à jour le calendrier général et contrôle son exécution ; - dans le délai de deux (2) mois suivant la date d’expiration du Projet, il adresse un
compte-rendu final unique à l’ANR faisant état de l’ensemble des Résultats issus du Projet ;
- il adresse les demandes de modifications du Projet à l’ANR; - il informe l’ANR des difficultés éventuelles dans la réalisation du Projet, en particulier
lorsque l’une des Parties décide d’abandonner sa Part du Projet ou lorsque les Parties souhaitent qu’un nouvel acteur participe au Projet.
- Il informe les Parties du changement de représentant d’une des Parties au Comité de Pilotage.
5.1.2 Obligations des Parties à l'égard du Coordonnateur
Chaque Partie s’engage à fournir au Coordonnateur, dans les délais impartis, les documents suivants: - les comptes-rendus intermédiaires pour transmission à l’ANR ; - les éléments nécessaires à l’établissement du compte-rendu final unique destiné à
l’ANR ; - les informations permettant de répondre aux éventuelles demandes de l’ANR. Par ailleurs, chaque Partie s’engage à informer le Coordonnateur de toute difficulté dans la réalisation du Projet, en particulier lorsqu’elle envisage d’abandonner sa Part du Projet.
5.2 Comité de Pilotage
5.2.1 Composition du Comité de Pilotage Pour le suivi et l’exécution du Projet et pour assister le Coordonnateur, il est créé un comité de pilotage (ci-après désigné par le « Comité de Pilotage ») composé d’un représentant de chacune des Parties. Le Comité de Pilotage est présidé par le Coordonnateur ou un représentant désigné par lui. Les représentants de chaque Partie peuvent être remplacés à tout moment : la Partie concernée en informe les autres Parties par écrit (fax, courrier ou courriel). Lesdits remplaçants devront être soumis à des obligations de confidentialité au moins équivalentes à celles du présent Contrat. Si nécessaire, et sur convocation écrite, le Comité de Pilotage pourra, d’un commun accord, inviter à l’une de ses réunions : i) tout spécialiste jugé pertinent au regard du Projet, y compris notamment des
spécialistes en propriété industrielle, qu’il soit membre du personnel des Parties ou intervenant extérieur, et / ou,
ii) tout représentant ou interlocuteur scientifique de l’un ou des sous-traitant(s). La liste des représentants au Comité est donnée en Annexe 3.
5.2.2 Missions du Comité de Pilotage
Le Comité de Pilotage a pour mission générale la gestion et le suivi du Projet ; il soumet toutes les propositions nécessaires au bon déroulement du Projet et sera notamment chargé :
Consortium OCFIA
7/60
- de suivre les Parts du Projet en cours et de favoriser les échanges d’informations
entre les Parties dans le cadre de la collaboration ; - d’identifier tout dysfonctionnement, constaté ou probable, et proposer des mesures
appropriées pour les résoudre ; - de valider les informations contenues dans les rapports devant être communiqués à
l’ANR par le Coordonnateur ; - de proposer d’éventuelles adaptations ou ré-orientations scientifiques du Projet, en
fonction des Résultats obtenus et de l'actualité scientifique mondiale, et le cas échéant mettre à jour le calendrier ;
- de coordonner les activités de valorisation (publications, protection, exploitation) et de communication externe relatives au Projet ;
- de préparer et proposer aux Parties toutes décisions nécessitant un avenant au présent Contrat; à ce titre il est entendu que toute modification du Projet qui impliquerait la suppression intégrale ou une modification fondamentale de l’objet de la Part du Projet d’une des Parties, ou toute modification qui augmenterait les charges ou les responsabilités de l’une des Parties, ou la durée du Projet, nécessitera un avenant au présent Contrat ;
- d’agir, en tant que médiateur, afin d’essayer de résoudre tout désaccord entre les Parties lié à l’exécution du Projet ou de leurs obligations au titre du Contrat. Tout désaccord de ce genre pourra être notifié par écrit au Comité de Pilotage par la plus diligente des Parties concernées. Le Comité de Pilotage devra se réunir dans les quinze (15) jours de la notification afin d’essayer de résoudre le différend. Si le Comité de Pilotage ne parvient pas à résoudre le différend à l’unanimité de ses voix dans les quarante-cinq (45) jours de la notification, le différend sera soumis aux directions respectives des Parties concernées.
5.2.3 Fonctionnement du Comité de Pilotage
Le Comité de Pilotage se réunit au moins deux (2) fois par an, et autant de fois que de besoin, à la demande de l’une quelconque des Parties. L’ordre du jour de chaque réunion est transmis aux adresses de correspondance indiquées à l’article 14.3 au minimum deux (2) semaines avant la tenue de la réunion. Les Parties sont convoquées par tout moyen écrit au moins dix (10) jours avant la date de la réunion. La convocation du Comité de Pilotage peut être faite valablement lors de la séance précédente. L'ordre du jour de la séance, non limitatif, est envoyé à titre indicatif par le Coordonnateur avant ladite séance. Chaque réunion fait l’objet d’un compte rendu établi par le Coordonnateur qui est transmis à chacune des Parties dans les quinze (15) jours suivant la date de la tenue de la réunion. Tout compte-rendu doit être approuvé par tous les membres présents à la réunion. Est considéré comme approuvé tout compte-rendu qui n’a pas fait l’objet de remarques dans les quinze (15) jours suivant la réception du projet de compte-rendu. En aucun cas, le Comité de Pilotage ne pourra prendre, au nom des Parties, des engagements autres que ceux prévus dans le Contrat, notamment s’ils peuvent avoir des répercussions sur leur Part du Projet, les coûts et/ou les délais, tels que définis dans le Contrat.
5.2.4 Décisions du Comité de Pilotage Toutes les décisions du Comité de Pilotage sont prises à l’unanimité de ses membres, étant entendu que chaque Partie aura un unique droit de vote de même valeur et, le Comité de Pilotage ne délibère valablement que lorsque la totalité de ses membres est présente ou représentée. Chaque fois que l’unanimité n’est pas atteinte, le Comité de Pilotage réexamine le(s) point(s) de désaccord(s) dans un délai de quinze (15) jours. A défaut d'accord amiable à
Consortium OCFIA
8/60
l’unanimité, l’objet du désaccord est porté à la connaissance des représentants légaux des Parties en vue d’arbitrage. Pour toute décision touchant à la défaillance et à l'exclusion d'une des Parties, le vote de celle-ci ne sera pas autorisé. Les personnes non-membres du Comité de Pilotage citées à l’article 5.2.1 i) et ii) ci-dessus n’auront en aucun cas le droit de prendre part au vote des décisions du Comité de Pilotage et seront tenues de respecter la confidentialité des informations échangées lors des réunions du Comité de Pilotage et devront avoir signé, préalablement à la réunion, un accord de confidentialité conforme aux obligations définies dans le cadre des présentes. Les décisions du Comité de Pilotage ne peuvent en aucun cas modifier les droits et obligations découlant du Contrat. Les Parties consentent à se soumettre à toutes les décisions du Comité de Pilotage. Aucune responsabilité ou charge supplémentaire ne peut cependant être imposée à une Partie sans son consentement.
ARTICLE 6 - CONFIDENTIALITE 6.1 Chaque Partie transmet aux autres Parties les seules Informations qu’elle juge nécessaires à
l’exécution du Projet, sous réserve du droit des tiers. Les Informations transmises par une Partie à une autre Partie, resteront la propriété de la Partie qui les a divulguées. Elles devront être restituées à cette dernière immédiatement sur sa demande.
6.2 Aucune stipulation du Contrat ne peut être interprétée comme obligeant l’une des Parties à
divulguer des Informations à une autre Partie, en dehors de celles qui sont nécessaires à l'exécution du Projet. Chaque Partie s’engage à garder secrètes les Informations de toute nature appartenant aux autres Parties reçues dans le cadre du Contrat. Chaque Partie s’engage à ce que ces Informations : a) soient gardées strictement confidentielles et soient traitées avec le même degré de
protection qu’elles accordent à ses propres informations confidentielles ; b) ne soient utilisées que pour les besoins du Projet; c) ne soient communiquées qu’aux seuls membres de son personnel ayant à les connaître. Chaque Partie s’engage à ce que son personnel visé au c) ci-dessus respecte les dispositions du Contrat. Toute autre communication ou utilisation de ces Informations implique le consentement préalable et écrit de la Partie qui les a communiquées.
6.3 Nonobstant les dispositions ci-dessus, chaque Partie peut communiquer les Informations appartenant aux autres Parties dont elle peut apporter la preuve : - qu’elles étaient disponibles publiquement préalablement à leur communication ou
postérieurement à celle-ci, mais en l’absence de toute faute qui lui soit imputable ; - qu’elles ont été reçues d’un tiers de manière licite ; - qu’elles étaient déjà en sa possession avant leur communication par l’autre Partie ; que l’utilisation ou la divulgation ont été autorisées par écrit par la Partie dont elles
émanent ; - qu’elles ont été développées de manière indépendante et de bonne foi par des personnels
de la Partie qui les reçoit sans qu’ils aient eu accès à ces Informations Confidentielles.
Consortium OCFIA
9/60
6.4 L’obligation de secret est maintenue pendant une période de cinq (5) ans à compter de la
résiliation ou de la survenance du terme du Contrat. ARTICLE 7 - PUBLICATIONS ET COMMUNICATIONS 7.1 Chaque Partie s’engage à ne pas publier de quelque façon que ce soit les Connaissances
Propres appartenant aux autres Parties dont elle pourrait avoir connaissance et ce, tant que ces Informations ne seront pas accessibles au public ou tant que cette Partie n’a pas reçu l’accord préalable de la Partie propriétaire des Connaissances Propres concernées. En revanche, il est entendu que les Résultats Propres pourront être communiqués ou publiés librement pendant la durée du présent Contrat et après l’échéance de celui-ci par la Partie les détenant.
7.2 Les Parties copropriétaires s’engagent à favoriser au maximum la diffusion publique des
comptes-rendus scientifiques du Projet ou de leurs résumés. a) Tout projet de publication ou de communication relatif au Projet ou aux Résultats Communs
doit obtenir, pendant la durée du présent Contrat et les six (6) mois qui suivent son expiration, l’accord écrit des autres Parties copropriétaires qui feront connaître leur décision dans un délai maximum de deux (2) mois à compter de la demande. Passé ce délai et faute de réponse, l’accord sera réputé acquis. Cette décision peut consister à :
- accepter sans réserve le projet ; ou - demander des modifications, en particulier si certaines informations contenues dans
le projet sont de nature à porter préjudice à l’exploitation industrielle et commerciale des Résultats Communs ; ou
- demander à ce que la publication soit différée d’une période maximale de trois (3) mois à compter de la première soumission du projet concerné, si des causes réelles et sérieuses paraissent l’exiger, en particulier si des informations contenues dans le projet de publication ou de communication doivent faire l’objet d’une protection au titre de la propriété industrielle.
b) Le projet de publication ou de communication correspondant doit faire référence au
concours apporté par chacune des Parties à la réalisation du Projet et mentionner l’aide de l’ANR.
c) Si des Informations contenues dans la publication ou la communication doivent faire l’objet
d’une protection au titre de la propriété industrielle, le projet de publication pourra être retardé d’une période maximale de six (6) mois à compter de la date de dépôt de la demande de brevet.
d) En Par dérogation aux stipulations de l’article 7.2a et s’agissant des Résultats Communs
non brevetables susceptibles d’exploitation industrielle, les Parties pourront décider d’un commun accord de constituer un « Dossier Technique Secret » y afférents. Dans ce cas les Parties détermineront par avenant :
- la part des Résultats Communs qui constituera le dossier technique secret et qui, par conséquent, ne pourra pas être publié ;
- le contenu des informations qui ne relèveront pas du dossier technique secret et qui pourront faire l’objet d’une publication ou d’une communication à des Tiers dans les conditions de l’article 7.2a ;
- la durée pendant laquelle le dossier technique restera secret ; - les conditions d’exploitation et les retours financiers relatifs à ces Résultats. e) Les dispositions qui précèdent ne peuvent faire obstacle ni à l’obligation qui incombe aux
chercheurs de produire un rapport annuel d’activité à leurs autorités scientifiques compétentes, ni à la soutenance de thèse d’étudiants chercheurs, sous réserve de respecter si nécessaire des mesures de confidentialité.
Consortium OCFIA
10/60
f) Au-delà d’une période de six (6) mois à compter de l’échéance du présent Contrat, toute communication des Résultats est libre de droit. Toutefois, la ou les Parties désireuses de faire une communication des Résultats en informera préalablement le Coordonnateur.
7.3 Utilisation du nom des Parties
Chaque Partie s’engage à ne pas utiliser, par écrit ou oralement, le nom de l’une des Parties dans quelque but que ce soit, notamment promotionnel (vidéo, plaquette publicitaire, poster, dossier de presse…) et ce quel que soit le support utilisé, sans avoir obtenu l’accord préalable et écrit de la Partie concernée.
ARTICLE 8 - PROPRIETE 8.1 Connaissances Propres
Les Connaissances Propres des Parties demeurent leur propriété respective. Chaque Partie dispose donc librement de ses Connaissances Propres. Aucune stipulation du Contrat ne peut être interprétée comme opérant un quelconque transfert de propriété des Connaissances Propres des Parties. En aucun cas l’une des Parties ne pourra se prévaloir sur la base des Connaissances Propres d’une autre Partie, d’une quelconque concession de licence ou d’un quelconque droit d’auteur ou de possession antérieure selon la définition de la loi française sur les brevets d’invention.
8.2 Résultats Propres Les Résultats Propres sont la propriété de la Partie qui les a générés seule.
8.3 Résultats Communs 8.3.1 Généralités
a) Les Résultats Communs sont la copropriété à parts égales des Parties les ayant
générés, à moins que lesdites Parties s’accordent sur la dévolution des droits de propriété à l’une d’entre elles.
b) La disposition précédente s’applique sous réserve des deux hypothèses suivantes :
- Lorsque les Résultats sont générés par le personnel d’un Laboratoire constitué entre plusieurs Parties, la répartition de la propriété des Résultats entre lesdites Parties est fixée conformément aux accords passés entre elles.
- Lorsque les Résultats sont générés par le personnel de plusieurs Laboratoires constitués entre plusieurs Parties, la copropriété de ces Résultats est répartie entre les Parties tutelles de ces Laboratoires au prorata de leurs apports intellectuels, humains, matériels et financiers respectifs. Les Parties tutelles de chaque Laboratoire font ensuite leur affaire de la répartition entre elles de la quote-part de propriété, conformément aux accords passés entre elles.
c) Tout Résultat Commun consistant en un brevet nouveau, un logiciel ou une autre
connaissance protégée par un droit de propriété intellectuelle, fera l’objet d’un règlement de copropriété, qui sera établi entre les Parties copropriétaires dès que nécessaire et en tout état de cause avant toute exploitation industrielle et/ou commerciale.
8.3.2 Résultats Communs brevetables
Consortium OCFIA
11/60
a) Les Parties copropriétaires de Résultats Communs décideront si ces Résultats doivent faire l’objet de demandes de brevet déposées à leurs noms conjoints et désigneront parmi elles un mandataire chargé des formalités liées au dépôt et à l’administration des brevets ainsi déposés. Les frais de dépôt, d’obtention et de maintien en vigueur des brevets seront supportés par les Parties copropriétaires à hauteur de leur quote-part de propriété.
b) Les Parties copropriétaires se concertent en temps voulu pour établir d’un commun
accord la liste des pays dans lesquels elles déposeront, à leurs noms conjoints, les brevets correspondant au brevet prioritaire qu’elles détiennent en copropriété.
c) Si l’une des Parties copropriétaires renonce à déposer, à poursuivre une procédure
de délivrance ou à maintenir en vigueur un ou plusieurs brevets sur des Résultats Communs en France ou à l’étranger elle devra en informer les autres Parties copropriétaires en temps opportun pour que celles-ci déposent en leurs seuls noms, poursuivent la procédure de délivrance ou le maintien en vigueur à leurs seuls frais et profits. La Partie qui s’est désistée s’engage à signer ou à faire signer toutes pièces nécessaires pour permettre aux autres Parties copropriétaires de devenir seules copropriétaires du ou des brevets en cause. Une Partie copropriétaire sera réputée avoir renoncé au dépôt, à la poursuite de la procédure de délivrance ou au maintien en vigueur d'un brevet, soixante (60) jours après la réception d’une lettre recommandée avec accusé de réception adressée par la ou les autres Parties copropriétaires lui demandant de faire connaître sa décision sur ce point qui est restée sans réponse En outre, il est entendu que la Partie copropriétaire ne saurait se prévaloir d’aucune rémunération au titre de l’exploitation du ou des brevets dans le ou les pays concernés.
d) Chaque Partie copropriétaire fait son affaire de la rémunération éventuelle de ses
inventeurs. ARTICLE 9 - EXPLOITATION 9.1 Utilisation et exploitation des Connaissances Propres
9.1.1 Utilisation par la Partie propriétaire
Chaque Partie dispose librement de ses Connaissances Propres.
9.1.2 Utilisation aux fins d’exécution du Projet Pour les besoins de l’exécution du Projet et à cette seule fin, chaque Partie concède à chacune des autres Parties un droit non exclusif, non cessible, sans droit de sous-licence, et sans contrepartie financière, d'utilisation de ses Connaissances Propres, dans la mesure où ces Connaissances Propres sont nécessaires à l’exécution de sa Part du Projet, à l’exception de toute autre utilisation. Ces Connaissances Propres sont communiquées par la Partie détentrice sur demande expresse d’une autre Partie et doivent être traitées comme des Informations Confidentielles conformément aux termes de l’article 6 du Contrat. Plus particulièrement, lorsque ces Connaissances Propres sont des logiciels, à défaut de stipulations différentes prévues dans un contrat de licence conclu entre les Parties concernées, la Partie qui les reçoit ne peut les utiliser que sur ses propres matériels et n’est autorisée qu’à réaliser la reproduction strictement nécessitée par le chargement, l’affichage, l’exécution, la transmission et le stockage de ces logiciels aux seules fins de son utilisation pour la réalisation de sa Part du Projet, ainsi qu’une copie de sauvegarde.
Consortium OCFIA
12/60
La Partie qui les reçoit s’interdit tout autre acte d’utilisation de ces logiciels et, notamment, tout prêt ou divulgation à des tiers, sauf autorisation préalable de la Partie détentrice, et toute exploitation. Le droit d’utilisation ainsi conféré n’entraîne pas l’accès aux codes sources des logiciels considérés sauf autorisation écrite et préalable de la Partie titulaire des droits sur lesdits logiciels.
9.1.3 Exploitation à des fins commerciales
Chacune des Parties s’engage à concéder aux autres Parties, sur demande expresse de celles-ci et sous réserve des droits des tiers, un droit non exclusif, non cessible, et sans droit de sous-licence, d'exploitation de ses Connaissances Propres nécessaires à la valorisation des Résultats, à des conditions normales et non discriminatoires. Les termes et conditions de cette licence seront négociés préalablement à toute exploitation industrielle et/ou commerciale et feront l’objet d’un contrat de licence conclu entre les Parties concernées. Plus particulièrement, lorsque ces Connaissances Propres sont des logiciels, la Partie qui les reçoit ne pourra les utiliser que sur ses propres matériels et ne sera autorisée qu’à réaliser la reproduction strictement nécessitée par le chargement, l’affichage, l’exécution, la transmission et le stockage de ces logiciels aux seules fins de son utilisation pour l’exploitation de ses Résultats, ainsi qu’une copie de sauvegarde.
9.2 Utilisation et exploitation des Résultats 9.2.1 Principes généraux
Chaque Partie peut librement utiliser, exploiter et/ou faire exploiter ses Résultats Propres. Les Parties s’engagent à prendre toutes les mesures appropriées, notamment à l’égard de leurs employés et/ou de leurs sous-traitants éventuels, leur permettant d’accorder aux autres Parties des droits d’utilisation et d’exploitation des Résultats Propres ou Résultats Communs, dans les conditions prévues au Contrat.
9.2.2 Utilisation aux fins d’exécution du Projet
Chacune des Parties concède aux autres Parties un droit non exclusif, non cessible, sans droit de sous-licence, et sans contrepartie financière, d'utilisation de ses Résultats Propres et de ses Résultats Communs aux seules fins de l’exécution de leur Part du Projet. Les conditions d’exercice de ce droit d’utilisation sont les mêmes que celles prévues à l’article 9.1.2 ci-dessus pour l’utilisation des Connaissances Propres.
9.2.3 Utilisation à des fins de recherche
Chaque Partie peut utiliser librement et gratuitement, sur sa demande, les Résultats Propres et les Résultats Communs des autres Parties pour ses seuls besoins propres de recherche et dans le cadre de collaboration de recherche avec des tiers, à l’exclusion de toute utilisation, directe et/ou indirecte, à des fins commerciales. Si les Résultats ainsi demandés constituent des logiciels, leur remise fait l’objet d’un accord écrit entre les Parties concernées qui en précise les conditions et modalités d’utilisation, étant entendu que les droits d’utilisation ainsi conférés n’entraînent pas l’accès aux codes sources, sauf accord exprès de(s) la Partie(s) (co)propriétaire(s).
9.2.4 Exploitation des Résultats Communs a) Les Parties copropriétaires des Résultats Communs préciseront leurs modalités
d'exploitation dans le cadre d’un accord de valorisation avant toute exploitation industrielle et commerciale ou, dans l’hypothèse de brevets nouveaux en copropriété dans le cadre du règlement de copropriété mentionné à l’article 8.3.1 c) ci-dessus et dans le respect des principes définis au présent Contrat. Il est d’ores et déjà convenu
Consortium OCFIA
13/60
entre les Parties que toute exploitation directe et/ou indirecte par une Partie copropriétaire des Résultats Communs impliquera une compensation financière au profit des autres Parties copropriétaires, selon les conditions et modalités définies ultérieurement dans l'accord de valorisation ou de règlement de copropriété susmentionnés. Lorsque les Résultats Communs consistent en des logiciels, l’accord préalable des autres Parties copropriétaires sera requis si l’exploitation envisagée entraîne la communication de codes sources.
b) Si aucune des Parties copropriétaires ne souhaite ou ne peut exploiter les Résultats
Communs, et selon les principes d’exploitation définis par les Parties copropriétaires, les autres Parties peuvent se porter candidates à l’exploitation desdits Résultats Communs. Dans un tel cas, si des Parties non copropriétaires ont fait part de leur intérêt pour obtenir des droits d’exploitation des Résultats Communs, les termes et conditions (notamment les conditions financières) de cette exploitation seront arrêtés au cas par cas dans un accord écrit spécifique.
c) Si aucune Partie ne souhaite ou ne peut exploiter les Résultats Communs, et selon
les principes d’exploitation définis par les Parties copropriétaires, les Parties copropriétaires pourront rechercher des tiers pour l’exploitation desdits Résultats Communs. Dans ce cas, un contrat de licence sera établi entre les Parties copropriétaires des Résultats Communs et le(s) licencié(s).
9.2.5 Exploitation des Résultats Propres et des Résultats Communs par une Partie non
(co)propriétaire
Chaque Partie propriétaire ou copropriétaire s'engage, pendant une durée de dix-huit (18) mois à compter de la date d’expiration ou de résiliation du Contrat et sous réserve des droits consentis à des tiers et de ses intérêts légitimes, à concéder à toute autre Partie qui en ferait la demande, un droit non exclusif, non cessible, sans droit de sous-licence d'exploitation de ses Résultats Propres dès lors qu’elles seraient nécessaires à l’exploitation des Résultats de la Partie qui fait la demande. Ce droit sera concédé à des conditions normales et non discriminatoires. Les termes et conditions de la licence seront négociés préalablement à toute exploitation industrielle et/ou commerciale et feront l’objet d’un contrat de licence conclu entre les Parties concernées. Dans le cas de logiciels, la Partie qui les reçoit ne pourra les utiliser que sur ses propres matériels et ne sera autorisée qu’à réaliser la reproduction strictement nécessitée par le chargement, l’affichage, l’exécution la transmission et le stockage de ces logiciels aux seules fins de l'exploitation de ses Résultats, ainsi qu’une copie de sauvegarde. Dans l’hypothèse où aucune licence n’aurait été conclue entre les Parties dans les conditions ci-dessus, à l'issue d’un délai de dix-huit (18) mois à compter de la date d’expiration ou de résiliation du Contrat, l’engagement susvisé prendra fin et la Partie propriétaire ou copropriétaire des Résultats se retrouvera libre de les exploiter et/ou de les faire exploiter à titre exclusif, sous réserve de l’accord des autres Parties copropriétaires dans le cas des Résultats Communs.
ARTICLE 10 – RESPONSABILITE AU TITRE DE L’EXECUTION DU PROJET 10.1 Responsabilités envers l’ANR
Chaque Partie exécutera sous sa seule et entière responsabilité la totalité des tâches correspondant à sa Part du Projet, telle que décrite en Annexe 1. Chaque Partie n’est responsable que de sa Part du Projet et ne peut en encourir de responsabilité au titre des Parts du Projet des autres Parties.
Consortium OCFIA
14/60
10.2 Responsabilités des Parties entre elles Les Parties renoncent mutuellement à se demander réparation des préjudices indirects (perte de production, d’intérêts, manque à gagner, etc.).
ARTICLE 11 – RESPONSABILITE EN CAS DE DOMMAGES - ASSURANCES 11.1 Dommages au personnel
Chaque Partie prend en charge la couverture de son personnel conformément à la législation applicable dans le domaine de la sécurité sociale, du régime des accidents du travail et des maladies professionnelles, et procède aux formalités légales qui lui incombent. La réparation des dommages subis par ces personnels, du fait ou à l'occasion de l'exécution du Contrat s'effectue donc à la fois dans le cadre de la législation relative à la sécurité sociale et au régime des accidents du travail et des maladies professionnelles et dans le cadre de leur statut propre.
11.2 Dommages aux biens Chacune des Parties conserve à sa charge sans recours contre une autre Partie, sauf cas de faute lourde ou intentionnelle, la réparation des dommages subis par ses biens propres du fait ou à l'occasion de l'exécution du Contrat. Si une police d’assurance de dommages est souscrite pour garantir lesdits biens, elle devra comporter une clause de non recours en faveur de chacune des Parties et de leurs éventuels assureurs.
11.3 Dommages aux tiers Chacune des Parties est responsable suivant les règles du droit commun des dommages de toute nature causés aux tiers dans le cadre de l’exécution du Contrat.
11.4 Responsabilité du fait des connaissances transmises
a) Les connaissances fournies par une Partie au titre du présent Contrat devront être des informations exactes selon le meilleur jugement et l'état des connaissances de cette Partie, cependant aucune garantie explicite ou implicite n'est donnée par cette Partie sur l'exactitude réelle des connaissances.
b) Les Parties conviennent par les présentes que l'utilisation des connaissances par elles ou
par toute personne qui recevra les connaissances de cette Partie se fera totalement aux risques de la Partie qui les reçoit, et chaque Partie convient par les présentes renoncer à tout recours à l’encontre de l'autre Partie au titre des réclamations faites par toute personne en raison de l'utilisation de ces connaissances par elle-même ou par toute personne à laquelle elle a transmis ces connaissances, et notamment en matière d’action en contrefaçon à l’encontre de brevets et autres droits d’auteur appartenant à des tiers.
ARTICLE 12 – DEFAILLANCE D’UN LABORATOIRE 12.1 La défaillance, pour une raison quelconque, de l’un des Laboratoires du Projet ne remet pas en
cause le caractère collectif du Projet. Au cas où l’un des Laboratoires ne serait plus en mesure d’assurer l’exécution de sa part de Projet, pour une raison quelconque, le Comité de Pilotage se réunira afin de déterminer si le Laboratoire défaillant est exclu de l’exécution du Projet et, si tel est le cas, trouver une solution de substitution, sous réserve de l’accord de l’ANR.
12.2 Les Parties pourront notamment proposer :
a) soit de répartir la Part du Projet incombant au Laboratoire défaillant entre les autres Laboratoires impliqués.
Consortium OCFIA
15/60
b) soit de confier la Part du Projet incombant au Laboratoire défaillant à un autre laboratoire,
rattaché ou non à une Partie. La ou les Partie(s) tutelle(s) dudit Laboratoire étant alors subrogé(s), sous réserve de l’établissement d’un avenant, dans tous les droits et obligations dont disposait la ou les Partie(s) sortante(s). Dans une telle hypothèse, les droits et/ou obligations de la nouvelle Partie seront identiques à ceux dont bénéficiaient et/ou auxquels était soumis la Partie tutelle du Laboratoire défaillant à la date effective de la résiliation, en ce compris notamment:
i) le droit de bénéficier de tous les droits de propriété intellectuelle résultant de la Part du
Projet réalisée dans le cadre du Contrat et détenus jusqu'alors par la Partie tutelle du laboratoire défaillant sous réserve de participer aux frais de dépôt des titres de propriété industrielle en cours de dépôt, de maintien et d'extension des titres déposés ;
ii) l'obligation de réaliser la Part du Projet confiée à la Partie tutelle du Laboratoire défaillant dans les conditions juridiques et techniques prévues dans le Contrat.
c) soit d’avoir recours à un sous-traitant. 12.3 Après validation de cette solution par l’ANR, la Partie tutelle du Laboratoire défaillant devra
remplir les obligations souscrites, et notamment payer les sommes dues, jusqu'à prise d'effet de l’exclusion du Laboratoire défaillant. En outre : a) elle communiquera immédiatement et gratuitement aux autres Parties et à son éventuel
remplaçant, un rapport reprenant l’ensemble des Résultats de la Part du Projet de ce Laboratoire réalisés jusqu’à la date d’exclusion et en demeurera responsable.
b) elle laissera à la disposition des autres Parties, les installations, matériels et prestations qui
auront fait l'objet d'un financement au titre du Projet, dans des conditions restant à définir. c) les licences et droit d’utilisation concédés par cette Partie aux autres Parties sur ses
Connaissances Propres et Résultats au titre du présent Contrat demeureront en vigueur. d) elle n’aura plus aucun droit en tant que tutelle du Laboratoire défaillant sur les licences qui lui
auraient été concédées par les autres Parties sur les Connaissances Propres ou sur les Résultats de ces dernières ; ces licences prendront fin immédiatement et automatiquement à la date effective de l’exclusion.
12.4 Toute modification de la répartition des Part du Projet entre les Parties se fera par voie
d’avenant.
ARTICLE 13 - RESILIATION DU CONTRAT 13.1 Résiliation partielle
a) En cas d'inexécution par une des Parties d’une ou plusieurs de ses obligations substantielles au titre du Contrat et suite à la demande de l’ANR ou d'une des Parties, la constatation de la défaillance sera soumise au vote du comité de pilotage, la Partie défaillante ne participant alors pas au vote. En cas de reconnaissance de la défaillance par le comité de pilotage, le Coordonnateur, ou la Partie désignée par le comité de pilotage si le Coordonnateur est la Partie défaillante, pourra mettre en demeure la Partie d'exécuter les dites obligations par lettre recommandée avec accusé de réception. Le Contrat sera partiellement résilié à l’égard de la Partie défaillante dans un délai de un (1) mois suivant la réception de la lettre, à moins que dans ce délai la Partie défaillante n'ait satisfait à ses obligations ou n’ait apporté la preuve d’un empêchement consécutif à un cas de force majeure. L'exercice de cette faculté de résiliation ne dispense pas la Partie défaillante de remplir les obligations contractées jusqu'à la date de prise d'effet de la résiliation.
Consortium OCFIA
16/60
b) Chaque Partie dispose du droit de se retirer du Projet avec l’accord préalable des autres Parties et de l’ANR, sous réserve d’un préavis de trois (3) mois.
c) Par ailleurs, les Parties pourront décider, sous réserve de l’accord de l’ANR, de l’exclusion,
de plein droit, d’une Partie qui se trouverait dans une des situations suivantes : • désistement ou exclusion du seul Laboratoire dont elle a la tutelle, • cession totale ou partielle, à moins que le repreneur reprenne les droits et obligations
liés au présent accord avec l’approbation du Comité de Pilotage et des autres Parties, • redressement ou de liquidation judiciaire, sauf si l'administrateur, après mise en
demeure, exige l'exécution du présent Contrat conformément aux articles L. 622-13 et L. 641-10 du Code de commerce,
• cessation d'activité ou de dissolution. d) Dans tous ces cas, le Comité de pilotage est alors réuni pour réfléchir à une solution de
substitution qui sera soumise à l’accord de l’ANR et constatée par avenant. e) La Partie sortante communiquera gratuitement à son remplaçant dès notification de la
résiliation partielle, tous les dossiers et informations relatifs au Projet, et laissera à sa disposition les installations, matériels et prestations qui auront fait l'objet d'une aide au titre du Projet. Les licences concédées par la Partie sortante au titre du présent Contrat, y compris les licences sur ses Connaissances Propres, seront maintenues pour la durée qui leur est propre et les engagements pris de concéder des licences continueront de s'imposer à la Partie sortante. En revanche, les licences concédées à la Partie sortante par les autres Parties prendront fin de plein droit dès réalisation de la résiliation partielle mentionnée ci-dessus.
13.2 Résiliation totale
Le Contrat pourra être résilié de plein droit à l’encontre de toutes les Parties sur décision unanime du Comité de Pilotage. Dans ce cas, chaque Partie fera son affaire personnelle de tout éventuel remboursement de subvention ou d’avance réclamé par l’ANR. Sauf accord contraire écrit des Parties , le Contrat sera automatiquement résilié en cas de décision de l’ANR d’arrêter le financement du Projet.
13.3 Rôle du Coordonnateur en cas de résiliation partielle ou totale Le Coordonnateur (ou toute autre partie désignée si la Partie défaillante ou qui se retire est le Coordonnateur) demandera à l’ANR une modification de l’attribution des aides correspondant à la nouvelle répartition des charges de travail.
13.4 Dispositions communes En cas de résiliation anticipée, totale ou partielle, du Contrat, les dispositions des articles 13, 14 et 15 demeureront en vigueur et s’appliqueront aux Résultats partiels obtenus jusqu’à la date de résiliation.
ARTICLE 14 - DISPOSITIONS DIVERSES 14.1 Intuitu Personae
Le Contrat a de convention expresse et déterminante entre les Parties un caractère intuitu personae. En conséquence, aucune Partie n'est autorisée à transférer à un tiers tout ou partie des droits et obligations qui en découlent pour elle, sans l'accord préalable et écrit des autres Parties et de l’ANR.
Consortium OCFIA
17/60
14.2 Sous-Traitance Pour les besoins du Projet et sous réserve de l’accord des autres Parties, chaque Partie peut sous-traiter à un tiers une partie de sa Part du Projet. Chaque Partie s’engage à imposer contractuellement à ses sous-traitants le respect des conditions du Contrat et reste responsable de la réalisation de sa Part du Projet qu’elle sous-traite à un tiers. De plus, tout accès par le sous-traitant aux Connaissances Propres ou Résultats d’une autre Partie sera subordonné à l’accord préalable écrit de la ou les Parties qui en est(sont) propriétaire(s). Le contrat de sous-traitance doit être établi dans des termes compatibles avec ceux du Contrat. A ce titre, chaque Partie s'engage à acquérir les droits de propriété intellectuelle des résultats obtenus par ses sous-traitants dans le cadre du Projet.
14.3 Correspondance Toute correspondance à raison de l’exécution du présent Contrat devra être effectuée aux adresses suivantes : • Pour la Société, à l’attention de :
• Vincent Bosquier Directeur Technique, ASA - Advanced Solutions Accelerator 199, Rue de l'Oppidum 34170 CASTELNAU LE LEZ
• Pour l’INSERM, à l’attention de : M. Hervé Rousseau, I2MR, CHU de Rangueil, 1 Av. Jean Poulhès, Bât L3, BP31432, Toulouse Cedex · Avec copie à : M. Angelo Parini et M. Ramiro Moreno, même adresse
• Pour l’UM2, à l’attention de : • M. Franck Nicoud, Université Montpellier 2 – Laboratoire I3M Cc/051 – Place Eugène
Bataillon – 34095 MONTPELLIER Cedex 5 - • Avec copie à : • Université Montpellier 2 – Service des Conventions Cc/428 – Place Eugène Bataillon –
34095 Montpellier Cedex 5.
14.4 Indépendance des Parties
Le Contrat ne doit en aucun cas être interprété comme créant une relation d’association ou une société, même de fait, entre les Parties, chacune d’elles devant être considérée comme cocontractants indépendants.
14.5 Intégralité du Contrat
Le présent Contrat contient l'intégralité des termes et conditions sur lesquels les Parties se sont mises d'accord. Il annule et remplace tous documents ou accords préalables relatifs à son objet. Toutes modifications qu'il s’avérerait nécessaire d'apporter au Contrat seront décidées ou arrêtées d'un commun accord entre les Parties et feront l'objet d'un avenant écrit au Contrat.
14.6 Renonciation Le fait, par l'une ou l'autre des Parties d'omettre en une ou plusieurs occasions de se prévaloir d'une ou plusieurs dispositions du Contrat, ne pourra en aucun cas impliquer renonciation par la Partie intéressée à s'en prévaloir ultérieurement.
14.7 Nullité d’une clause Dans l'hypothèse où une ou plusieurs des dispositions du Contrat serait contraire à une loi ou à un texte légalement applicable, cette loi ou ce texte prévaudrait, et les Parties feraient les
Consortium OCFIA
18/60
amendements nécessaires pour se conformer à cette loi ou à ce texte. Toutes les autres dispositions resteraient en vigueur et les Parties feraient leurs meilleurs efforts pour trouver une solution alternative acceptable dans l'esprit de ce contrat.
14.8 Force majeure Aucune des Parties ne pourra se prévaloir à l'encontre de l'autre, notamment sur le plan des délais, de la non-exécution d'obligations due à la force majeure ; on entend par force majeure tous les événements indépendants de la volonté des Parties, imprévisibles ou, s'ils ne sont pas imprévisibles, inévitables, intervenus après l'entrée en vigueur du contrat, et empêchant l'exécution, en tout ou partie, des obligations qui en dérivent, tels que grèves, événements atmosphériques exceptionnels, impossibilité d'obtenir ou hausse substantielle du coût des matières premières, de l'énergie, de la main-d'œuvre, pannes des machines nécessaires à la fabrication, défaut des sous-traitants, ou acceptation de commandes antérieures, faits de guerre, émeutes, incendies, cataclysmes naturels ...
ARTICLE 15 – REGLEMENT DES LITIGES
Tout litige ou différend entre les Parties relatif à l’interprétation et/ou l’exécution et/ou la résiliation et/ou à la validité du Contrat (ou de l’une quelconque de ses clauses) qui n’aurait pu être réglé amiablement au sein du Comité de Pilotage sera soumis aux tribunaux français compétents.
Fait en quatre (4) exemplaires originaux rédigés en français Pour ASA Pour l’Université Montpellier 2 Fait le …………… Fait le …………… A …………… A ……………. _________________________ ________________________ Madame Danièle HERIN Présidente Pour l’INSERM Pour le CNRS Fait le …………… Fait le ……… A Paris A Montpellier _________________________ ----------------------------------------- Madame Mireille BLANC Monsieur Bernard JOLLANS Administratrice Déléguée Régionale Délégué Régional Languedoc-Roussillon
Consortium OCFIA
19/60
ANNEXE 1 - PROJET DE RECHERCHE
Résumé du projet en français
Les pathologies vasculaires sont multifactorielles et spécifiques à chaque patient. L’initiation et la progression d’un anévrisme, d’une dissection ou d’une sténose restent des phénomènes difficiles à comprendre. Pour ces raisons, et parce que l’athérosclérose représente la principale cause de décès dans les pays développés, la recherche dans ce domaine est cruciale. Une meilleure compréhension de la physiopathologie et une augmentation du taux de guérison est possible, à condition d’avoir accès à l’imagerie fonctionnelle de type biomécanique permettant d’évaluer les contraintes mécaniques dont les vaisseaux sont le siège. La puissance de calcul des nouveaux ordinateurs permet actuellement d’effectuer des simulations numériques complexes, notamment de type Mécanique des Fluides Numériques (MFN), utiles dans l’industrie et dans la recherche pour optimiser la conception de nouveaux systèmes ou mieux comprendre certains phénomènes mal maîtrisés. Le cadre général du programme Optimised Computational Functional Imaging for Arteries (OCFIA) est l’introduction du calcul scientifique haute performance dans le monde médical afin de rationaliser les décisions thérapeutiques associées à certaines maladies vasculaires mal comprises. Plus précisément, il s’agit de coupler les techniques d’imagerie médicale, essentiellement morphologiques, et le calcul scientifique, à travers la MFN, afin de produire de l’imagerie fonctionnelle fournissant aux praticiens une meilleur connaissance quantitative des paramètres biomécaniques (champ de vitesses, de pression, de contraintes, …) des patients. Plusieurs facteurs rendent nécessaire l’utilisation de calcul hautes performances (CHP) pour atteindre cet objectif : a) les fonctions biomécaniques doivent être produites sur un territoire vasculaire important ; la dissection aortique couvre en effet souvent la totalité de l’aorte thoracique et s’étend jusque dans l’aorte abdominale, b) les équations sous-jacentes à résoudre (Navier-Stokes avec rhéologie à effet mémoire dans une géométrie complexe et variable en temps) sont complexes et fortement non linéaires, c) cette approche ne sera utile aux patients et aux praticiens qui les soignent que si le temps de restitution de la chaîne complète, des données médicales brutesà l’imagerie fonctionnelle, est inférieur à quelques heures. La plupart des simulations d’écoulements sanguins réalisées jusqu’à présents l’ont été sur des modèles in vitro théoriques ou in vivo avec une hypothèse de paroi rigide, voire linéaire élastique homogène isolée de toute contrainte extérieure. En d’autres termes, les simulations hémodynamiques réalisées à ce jour ne prennent pas en compte les variations physiologiques de la géométrie artérielle, négligeant ainsi l’effet pourtant majeur qu’elles ont sur l’écoulement sanguin. Dans ce cadre, le projet vise à relever un double défi : 1) faire le pas vers une prise en compte des variations géométriques physiologiques, des conditions limites pulsées et de la rhéologie sanguine lors de la simulation de l’écoulement sanguin dans les vaisseaux, 2) mettre au point une chaîne de traitement complète et optimisée
Consortium OCFIA
20/60
(OCFIA) des données médicales brutes produisant de l’imagerie fonctionnelle biomécanique d’une qualité suffisante et en un temps suffisamment court pour constituer une véritable aide au diagnostic et à la décision thérapeutique.

Consortium OCFIA
21/60
Summary in English
Vascular pathology is multi-factorial and patient specific. The initiation and the progression of an aneurysm, of a dissection or of a stenosis still remain difficult to grasp. For these reasons, and also because atherosclerosis represents the major cause of death in the developed nations, research in this domain is crucial. A better comprehension of the physiopathology and an increase of the cure rate are possible, provided we have access to functional bio-mechanic imaging thus allowing evaluation of the mechanical constraints in vessels. Currently, the calculation power of new computers allows the carrying out complex numerical simulations e.g. in Computational Fluids Mechanic (CFD), useful in industry and in the research field to optimize the conception of novel systems, and to better apprehend poorly mastered issues. The general framework of the Optimised Computational Functional Imaging for Arteries (OCFIA) program is to introduce high-performance scientific computing in the medical domain with the aim to rationalize therapeutic decisions in respect to vascular diseases yet poorly understood. More precisely, it consists in coupling medical imaging techniques, essentially morphological, with scientific computing, through CFD, to yield functional imaging, thus providing to physicians a better quantitative knowledge of the biomechanical state (field of speeds, pressure, loads ...) to the patients. Several factors make it necessary to resort to high performance computing (HPC) to achieve this objective: a) the biomechanical functions must be produced on an important vascular territory; aortic dissection actually often covers the whole thoracic aorta and spreads itself even in the abdominal aorta, b) the inherent equations to be resolved (time-dependent Navier-Stokes which takes into account the memory effect of the rheology, within a complex geometry system) are very intricate and non linear. c) this approach will only be useful to the patients and to their physicians if the restitution time of the complete chain is less than a few hours. Most of the blood-flow simulations conducted so far on theoretical in vivo or in vitro models have been based on the rigid-walls hypothesis, or assumed homogenous, linear elastic arteries, isolated from any exterior constraint. In other terms, hemodynamic simulations realized so far do not take into account the physiological variations of arterial geometry, hence neglecting the nonetheless major effect they have on blood flow. In this particular context, this project aims at addressing a double challenge: 1) make a step towards the tackling of physiological geometric variations, the pulsated limit conditions and blood rheology during the simulation of blood flow in vessels, 2) to settle a complete and optimized chain of treatment (OCFIA) for raw medical data and producing bio-mechanic functional imaging of fair quality within sufficient short time-laps for coherent therapeutic insight.
Consortium OCFIA
22/60
Introduction
Risk factors for cardiovascular disease (hypertension and high cholesterol) and their role have been identified, but cannot explain the observed localised occurrence and the progression of the disease (stenosis, aneurysm rupture, aortic dissection). Currently, available techniques such as Computed Tomography (CT), Magnetic Resonance Imaging (MRI) and Ultrasound (US) do not allow accurate determination of the complex velocity distribution and biomechanical load on the arterial wall. Nevertheless there is not any doubt that medical imaging is an essential tool for the understanding of these pathological processes. Cardiovascular disease is clearly multi-factorial and it has been shown that deviations of the normal velocity field (changes in wall shear stress) play a key role [1]. Despite many hemodynamic studies carried out with models of arterial bifurcations, especially the carotid artery bifurcation, the precise role played by wall shear stress (WSS) in the development and progression of atherosclerosis remains unclear. Still, it is certain that the mechanical load induced by the fluid on atherosclerotic plaques and their surrounding tissues is of the utmost importance for predicting future rupture (culprit plaques) and preventing ischemic events [2],[3]. In the same way, the risk of rupture of an aortic abdominal aneurysm (AAA) depends more on biomechanical factors than simply on the aneurysm diameter. Although clinical decisions are based only on the latter today, wall tension is a significant predictor factor of pending rupture [4]. Computational Fluid Dynamics (CFD) techniques can provide extremely detailed analysis of the flow field and wall stress (shear & tensile) to very high accuracy. New advances in simulation techniques could make a significant contribution to a better quantitative knowledge of the biomechanical condition of the arteries and lead to a new understanding via deepened insights into these conditions. Advanced simulations could potentially be used for predicting plaque and aneurysm rupture, improving endovascular prosthesis design, as well as for guiding treatment decisions by predicting the outcome of interventional gesture (i.e. stent-coil technique). However, applying computational fluid dynamics (CFD) to actual pathological regions of the arterial tree is very challenging and has never been done so far with sufficient accuracy and time efficiency to be useful in the clinical practice. Several reasons can be put forward to explain this:
• the blood rheology is complex and, once coupled to flow motion equations, leads to a set of strongly coupled, highly non-linear set of partial differential equations which is far less understood than the classical Navier-Stokes system,
• the fluid-structure problem is very stiff because the blood to arterial tissue density ratio is close to unity; from an algorithmic point of view, this means that the fluid and structure equation must be advanced simultaneously in time, leading to potentially costly methods,
• the arterial wall rheology is essentially unknown and hardly measurable because pathology and patient specific; uniform linear elasticity is most often assumed as a first step, but no reliable data are available to produce the second step,
Consortium OCFIA
23/60
• the external load to which the artery is submitted to is unknown, • hemodynamic data with sufficient time and space resolution are hardly measureable
under in vivo conditions, although they are necessary to feed the CFD simulations with realistic boundary conditions,
• accurate geometrical data about the arterial region require advanced medical imaging systems that are only available in radiology department of hospitals whose first objective is to host and treat patients and where neither the computing science nor the computational mechanics are part of the common expertise and background.
To overcome most of the above mentioned difficulties, the Optimised Computational Functional Imaging for Arteries (OCFIA) project aims at proposing and assessing a new methodology where advanced medical imaging techniques and CFD methods are inter-connected in order to obtain biomechanical data related to the blood flow under realistic and physiological conditions. We present a complete, optimized calculation chain (Optimized Computational chain for Functional Imaging in Arteries thereafter the OCFIA chain) whose input come from an entirely non-invasive 4D MRI protocol that provides time varying geometry and flow rates and output is a functional imaging description of the arterial tree region of interest. The present consortium has been designed in order to put together experts in vascular pathology and medical imaging (I2MR), computational fluid dynamics and mathematical modelling (I3M) and computer science and high performance computing (HPC) and software optimisation (ASA). Four work-packages have been devised in order to organize the research effort towards the development and application of the OCFIA chain to actual patients in the clinical environment.
Contexte et état de l’art / Context and state-of-the art
In the cardiovascular engineering community, considerable progress has been made towards combining simulations with imaging techniques for subject-specific flow simulations. A number of studies incorporating anatomical images into flow models have been shown to be capable of providing detailed velocity and wall shear stress for anatomically realistic arteries. A review of the progress made in the area of image-based computational modelling in large arteries has been given by Steinman [5]. Most of these simulations considered steady-state flow which in some cases gives reasonable approximations to the wall shear stress. Studies with realistic pulsatile flow conditions require detailed medical data on the blood pressure and the pulse waveform and appropriate numerical treatments in the CFD code. Only a very small part of the published studies accounts for the effects of the blood flow domain time variations. The activity of three major groups in the field of computational hemodynamics over unsteady geometries are shortly described in the following: .
• In the USA, research in cardiovascular biomechanics in the field of numerical simulations based on 4D MRI takes already great steps. Indeed, the Georgia Tech and Emory University researchers have developed an innovative new technology that
Consortium OCFIA
24/60
will help pediatric cardiac surgeons designing and testing a customized surgical procedure before they ever pick up a scalpel. With a better understanding of each child’s unique heart defect, surgeons could greatly improve the likelihood that children with complex defects requiring multiple surgeries over a period of several years could have smoother recoveries and an improved quality of life after their operations. The technology, known as image-based surgical planning and developed with the help of pediatric cardiologists and pediatric surgeons at The Children’s Hospital of Philadelphia and Emory University, creates a three-dimensional model of the child’s heart with data from the child’s MRI scans at different times in the cardiac cycle, also called a 4-D MRI. The models allow surgeons to visualize the direction of blood flow and determine any energy loss in the heart. So if a surgeon was planning a certain correction to an area of a child’s heart, a model created by the system would show the surgeon how well blood would flow through the newly configured heart. The goal of the Georgia Tech/Emory project is to create a complete system that allows surgeons to get a detailed look at the child’s heart functions with the new MRI system, design surgical procedures for optimum postoperative performance and evaluate the heart’s performance with a sophisticated blood flow computer simulation. The work was presented last month at the American Heart Association’s Scientific Sessions meeting in Chicago (nov. 2006) and has been published in Circulation and the Annals of Thoracic Surgery. Other examples in the USA confirm this tendency to combine medical imaging with CFD seeking to meet the needs for applicable functional imaging on clinical applications.
• In France, the team of J-F Gerbeau at INRIA Rocquencourt develops advanced
algorithms for solving the fluid-structure interaction problems [34,35]. This issue is particularly difficult to face when the fluid added mass acting on the structure is strong, as it happens in hemodynamics for example. Indeed, several works have shown that, in such situations, implicit coupling is necessary in order to avoid numerical instabilities, the fundamental reason being the fact that the fluid to tissue density ratio is close to unity. Although significant progresses have been achieved during the last years, solving the fully coupled problem often exhibits a prohibitive computational cost. They introduce a semi-implicit coupling scheme which remains stable for a reasonable range of the discretization parameters. The first idea consists in treating implicitly the added-masse effect, whereas the other contributions (geometrical non-linearity, viscous and convective effects) are treated explicitly. The second idea, relies on the fact that this kind of explicit-implicit splitting can be naturally performed using a Chorin-Temam projection scheme in the fluid. They prove (conditional) stability of the scheme for a fully discrete formulation. Several numerical experiments point out the efficiency of this scheme compared to several implicit approaches.
• In The Netherlands, de Putter et al [6], at the faculty of Biomedical Engineering
(Technische Universiteit Eindhoven) developed an approach to compute the wall
Consortium OCFIA
25/60
stress on the true diastolic geometry at a given pressure with a backward incremental method. The method has been evaluated with a neo-Hookean material law for several simple test problems. The results show that the method can predict an unloaded configuration if the loaded geometry and the load applied are known. The effect of incorporating the initial diastolic stress has been assessed by using three patient-specific geometries acquired with cardiac triggered MR. The comparison shows that the commonly used approach leads to an unrealistically smooth systolic geometry and therefore provides an underestimation for the peak wall stress. Their backward incremental modelling approach overcomes these issues and provides a more plausible estimate for the systolic aneurysm volume and a significantly different estimate for the peak wall stress. When the approach is applied with a more complex material law which has been proposed specifically for abdominal aortic aneurysm similar effects are observed and the same conclusion can be drawn. A key ingredient for computational hemodynamics under in vivo geometrical conditions, even under the rigid wall assumption, is the surface reconstruction from medical images. The level set method [12] has recently been applied to the reconstruction of a bifurcation [13],[14] and has a number of advantages: a) it can handle complex topology without difficulty, b) it is rather insensitive to image noise and c) extends straightforwardly to time-series of images of moving vessels. Aspects a) and b) imply that the amount of manual intervention required is negligible.
Computational hemodynamics in particular and HPC in general is expected to boost the basic understanding and treatment capabilities with respect to at least these two following aspects:
• Stented arteries: To date, angioplasty is the first choice treatment for arterial stenosis and short occlusion in small arteries (700,000 stents per year in Western Europe, 1.5 million per year in the USA). Stenting is generally very successful; however in some 10% of cases the vessels narrow again (restenosis). The medical causes of restenosis are not well understood, but hemodynamics and effects of the altered wall compliance seem to be major factors. A number of simulations have been conducted which typically neglect the stent deformation [7]. Though stent design is crucial in creating mechanical phenomena that might lead to stent failure, little attention has been given to improve the stent design in order to minimize stent-induced disturbances on normal hemodynamics and wall mechanics.
• Atherosclerotic plaque: Obviously, for clinicians who look into mechanisms
responsible for the progression of the atherosclerotic plaque or the growth of an aneurysm, access to knowledge of the vessel wall mechanics under the altered morphological and flow conditions is important. While the mechanical response of healthy arteries under physiological conditions is well studied [8], studies on atherosclerotic vessels in general provide wall data, but not the mechanical properties of plaque and the underlying arterial wall [9]. The specific mechanism by which
Consortium OCFIA
26/60
plaques rupture remains unknown, but the flow, the geometry and the material properties play significant roles in all hypotheses. Studies so far mostly considered the behaviour of plaque under static pressure have been presented [10]. Very few investigations have considered the fully coupled interaction of fluid motion and vessel wall [7] [11].
• HPC applied to medical research : Today's medical research is strongly linked with
advances in parallel and high performance computing. Ambitious research programs such as NeuroSpin (Saclay, France) are feasible thanks to the support of the computational ressources of CEA (9968 processors, 63 TFlops, 7th in the top 500 supercomputers). Data storage, visualization and grid infrastructure are also key issues. The development of Virtual Vascular Surgery is encouraged by grid computing consortiums such as Crossgrid. There is no doubt that advances in computational ressources and infrastructure will benefit to the medical community. In return, more and more challenging applications will rise and stimulate research and development.
Partenaires / Partnership
I2MR, UMR 858 INSERM, Bâtiment L3, CHU Rangueil, Toulouse (Institut de médecine moléculaire de Rangueil - Equipe X - Athérosclérose et artériosclérose de Greffe) The team of Radiology Department of Rangueil Hospital comprises radiologists, interventional radiologists, residents and three PhD specialized in MRI sequence design and medical image processing. The department is also a research unit associated to the I2MR (institut de médicine moléculaire de Rangueil) directed by the French institute of national research in medicine (INSERM U858). Four professors will be involved in the OCFIA project. Their activity covers the whole spectrum of radiological sub-specialities with a particular interest for both diagnostic and therapeutic aspects of vascular diseases. All imaging systems are available (2 MRI, 2 MDCT scanners, 3D rotational angiography, Trans oesophageal echography, Intra Vascular Ultra Sonography...). These interventional radiologists are board-certified physicians and are specialize in minimally invasive, interventional radiology. The team was involved in the more recent international studies on thoracic stent grafts, in particular for aortic dissections and aneurysms. Recently, a comparative study [15] was made by Prof H. Rousseau et al (coordinator of the OCFIA project and scientific representative of the I2MR framework) in order to evaluate surgery and stent-graft repair of acute or sub acute traumatic aortic rupture. In stable rupture of the aorta, initial conservative treatment is safe and allows management of the major associated lesions. Stent grafting is a valuable therapeutic alternative to surgical repair, especially in patients considered high risk for conventional thoracotomy. During his PhD preparation work, R. Moreno used an in vitro model of the aorta, which consists on a transparent silicon tube mimicking the anatomy of the thoracic aorta and the supra-aortic
Consortium OCFIA
27/60
trunks. A ventricular assisted device was used to generate a pulsatile flow. This experimental setup permitted the first 4D MRI protocol design dedicated to in vitro CFD image based application (blood flow computation chain). The same protocol is now applied to volunteers and patients in order to extract realistic and patient specific boundary condition data set [16].
Four members of the permanent staff and one Engineer will be involved part time in this research project: 45% Prof. H. Rousseau (Cardiovascular imaging, Aortic disease [14, 15, 16, 22-24,
27-33], head of the radiology department, contact for OCFIA) 20% Prof. Philippe Otal ( Visceral & vascular imaging,
[15,22,24,25,27,29,30,32,33]) 20% Prof. Valérie Chabbert (Thoracic & Cardiovascular imaging, [24,25,27,32,33]) 10% Prof. Francis Joffre (Renal & Cardiovascular imaging, [24,25,30]) 90% The CDD position must be filled by R. Moreno (PhD) in this research project
(MRI sequence design, moving meshes, CFD applications [14,16,21,23]). I3M, Institut de Mathématiques et de Modélisation de Montpellier The institute is part of the Department of Mathematics of the University Montpellier II and is also a research unit associated to the French agency for scientific research (CNRS – UMR 5149). About 110 people are working in this laboratory (80 with a permanent position as a teacher/researcher, 30 PhD students). Its activity is well balanced between mathematical analysis and scientific computation with industrial or medical applications. Six professors at I3M perform their research in topics related to Computational Fluid Dynamics (flow control and optimization, fluid/structure interaction, Large Eddy Simulations of turbulent flows, high order numerical methods for unstructured meshes, physical and numerical modeling of unsteady boundary conditions) or medical imaging (3D reconstruction for Tomography TEP, in collaboration with CHU Montpellier and Siemens Medical Systems - ongoing thesis under CIFRE funding). I3M has a strong implication in biomechanical research with former or ongoing collaborations with the faculty of medicine of Nîmes (effects of stenting), CHU Montpellier (effects of moving arterial domain), INRIA (3D reconstruction from CT images), the Center for Turbulence Research of Stanford University (stenting effects), LIRMM (3D reconstruction for TEP), General Electric and Siemens (inverse problems for medical imaging, image segmentation). Prof. F. Nicoud, the scientific representative of I3M in the framework of this research project, has strong connection CHU Toulouse and is working in collaboration with Prof. H. Rousseau (the OCFIA coordinator) since 2001. He is the co-advisor of R. Moreno who used the AVBP code during his PhD thesis to compute several blood flows under physiological conditions. The concept of using 4D IRM sequences to generate time varying finite element meshes [16] and perform moving boundaries hemodynamic simulations was initiated and developed during this PhD study, after a preliminary study performed at I3M and dealing with the effects of arterial stenting on the blood flow characteristics [17]. Before he took his position at University Montpellier II, F. Nicoud worked as a senior scientist at CERFACS for several years. As such, he has been a key contributor to the development
Consortium OCFIA
28/60
of the CERFACS code AVBP which will be used during this research project. He noticeably developed integral characteristic based boundary conditions which are well suited for cardiovascular applications where precise data are most of the time missing [18]. He is also an active member of the Société de Biomécanique and is a member of the management committee of the GDR 2760 « Biomécanique des Fluides et des Transferts – Interaction fluide / structure biologique » dirigé par V. Deplano (CNRS IRPHE)
Three professors and one CNRS research engineer from I3M will be partly involved in this project: 42 % F. Nicoud (numerical methods, boundary conditions [14,16-18,21]), 20 % B. Koobus (fluid-structure interaction, moving meshes [36-38]), 15 % J.F. Crouzet (inverse problem, 3D reconstruction, [39-41]), 15 % P. Redont (homogeneisation techniques (rheology), computing support [42-
44]), ASA - Adavanced Solutions Accelerator is a Small and Medium Business company launched early 2006 addressing two main Information Technology (IT) segments i.e. Deep Computing (including High Performance Computing) and Bioinformatics. Vision statement is clearly spelled as being THE academic and private research scientific computing partner of any leading edge project gated by IT. To that extent, a major alliance has been from day one established with IBM, as a leading worldwide IT player with top ranking in High Performance Computing (HPC) systems and as well as market share. In parallel, ASA has already started several joint efforts with CNRS - IGH "Institut de Génétique Humaine" on Genomics, Limoges Hospital and University as well as CEA-DSV "Direction des Sciences du Vivant" on Proteomics, and has help CNRS-Hydrosciences to architect, implement and administrate an IT cluster. More over key services provided, either as a fee, or within a joint project with academic bodies, include tuning, optimization and parallelisation of a given application package, when deemed necessary to enable a research breakthrough. On demand computing is also a free service from ASA Portfolio. ASA staff comprises today 5 key skills from 3 citizenships, of which three own Biology or Neurosciences Masters as well as Information technology complementary degrees. Such project at the conjunction of CFD and Life Sciences is clearly at the heart of ASA corporate strategy. More over, with well established links with IBM corporation, ASA achieved to get informal agreement from IBM to get access, as it does exist today for software vendors application evaluations, to major IT architectures such as Blue Gene or other large internal clusters.
Fred Viart (50%), CEO and founder ASA, is a former IBM upline manager, in charge from 1997 til 2005 of the IBM European benchmark center. This center staffed with more than 100 Engineers from all over the world was in charge of helping european and asia pacific customers to architect, optimize performance for ther home grown or
Consortium OCFIA
29/60
any given packaged applications. Such a center was, and still is equiped with more than 20 Tflops of various kind of processor types and architecture, including Grid computing, Blue Gene, and some of the technolgy that runs in top european supercomputer MareNostrum in Barcelona. Vincent Bosquier (50%), ASA Technical Director, was before joining ASA, in charge of setting up and optimizing a 38 nodes cluster for a french Biotech Company dealing mainly with protein virtual screening. Dr Ming Chau (90%) PhD from Toulouse University and graduated from ENSEEIHT engineering school is planned to be hired by ASA for the duration of this project and stay in the company to bring his broad range of knowledge in IT optimisation. He is skilled in Parallel Computing, Applied Mathematics and Code tuning and optimisation.
Due to the nature of both private and public research projects ran by ASA or ASA Team members in their previous jobs, technical publications written cannot be disclosed. As far Dr Chau is concerned here are his recent ones to be published shortly [19], [20].
Organisation et management du projet / Project organization and management
This project does include significant challenges as well as key deliverables. To that extent, management system for the project will be implemented as follows:
• A Management Board will be established with a deliverable focus, reviewing achievements and next coming milestones, resources plans, documentation issued or to be issued, budget, internal and external communication, major plan changes as well as risks identification and management. This management Board will meet thru calls or Visio conferencing every other month and will issue a meeting summary with project status, and decisions taken. It will be run as a face to face meeting alternatively in Toulouse and Montpellier every 6 months. Should more frequent meetings be needed, it's up to this board to decide when and how. Management Board will be led by Coordinator Prof. Hervé Rousseau (Toulouse, I2MR, INSERM U858, CHU of Rangueil) with attendance for all partners from their lead person (Montpellier I3M Franck Nicoud, ASA Frédéric Viart) as well as their scientific officer.
• A Scientific Board will be as well established to focus on key scientific challenges and
bottlenecks, with the main intent to uncover them before they arise and start gating the project schedule and call for all partners or beyond help to solve them.
Detailed technical achievements will be reviewed documented and be ready for Management Board approval. Most operating decisions will be handled by this scientific board, leaving resources issues only for decision by Management Board. This board will meet thru calls or Visio conferencing every two weeks and will issue a
Consortium OCFIA
30/60
meeting summary with project status including next short term steps, and decisions taken. Should a gating need for resource that can't be solved by a unique partner be identified during this scientific board, it can call for a management board to be held within two weeks. Scientific Board will be led by I3M representative Prof. Franck Nicoud with attendance of all partners’ involved technical teams.
Regardless of ANR documentation and reporting requirements that will be fulfilled as priority one by the project team, formal Project file updates will be issued every 6 months from T0 on for availability to partners and appropriate bodies. Thanks to the limited number of partners, the size of each team and the geographical position of Montpellier- Toulouse (2 hours drive) such a management system should overcome most issues and drive project efficiency. The issues raised at different level of the work-packages will be highlighted during workshops to be held for this purpose, at the given centre depending on the thematic and the staffs’ availabilities.
Structure du projet – Description des sous-projets / Structure of the project – Work-packages
Each individual partner of the network is an internationally recognised leading expert in his specific field. The particular areas of expertise are listed in § 5. However, no single partner possesses the full range of scientific skills to conduct the multi-disciplinary research of OCFIA. Hospital need the expertise of bioengineering group to advance with the understanding of flow physics and the application of simulations. Engineers need the expertise in the pathology and the input of case studies from the hospital. Both need the optimization skills of HPC experts in order to significantly reduce the restitution time of the data reduction steps and computations. In this project we propose a method to build patient-specific geometric data and boundary conditions, for unsteady CFD runs, with time varying meshes valid over the cardiac cycle. The structure of the project is illustrated through a block diagram containing the most important key words of the problem chain.
The starting point is a specific 4D MRI protocol, developed during R. Moreno’s CDD work at
I2MR and I3M in order to extract the full geometric data at several phases over the cardiac
cycle. Hemodynamic boundary conditions (velocity inlet and outlet) are acquired by means of
another sequence, a velocity-encoded MR imaging, into the same MRI device. . A noise
reduction strategy is then used together with a 3D Level Set method [12] to extract one
native blood flow domain and a mesh generator is used to generate the associated native
mesh.. The next step consist in computing a non-linear-transformation field [16] from 4D
vascular images (image warping). The physiological time variations of the arterial domain is
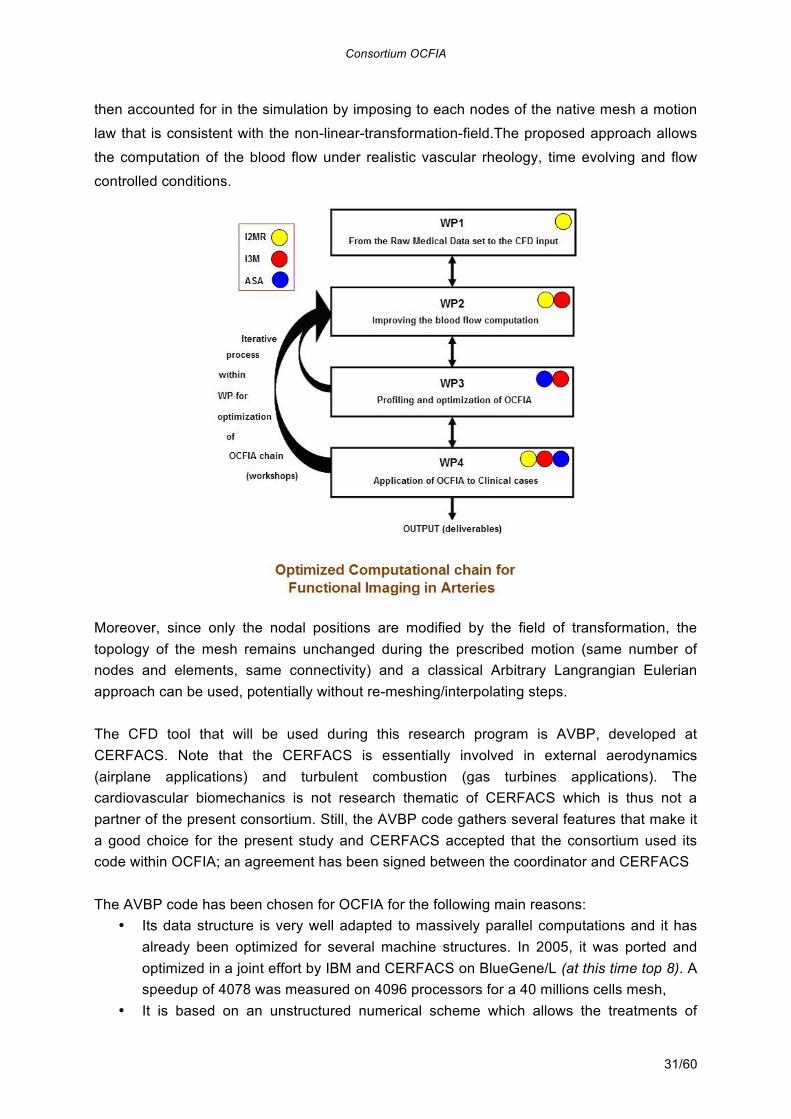
Consortium OCFIA
31/60
then accounted for in the simulation by imposing to each nodes of the native mesh a motion
law that is consistent with the non-linear-transformation-field.The proposed approach allows
the computation of the blood flow under realistic vascular rheology, time evolving and flow
controlled conditions.
Moreover, since only the nodal positions are modified by the field of transformation, the topology of the mesh remains unchanged during the prescribed motion (same number of nodes and elements, same connectivity) and a classical Arbitrary Langrangian Eulerian approach can be used, potentially without re-meshing/interpolating steps. The CFD tool that will be used during this research program is AVBP, developed at CERFACS. Note that the CERFACS is essentially involved in external aerodynamics (airplane applications) and turbulent combustion (gas turbines applications). The cardiovascular biomechanics is not research thematic of CERFACS which is thus not a partner of the present consortium. Still, the AVBP code gathers several features that make it a good choice for the present study and CERFACS accepted that the consortium used its code within OCFIA; an agreement has been signed between the coordinator and CERFACS The AVBP code has been chosen for OCFIA for the following main reasons:
• Its data structure is very well adapted to massively parallel computations and it has already been optimized for several machine structures. In 2005, it was ported and optimized in a joint effort by IBM and CERFACS on BlueGene/L (at this time top 8). A speedup of 4078 was measured on 4096 processors for a 40 millions cells mesh,
• It is based on an unstructured numerical scheme which allows the treatments of
Consortium OCFIA
32/60
arbitrarily complex geometries, such as those met in the cardiovascular system, • Since it is developed to perform unsteady simulations of turbulent flows, it uses both
low dissipative numerical schemes in order which minimize the artificial dissipation. The extension of these schemes to time varying meshes with simple geometric laws has been implemented,
• A whole family of characteristic-based boundary conditions has been implemented in order to minimize the artificial reflection near inlets and outlets. Noticeably, integral boundary conditions have been developed which allows the user to prescribe mean flow rate through the inlet section instead of the exact flow rate profile over this section. This feature is extremely useful for biomechanical applications where the current measurement techniques do not offer enough resolution to provide the blood flow repartition over an artery cross section,
• It is extensively validated with a whole set of academic test cases including several well suited to cardiovascular application such as the pulsed pipe flow,
• It has already been used several times for biomechanical applications, noticeably within the thesis of R. Moreno at CHU Toulouse, but also in the framework of several Master training periods in collaboration with INRIA Rocquencourt and IMF Toulouse,
Two people of the OCFIA program knows this code very well:
• the scientific representative of I3M, as a former developer of AVBP and also as an advisor of several PhD students using this tool,
• R. Moreno, who will be the post-doctorant hired by CHU for OCFIA, as an expert user of AVBP for biomechanical applications.
Thus, although AVBP is not dedicated to cardiovascular applications, it is one of the most mature CFD code worldwide for unsteady applications in complex geometries. It is definitely a very good candidate for the OCFIA program whose objective is not to develop a federative code for biomechanical applications but to demonstrate the feasibility of complex CFD analysis under the constraints imposed by the medical routine in CHU hospitals. Work-package 1 : “Medical data treatment” – Leader I2MR Until now, all image data sets were been acquired in the same MRI system. The advantage is twice. The boundary conditions setup is optimal because the temporal (ECG) and spatial references are the same for all data sets. The clinical application is easy because the patient undergoes all examinations into the same image protocol. Still, significant challenges must be addressed before raw data can be post-processed into CFD input routinely. This work package aims at improving the image filtering and segmentation, but also the mesh generation and transformation from one cardiac phase to the other.
• Geometry acquisition. The objective of this acquisition is to track the real wall motion of vascular structures over the cardiac cycle. Nowadays, a contrast-enhanced acquisition is used during clinical vascular studies. It is our start point and we use this
Consortium OCFIA
33/60
data set to extract and build the first numerical mesh of our proposed method. In order to animate the motion of this ‘native mesh’, we perform a cine scan (4D MRI) of the same volume of interest without contrast-enhance. Here, the most important parameter is the spatial deformation from the first static geometry to the other cardiac phases. A variety of scan methods are available for cine scans but there is a need to design an optimal sequence dedicated to wall displacements but also to extract the native geometry. Many advantages are required : full coverage of the cardiac cycle, intrinsic high signal-to-noise ratio, high signal of blood, short scan time, no breath hold and intrinsic flow compensation (limit artifacts). Cine scan have been applied in order to cover exactly the same field of view (FOV) of the usual contrast-enhanced acquisition. New isotropic voxel dimensions are next to (2x2x2 mm)x20 cardiac phases. Although this spatial resolution is not good for image visualization, it’s a good approximation to estimate the non linear transformation field necessary to build the moving meshes. In this project, we plan to develop cine scans to complete all geometry processing (native mesh & wall deformation) from a single 4D MRI sequence with 1x1x1x20c.ph resolution. This will put more pressure on the tools used to post-process the MRI images and generate the sequence of time varying meshes required by the CFD solver.
• Segmentation, 3D surface reconstruction & ‘native’ volume meshing: 3D image
reconstruction methods based on 3D level set methods (J.A. Sethian, 1999) will be developed as they have the potential to offer the robustness and ergonomic use required in clinical routine application. They also promise superior robustness to image noise which will be of importance as the image resolution will be pushed to its limits. Actually, the excessively fine meshes from the 3D method will be coarsened using mesh-decimation techniques to be suitable for CFD.
• Moving meshes via Non-linear transformation field: Transforming one image
volume to another involves estimating a spatial vector field (deformation field) that maps from coordinates of one volume to those of the other (image warping). In this work, the source volume will be considered as fixed (corresponding to the native mesh), and a mapping from this volume to the template volume will be estimated. A high dimensional approach will be used, whereby a finite element method is employed to estimate translations at the location of each voxel in the template image. Bayesian statistics will be used to obtain a maximum a posteriori (MAP) estimate of the deformation field. The fundamental assumption is that the probability of stretching a voxel by a factor of n is considered to be the same as the probability of shrinking n voxels by a factor of 1/n. The penalty function of choice is based upon the logs of the singular values of the Jacobian matrices having normal distributions, which enforces a continuous one-to-one mapping.
Preliminary tests performed with a prototype implementation of the method showed that a parametric study is necessary to better understand the effects of the
Consortium OCFIA
34/60
numerical/statistical/regularisation parameters involved. It is also necessary to produce sufficient know-how to better understand the algorithm convergence: for example, it seems that early iterations, with a high regularisation parameter are necessary to find the low frequency warping (large movements) and obtain a smooth transformation field and that subsequent iterations, with less regularization are necessary to come to fine warping (details). A strong assumption made so far [16] is that the blood velocity at solid boundaries is equal to the nodal velocity as given by the transformation field. In other words, one assumes that the transformation field represents the motion of material points of the arterial wall. A specific action will be taken within the “Blood flow simulation” work package regarding this issue. From a medical imaging point of view, a specific MRI tagged sequence will be designed in order to assess the velocity of the arterial tissue, for comparison with the transformation velocity and assessment of the systematic error associated with this assumption.
Work-package 2: “Blood flow computations” – Leader I3M This work package aims at improving the description of the blood response to large geometrical changes over the cardiac cycle. This means improving the numerical algorithm to reach better accuracy and robustness of the results, and also improving the physical model which is solved numerically in order to include more complex effects of importance for the blood flow description. These two aspects are connected since any modifying the physical model may impact the behavior of the numerical procedure. Note that most of the work perform within WP2 will be part of the PhD thesis directed by Prof Franck Nicoud at the I3M. The detailed thesis subject including environments details is provided as an annex at the end of this file. The following ways of improvements of the flow computations will be investigated within this Work Package:
• Boundary conditions: Unsteady inlet/outlet boundary conditions will be developed that provide the inlet and outlet pulsating flow data and the corresponding arterial motion. Such boundary conditions should be able to reproduce the time delay and amplitude attenuation produced by the part of the arterial tree that is not computed by the 3D solver. One difficulty is the fact that the boundary impedance depends on the time frequency of the perturbations leaving the computational domain. This means that the boundary conditions must contain an on-line determination of the frequency components of the boundary variables. Note that this problematic is also shared by the combustion instability community where the phase lag at boundaries is one of the key parameter in the stability analysis. This common interest with the CFD team of CERFACS will boost scientific exchanges and cooperation between the OCFIA partners and the AVBP developers,
Consortium OCFIA
35/60
Another issue that will be investigated is the effect of the blood flow boundary condition at solid boundaries on the overall results and biomechanical functions. This is related to the assumption made so far that the transformation field used to generate the sequence of time varying meshes from the native mesh is also relevant to the displacement of material points of the arterial tissue. Under this assumption, the blood velocity at solid boundaries is equal to the velocity of the boundary nodes during the cardiac cycle. This is obviously wrong if one considers an artery submitted to a block rotation around its axis for which the transformation field would be zero, but not the boundary velocity. Thus several assumptions will be formulated regarding the arterial boundary condition (e.g. the blood velocity is induced by the wall normal motion of the artery) in order to investigate its effects on the overall blood flow solution. Note that qualitative data will be obtained within the “Medical data treatment” work-package in order to assess the systematic error related to the different assumptions that can be made.
• Multi-scale algorithm: As an alternative to the advanced boundary conditions
described above, the 3-D domain computed with AVBP can be coupled with a simplified 1D "hydraulic" model and 0D lumped model. The resulting hybrid, multi-scale description will allow accounting for the patient specific, distal properties of the arterial tree on the region of interest that is computed by resolving the equations for the blood motion. This will also allow assessing the sensitivity of the simulations to the variability in the medical data and the robustness of the subsequent conclusions that can be drawn in terms of diagnostics or therapeutic decision. The 1D hydraulic code will be provided by I3M. From a numerical point of view, coupling the 3D domain with variable geometry and a 1-D hydraulic model arising both practical (is it necessary/useful to couple the 3D and 1-D codes or should the hydraulic code be considered as a subroutine of AVBP ?) and fundamental issues (which variables should be exchanged ?, how avoiding artifact reflection at the interface ?),
• Handling low Mach numbers: The Mach number in blood flows is of order 10-3, far
below the region where solvers based on the compressible Navier-Stokes equations are efficient. So far, the blood flow simulations performed with AVBP were assuming an equivalent fluid with appropriate density and viscosity but very small speed of sound so that the effective Mach number (M) was close to 0.1 and the numerical issues related to the limiting case where M is close to zero could be avoided. This way of proceeding may be understood as a very crude preconditioned method for the compressible Navier-Stokes equations. Since many preconditioned methods have been proposed in the open literature, a comprehensive study will be performed in order to select the most appropriate for biomedical applications.
• Handling variable geometries: The Arbitrary Lagrangian Eulerian (ALE) approach
will first be used since it is already implemented in AVBP. Recall that in OCFIA, a
Consortium OCFIA
36/60
specific MRI sequence will be used to generate time resolved medical images. Segmentation, 3D reconstruction and mesh generation algorithms are first applied to a set of images corresponding to a reference phase in order to create a native mesh. Non-linear transformations are then applied to this native mesh in order to generate the meshes corresponding to the different phases which represent the cardiac cycle. Preliminary tests have demonstrated the potential of this approach to reproduce the blood response to small (carotid bifurcation) to moderate (aorta) geometrical changes. One can expect difficulties in the cases where the geometrical changes are large because the connectivity of the mesh is kept constant during the non-linear transformation process. Moreover, the ALE technique will break down in cases where the vessel topology changes; this could happen in severe aorta dissection for example. Thus, it is plan to investigate the potential of an Immersed Boundary Method to handle cases which could not be treated by ALE.
• Blood rheology: Almost all the cardiovascular simulations presented in the literature
assume a Newtonian behavior for the blood. This assumption is not justified under two peculiar circumstances: the diameter of the computed vessels is not large enough to assume large shear rate and neglect rolls formations; the time of residence in the flow domain is not negligible compared to the sedimentation time. Both of these situations are expected to occur in OCFIA. Indeed, the small arteries connected to the superior aorta must be accounted for in the computation if the distal flow rate is to be computed accurately. Besides, aorta dissection or aneurysms are characterized by region where the blood flow velocity is virtually zero and the residence time is very large. Two rheological models will be implemented in the AVBP code in order to reach a better description of the blood flow. The first one will be a Casson type of model, relating the viscosity to the local shear rate, and accounting for the yield stress. The second model will account for the thixotropic behavior of the blood caused by erythrocyte aggregation. To this end, a transport equation for the time of residence will be added in AVBP. The effect of changing the rheology of the fluid on the stability of the (preconditioned) numerical schemes will be analyzed and modifications will be proposed if required.
It is important to note that all the numerical and physical developments described above may change the profiling the code and the way it should or can be optimized for the different architectures that will be used during OCFIA. As a consequence, the “Blood flow computations” and “Profiling and optimization of the OCFIA chain” work-packages led by I3M and ASA will be strongly inter-connected.
Work-package 3: “profiling and optimization of OCFIA” – Leader ASA
• Parallel Image post-processing Today, the whole image post-processing takes 12 hours on a personal computer, in the Matlab environment. As a better spatial resolution is expected in future works, the current
Consortium OCFIA
37/60
materiel configuration will not be able to run post-processing. The porting of some scripts that are currently used, to Fortran parallel programs, will be performed each time it is necessary. Focus is put on the computation of native meshes and wall deformations:
1. A survey of existing implementations of the algorithms. The following points will be examined: numerical adequacy, licence agreement, portability.
2. Remaining implementation work to complete the whole application. 3. Tests and code optimizations dedicated to the actually used architectures.
• Profiling and optimization in CFD :
All the research and development work on the modelling of blood flow have significant impact on the usage of AVBP. Profiling and analysis will be performed besides the numerical simulations. The aim is to ensure that the CFD software remains exploited in optimal conditions:
1. Analysis of the user code inside the AVBP templates. 2. Enabling profiling and debugging facilities. 3. Checking of the execution reports.
Besides, a survey on potentially faster numerical algorithms will be performed, in order to optimize numerical algorithms as changes in models are performed in former work packages. These directions can be explored:
4. Optimization of domain decomposition in AVBP regard to overlapping and transmission conditions between subdomains
5. Choice of preconditionning techniques, improvements on the solution of algebraic systems. These optimizations should be adapted to the the physical problem solved. The need of load balancing will also be examined. The required software development, profiling and optimization will be performed, on all the targeted architectures.
• Identifying appropriate High Performance Architecture.
Several architecture elements need to be assess thru in depth technical analysis for the series of codes listed above that need to be tuned. Processors: currently available processors from various vendors include:
1. Intel and Intel chip sets based with frequency ranging from less than 2.0 ghz to 3.6 Ghz. Increased frequency impact on elapse time for runs wil be assesed. On the other hand, testing 2H2006 technologies such as dual core (Woodcrest) with common L2 cache as well as just released quadricore (Clovertown and next Tigerton MP) using a double dual core architecture with L2 + L3 cache to the expenses of clock frequency, need as well to be evaluated.
2. AMD Opteron, long lasting as a better performing processor for most scientific workloads, will need as well to be evaluated. Current 2218 dual core 2.8 Ghz as well
Consortium OCFIA
38/60
as Opteron Revision F next coming are the ones to egt codes tested on. Typical to this processor, Path scale Compiler, usually brings significant performance improvements compared to other generally available compilers, but this need to be as well tested.
3. Power PC is leading, performance wise on most applications requiring high memory bandwith. More over very large clusters (beyond 512 nodes) tend to use this architecture, such as Mare Nostrum Barcelona super computer, both for performance and environnemental considerations (power / cooling). Power PC is therefore as well a serious candidate for evaluation. As another member of the Power family, the Blue Gene Power PC implementation, running at very low frequency but implemented on architecture allowing scaling up to 64000 processors. ADVP been already proven to scale above 5000 processors testing this type of architecture is also required. More over, next generation of Blue Gene Power PC to be released end 2007 well within the first stage of this project, performance delta brought by this new technology need to be measured.
4. POWER6 from IBM, with a 2H2007 availability bringing an increased clock frequency up to 4.5 GHz as well as key features inheritated from the Power architecture such as multiple parallel execution elements, Branch history table… will as well be tested for performance validation.
5. CELL Broadband Engine, from Sony, Toshiba and IBM, this is a customized processor including a nanocore (one master core and 8 slaves). This Cell Broadband Engine was designed for image processing, and as such is currenly implemented in Game devices such as Play station and others. A dual Cell BE server already exists in Blade packaging for high density clusters and is in used for High Performance Computing in selected area, including some life sciences applications. Ability of this type of processor, though requiring code changes, but running Linux Fedora, to perform for post processing, need to be checked. Parallelization of image processing and code optimization will require special attention and care on the later architecture as hybrid memory model applies. The IBM XL optimized compiler uses the OpenMP programming model to support parallel programming across the PPE and multiple SPEs. On other architectures, effectiveness are expected with MPI parallelization or compilers facilities. Further optimisation with hybrid MPI+OpenMP model can be done if required.
Memory:
1. Memory architecture : Most current implementations rely on DDR2 memory architecture and as such if a cost effective solution need to be invested for routine runs in an hospital, it will most likely be the one chosen. However, FBDIMM could improve significantly memory subsystem performance. In fact, existing DDR2 memory employs multidrop parallel bus. This means electrical loadings increase as DIMMs are added to the bus and therefore it does limit speed of the memory bus. While FBDIMM solves problem by placing an Advanced Memory Buffer on DDR2 DIMM and employs a serial memory bus. Serial buses greatly reduce wiring
Consortium OCFIA
39/60
requirements and enable greater memory buses supported in a system, thus increasing capacity and throughput.
2. Memory size : Pending on architecture type (scale in or scale out, see below)
available memory sizes are different. Up to 16 GB per node as of today on most scale out implementation and up to 1 TB for scale in Large SMP servers. Applications usage of memory as well as data in memory affinity to local processor when a parallel solution is implemented need to be characterized for appropriate trade off.
Scale in - Scale Out architecture
With the exception of PowerPC solely implemented on scale out architectures, Intel, AMD and POWER6 are also provided by server manufacturer as Large SMP (up to 64 Way for POWER6). It's therefore required that for both image post processing and CFD, scale in up to a 64 way as well as Scale out up to 1024 nodes be evaluated. Interconnect Network Moving to Scale out architecture requires as well for any of the two processing, or for both, to assess newly coming interconnect network architectures. Current Gigabit Ethernet, 10Gb, Infiniband 4X, Myrinet, Quadrics, deliver totally different performances either on overall bandwith or latency values. Other network considerations (at processor level), such as TOE (TCP/IP Offload) IOAT (Intel I/O acceleration Technology) are to be assessed. Current data available from server laboratories on scalability demonstrate TOE maturity and IOAT as an early stage only, but overall compelling gains in throughput ranging from 30 to 60% versus NIC Overall. As project progress and more technological improvements are brought to the HPC community by Processor and Server manufacturer, some parts of this work will need to be performed again. As such evolution will never stops, two major milestones during the project, linked to architecture and optimized code deliverables will force two times a checkpoint with documenting optimum configurations.
• Dedicated cluster
Current numerical experiments do not exceed 24 hours, due to their sizes and moreover, fit inside average amount of memory - lesser than 1 GB. As the AVBP library already benefits from former optimization, parallel simulation of blood flow would be immediately efficient if a very high bandwidth network is available between the nodes of the cluster. Scalability is ensured as long as the size of the problem is large enough - this should not be a problem. Besides, this device will shorten the development and validation process of the parallel implementation of image processing algorithms. It will also allow the research team to launch many simulations in order to validate changes on models. If parallelization of image processing is done, 2 runs per day would be reachable with the current sizes of data. As

Consortium OCFIA
40/60
more precision is expected in future simulations, the cluster will be available to perform more CPU consuming runs. These developments will have positive impacts on the designing of a medical application and the specification of dedicated computational resources. Work-package 4: “Application of OCFIA to clinical cases” – Leader I2MR (Clinical applications) Currently, the large majority of pathologies of the descending aorta are treated by thoracic Stent-graft, a kind of endoprosthesis inserted via a femoral access which make it possible to exclude the lesion from blood flow. This technique presents many advantages compared to surgery because they avoid thoracotomy and aortic clampage, sources of cardiac, neurological and pleural complications, as well as medullary ischaemia. Obviously these results are confirmed in literature, with paraplegia and death rate significantly inferior compared to surgery. If until now, only the lesions of the descending aorta were accessible to this type of treatment for anatomical reasons, the latest technological developments augur that a majority of the lesions of the aortic arch will soon be accessible to this type of treatment. But the acquired experience over these last years, show that these stent grafts are subjected to major mechanical constraints, which can involve deterioration of the material or modifications of the aortic wall with risks of ruptures or dissections. The understanding of these phenomena enabled us to modify empirically our technique of treatment. But actually, a mathematical evaluation should help us to modify the characteristics of these stent-grafts (according to their flexibility, resistance…) to avoid their deterioration over time and make them more reliable. The study that we propose should also enable us to analyse the rheological modifications and the parietal forces exerted by blood flow upstream and downstream from the stent-graft, source of local aortic trauma with a risk of rupture or thrombus formation. Finally, in the context of dissections, related to a parietal breach making it possible for the blood flow to infiltrate in the arterial wall, the physiopathology is much more complex, and the mathematical evaluation should provide a better understanding of the lesions and will help the therapeutic decisions. Indeed, different type of treatments, surgical or endovascular can be considered, the choice residing on the analysis of the lesions, but also on hemodynamic concepts, difficult to obtain with noninvasive examinations. The objective of our workpackage would be to provide this hemodynamic and rheological information in three different configurations by a functional non-invasive examination and thus, propose the best therapeutic choice according to each clinical case.
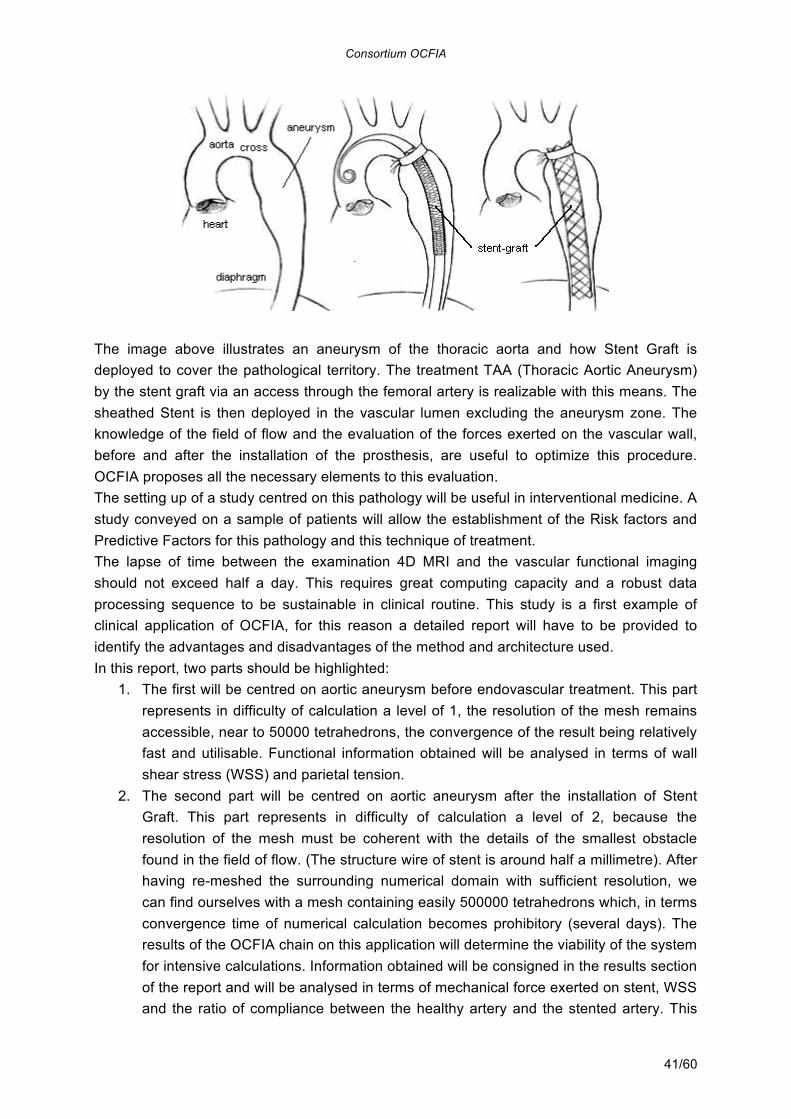
Consortium OCFIA
41/60
The image above illustrates an aneurysm of the thoracic aorta and how Stent Graft is deployed to cover the pathological territory. The treatment TAA (Thoracic Aortic Aneurysm) by the stent graft via an access through the femoral artery is realizable with this means. The sheathed Stent is then deployed in the vascular lumen excluding the aneurysm zone. The knowledge of the field of flow and the evaluation of the forces exerted on the vascular wall, before and after the installation of the prosthesis, are useful to optimize this procedure. OCFIA proposes all the necessary elements to this evaluation. The setting up of a study centred on this pathology will be useful in interventional medicine. A study conveyed on a sample of patients will allow the establishment of the Risk factors and Predictive Factors for this pathology and this technique of treatment. The lapse of time between the examination 4D MRI and the vascular functional imaging should not exceed half a day. This requires great computing capacity and a robust data processing sequence to be sustainable in clinical routine. This study is a first example of clinical application of OCFIA, for this reason a detailed report will have to be provided to identify the advantages and disadvantages of the method and architecture used. In this report, two parts should be highlighted:
1. The first will be centred on aortic aneurysm before endovascular treatment. This part represents in difficulty of calculation a level of 1, the resolution of the mesh remains accessible, near to 50000 tetrahedrons, the convergence of the result being relatively fast and utilisable. Functional information obtained will be analysed in terms of wall shear stress (WSS) and parietal tension.
2. The second part will be centred on aortic aneurysm after the installation of Stent Graft. This part represents in difficulty of calculation a level of 2, because the resolution of the mesh must be coherent with the details of the smallest obstacle found in the field of flow. (The structure wire of stent is around half a millimetre). After having re-meshed the surrounding numerical domain with sufficient resolution, we can find ourselves with a mesh containing easily 500000 tetrahedrons which, in terms convergence time of numerical calculation becomes prohibitory (several days). The results of the OCFIA chain on this application will determine the viability of the system for intensive calculations. Information obtained will be consigned in the results section of the report and will be analysed in terms of mechanical force exerted on stent, WSS and the ratio of compliance between the healthy artery and the stented artery. This
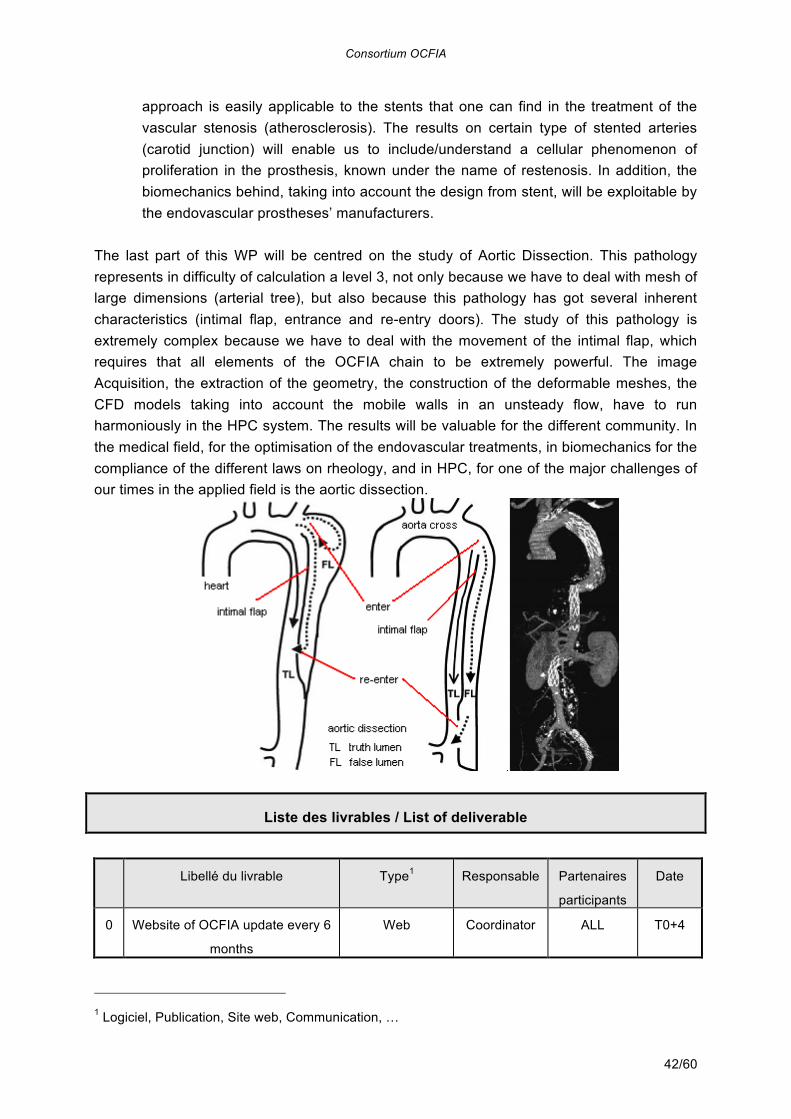
Consortium OCFIA
42/60
approach is easily applicable to the stents that one can find in the treatment of the vascular stenosis (atherosclerosis). The results on certain type of stented arteries (carotid junction) will enable us to include/understand a cellular phenomenon of proliferation in the prosthesis, known under the name of restenosis. In addition, the biomechanics behind, taking into account the design from stent, will be exploitable by the endovascular prostheses’ manufacturers.
The last part of this WP will be centred on the study of Aortic Dissection. This pathology represents in difficulty of calculation a level 3, not only because we have to deal with mesh of large dimensions (arterial tree), but also because this pathology has got several inherent characteristics (intimal flap, entrance and re-entry doors). The study of this pathology is extremely complex because we have to deal with the movement of the intimal flap, which requires that all elements of the OCFIA chain to be extremely powerful. The image Acquisition, the extraction of the geometry, the construction of the deformable meshes, the CFD models taking into account the mobile walls in an unsteady flow, have to run harmoniously in the HPC system. The results will be valuable for the different community. In the medical field, for the optimisation of the endovascular treatments, in biomechanics for the compliance of the different laws on rheology, and in HPC, for one of the major challenges of our times in the applied field is the aortic dissection.
Liste des livrables / List of deliverable
Libellé du livrable Type1 Responsable Partenaires
participants
Date
0 Website of OCFIA update every 6
months
Web Coordinator ALL T0+4
1 Logiciel, Publication, Site web, Communication, …
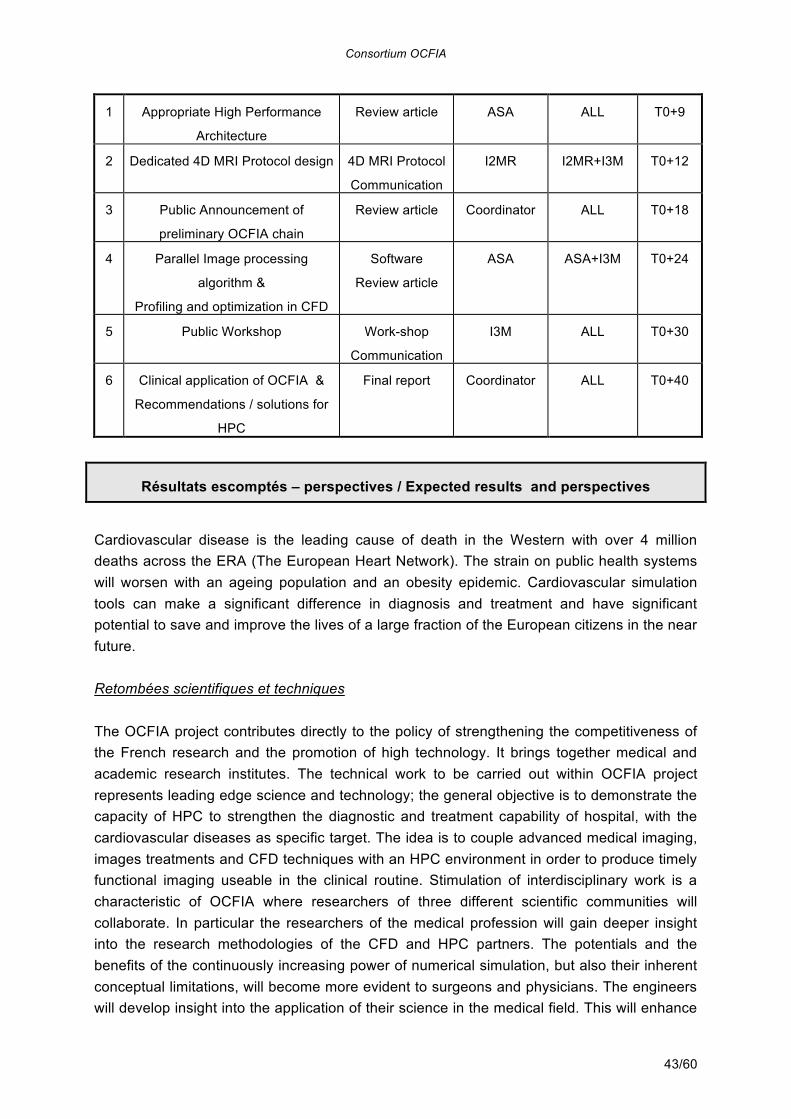
Consortium OCFIA
43/60
1 Appropriate High Performance
Architecture
Review article ASA ALL T0+9
2 Dedicated 4D MRI Protocol design 4D MRI Protocol
Communication
I2MR I2MR+I3M T0+12
3 Public Announcement of
preliminary OCFIA chain
Review article Coordinator ALL T0+18
4 Parallel Image processing
algorithm &
Profiling and optimization in CFD
Software
Review article
ASA ASA+I3M T0+24
5 Public Workshop Work-shop
Communication
I3M ALL T0+30
6 Clinical application of OCFIA &
Recommendations / solutions for
HPC
Final report Coordinator ALL T0+40
Résultats escomptés – perspectives / Expected results and perspectives
Cardiovascular disease is the leading cause of death in the Western with over 4 million deaths across the ERA (The European Heart Network). The strain on public health systems will worsen with an ageing population and an obesity epidemic. Cardiovascular simulation tools can make a significant difference in diagnosis and treatment and have significant potential to save and improve the lives of a large fraction of the European citizens in the near future. Retombées scientifiques et techniques
The OCFIA project contributes directly to the policy of strengthening the competitiveness of the French research and the promotion of high technology. It brings together medical and academic research institutes. The technical work to be carried out within OCFIA project represents leading edge science and technology; the general objective is to demonstrate the capacity of HPC to strengthen the diagnostic and treatment capability of hospital, with the cardiovascular diseases as specific target. The idea is to couple advanced medical imaging, images treatments and CFD techniques with an HPC environment in order to produce timely functional imaging useable in the clinical routine. Stimulation of interdisciplinary work is a characteristic of OCFIA where researchers of three different scientific communities will collaborate. In particular the researchers of the medical profession will gain deeper insight into the research methodologies of the CFD and HPC partners. The potentials and the benefits of the continuously increasing power of numerical simulation, but also their inherent conceptual limitations, will become more evident to surgeons and physicians. The engineers will develop insight into the application of their science in the medical field. This will enhance
Consortium OCFIA
44/60
their understanding of the application and the improved applicability of the research and the skills acquired by the researchers will ultimately prove extremely valuable to the bioengineering industry. Two objective measures of the success of the project will be available at the end of OCFIA:
• The interest and the implication of the medical community in the workshop “HPC and Medical routine” that will be organized during the course of the project in order to disseminate the information gained during its achievement. This scientific event is scheduled at T0+30 in order to have sufficient input from OCFIA and also to keep time for incorporating ideas/recommendations from the whole clinical community into the final report about the clinical applications of OCFIA,
• The final report at T0+40 about the clinical applications of the OCFIA chain. This report will detail how and to which extend the CFD based functional imaging has been useful to make a better therapeutic decision for one or more patient of CHU Rangueil. Behind the scientific/fundamental interest that the work scheduled within OCFIA deserves, the three consortium partners understand the breakthrough that would represent the actual application of computational functional imaging to a clinical case.
Hopefully, the project will make very good progress toward developing a cardiovascular simulation chain, between image data set acquisitions to the functional result, with the ambitious objective to demonstrate the potential of such a chain in the clinical environment. This tool will alter the way physicians diagnose and treat cardiovascular disease in the future. Europe has excellent research in the fields of engineering science and cardiovascular medicine. However, it has fallen behind the USA in integrating these disciplines and bringing the advance in simulation techniques to clinical practice. This project aims at reducing this gap. OCFIA will result in an improvement of the medical and engineer workgroup relationship, a mandatory to resolve the complicated fluid to vessel wall interaction problem. A new generation of biomedical researchers needs to be trained in advanced engineering methods as well as in the medical applications to particular pathologies. This project provides training and transfer of knowledge in this area for a new generation of researchers (medical, numerical) that is needed to meet the challenges in health care. The training of 3 young researchers in the field of cardiovascular biomechanics is an important contribution for strengthening the research and development effort in France. The scientific progress made within OCFIA will be shared with the community thanks to the web site that will be open shortly after the project start and which will host all the deliverables and meeting minutes. Another efficient mean of dissemination will be the workshop that will be organized at T0+30 in order to promote the use of HPC tools in clinical environment. In this way, it is expected that the progress will benefit the largest part of the potential end users (cardiovascular radiology departments in hospitals). The technical/scientific progress will be made sustainable thanks to the interest that the major medical systems manufacturers (GE, Philips, Siemens) should show for the HPC-based functional imaging by incorporating this
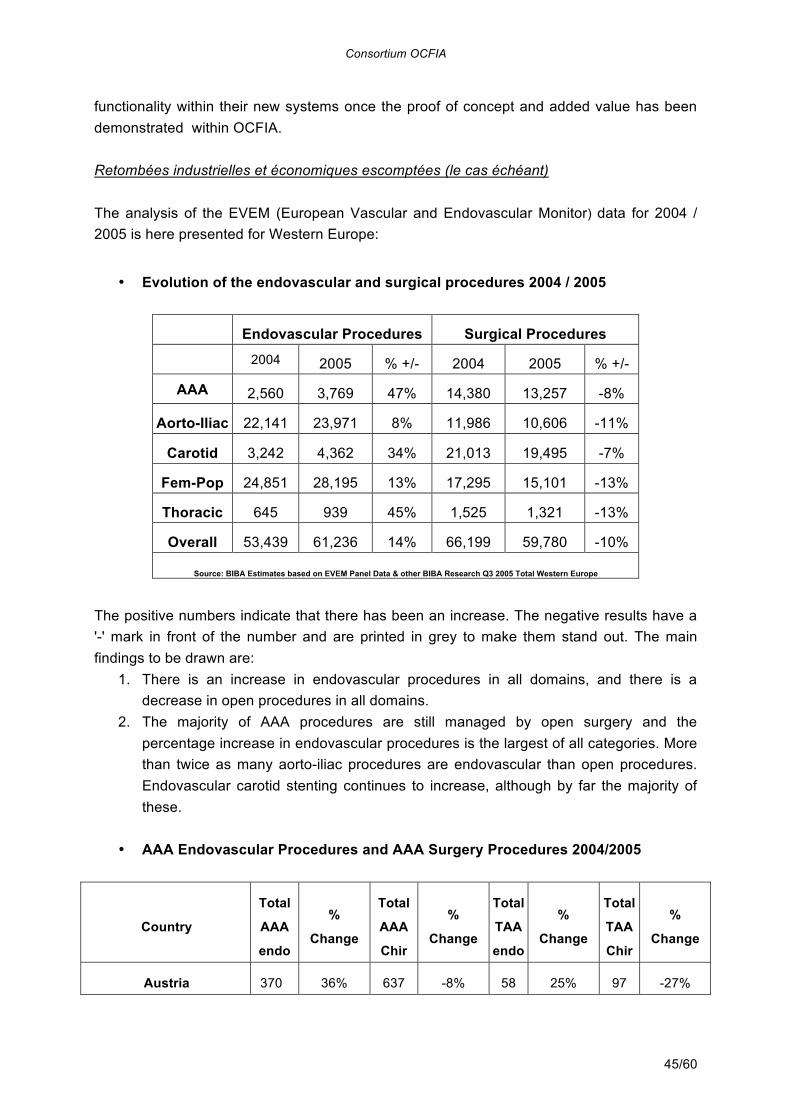
Consortium OCFIA
45/60
functionality within their new systems once the proof of concept and added value has been demonstrated within OCFIA. Retombées industrielles et économiques escomptées (le cas échéant)
The analysis of the EVEM (European Vascular and Endovascular Monitor) data for 2004 / 2005 is here presented for Western Europe:
• Evolution of the endovascular and surgical procedures 2004 / 2005
Endovascular Procedures Surgical Procedures
2004 2005 % +/- 2004 2005 % +/-
AAA 2,560 3,769 47% 14,380 13,257 -8%
Aorto-Iliac 22,141 23,971 8% 11,986 10,606 -11%
Carotid 3,242 4,362 34% 21,013 19,495 -7%
Fem-Pop 24,851 28,195 13% 17,295 15,101 -13%
Thoracic 645 939 45% 1,525 1,321 -13%
Overall 53,439 61,236 14% 66,199 59,780 -10%
Source: BIBA Estimates based on EVEM Panel Data & other BIBA Research Q3 2005 Total Western Europe The positive numbers indicate that there has been an increase. The negative results have a '-' mark in front of the number and are printed in grey to make them stand out. The main findings to be drawn are:
1. There is an increase in endovascular procedures in all domains, and there is a decrease in open procedures in all domains.
2. The majority of AAA procedures are still managed by open surgery and the percentage increase in endovascular procedures is the largest of all categories. More than twice as many aorto-iliac procedures are endovascular than open procedures. Endovascular carotid stenting continues to increase, although by far the majority of these.
• AAA Endovascular Procedures and AAA Surgery Procedures 2004/2005
Country
Total
AAA
endo
%
Change
Total
AAA
Chir
%
Change
Total
TAA
endo
%
Change
Total
TAA
Chir
%
Change
Austria 370 36% 637 -8% 58 25% 97 -27%
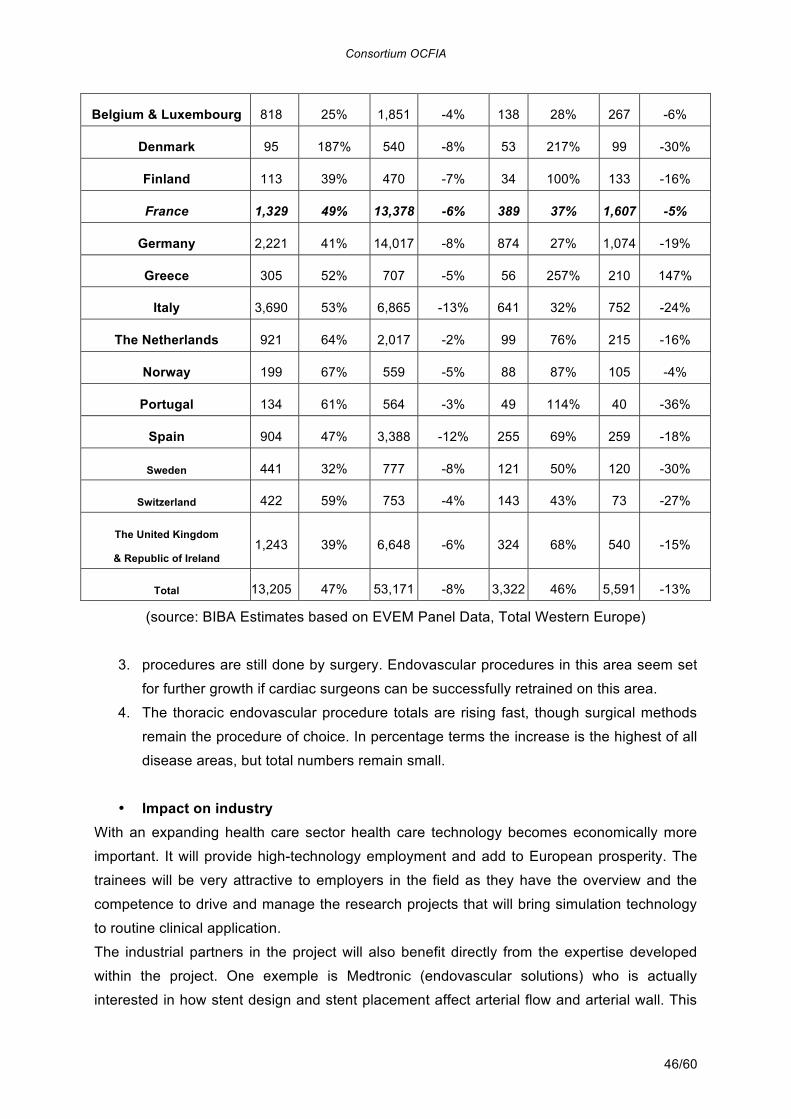
Consortium OCFIA
46/60
Belgium & Luxembourg 818 25% 1,851 -4% 138 28% 267 -6%
Denmark 95 187% 540 -8% 53 217% 99 -30%
Finland 113 39% 470 -7% 34 100% 133 -16%
France 1,329 49% 13,378 -6% 389 37% 1,607 -5%
Germany 2,221 41% 14,017 -8% 874 27% 1,074 -19%
Greece 305 52% 707 -5% 56 257% 210 147%
Italy 3,690 53% 6,865 -13% 641 32% 752 -24%
The Netherlands 921 64% 2,017 -2% 99 76% 215 -16%
Norway 199 67% 559 -5% 88 87% 105 -4%
Portugal 134 61% 564 -3% 49 114% 40 -36%
Spain 904 47% 3,388 -12% 255 69% 259 -18%
Sweden 441 32% 777 -8% 121 50% 120 -30%
Switzerland 422 59% 753 -4% 143 43% 73 -27%
The United Kingdom
& Republic of Ireland 1,243 39% 6,648 -6% 324 68% 540 -15%
Total 13,205 47% 53,171 -8% 3,322 46% 5,591 -13%
(source: BIBA Estimates based on EVEM Panel Data, Total Western Europe)
3. procedures are still done by surgery. Endovascular procedures in this area seem set
for further growth if cardiac surgeons can be successfully retrained on this area.
4. The thoracic endovascular procedure totals are rising fast, though surgical methods
remain the procedure of choice. In percentage terms the increase is the highest of all
disease areas, but total numbers remain small.
• Impact on industry
With an expanding health care sector health care technology becomes economically more
important. It will provide high-technology employment and add to European prosperity. The
trainees will be very attractive to employers in the field as they have the overview and the
competence to drive and manage the research projects that will bring simulation technology
to routine clinical application.
The industrial partners in the project will also benefit directly from the expertise developed
within the project. One exemple is Medtronic (endovascular solutions) who is actually
interested in how stent design and stent placement affect arterial flow and arterial wall. This
Consortium OCFIA
47/60
will be valuable information to be incorporated on the stent design process.
• Business development, workforce and market impact. With a fully validated imaging and computing solution, thanks to the final output of this
project, several business developments will be triggered.
On the academic side, re-gained leadership in this field will enable additional projects and
research fields wherever both CFD and medical imaging needs to be bundled to deliver new
hospital tools.
Regardless of the highly skilled workforce required to staff those additional projects (PhD,
research engineer…) in public research, the full solution implementation will yield a
significant value added for any private company able to run such a business.
Solution itself, including IT hardware, software tools, services to integrate it with imaging
equipments, as well as skill transfer workshops can easily be valued at 100 K€ per
implementation. With 65 , european only, hospitals as a preliminary market, a 6,5 M€
revenue can be sized.
With a need to permanently keep the solution up to date as both softwares, hardwares and
medical imaging equipments performances increase, this represents a long term activity
worth 20-30 people in a company running it.
No need to say ASA, primary private partner for this project, is ready to invest in any market
analysis, additional solution packaging and marketing budget required to capture this
business. First within France selected hospitals and then abroad.
Propriété intellectuelle / Intellectual property
• Agreement between partners: An agreement between partners will be signed at the
time of the initial phase of the project to define the important points necessary for best possible management (financial conditions, IPR Intellectual Property Right, work plan,…). The agreement between partners will identify the experience of each partner to reach the objectives of the project. The list corresponding of patents at the disposal of the partners for the duration of the project will be included. Produced knowledge will belong to the partner who generated them; thus partner is the first person in charge in protection of results.
• Management of the intellectual rights of ownership: Subject to the rights of the State taking into account its participation in the financing of work and the possible rights of a third, the Partners are agree with what follows : 1. Each Partner will preserve the property of its original knowledge acquired or
developed before the entry into force of Convention, or independently of the execution of this one. The Partner holding knowledge agrees to concede to another Partner of Convention, with its request, a right of free use, nonexclusive
Consortium OCFIA
48/60
and non-transferable, known as former knowledge, necessary to the other Partner to complete its own work with the title of Convention.
2. Each Partner will be sole owner of new knowledge, which it will have acquired only within the framework of Convention. If, for the needs of work under the title of Convention, a Partner needed to reach new knowledge of another Partner, the latter will concede a right of use to him, free, nonexclusive and non-transferable, as new knowledge for the only ends to the execution of Convention.
3. New knowledge obtained jointly and likely to be patented will make, except contrary agreement of the Partners, the object of a deposit of patent application in joint ownership. The rights of the Partners will be based on their respective contributions to these patentable results, each one having a right free, nonexclusive, inalienable and intransmissible of exploitation of these results. For new knowledge obtained jointly and not patented or not patentable, each Partner will profit from a nonexclusive, inalienable and intransmissible right free of analysis of the results.
• Classified information: It is not required to provide classified information in the project.
• Publications: The Consortium agreement will also establish rules regarding publications through the network that promote dissemination. All publications will be submitted to all network partners at least 4 weeks before submission. If partners raise objections the Management Board will arbitrate.
• Software licence for avbp code: For scientific reasons detailed within this file (section 7), the CFD tool used within OCFIA will be the AVBP software. The AVBP library will be made available to the OCFIA partners under an agreement valid for a four-year period and which is reproduced below: The AVBP software is a research software dedicated to unsteady simulations of reacting flows. It is developed by CERFACS and IFP (Institut Français du Pétrole). The software AVBP is being provided to the LICENSEE (each OCFIA partner) by its owners CERFACS and IFP under the following licence:
1. Permission is hereby granted to use, copy, amend or otherwise alter this
software and its documentation for IN-HOUSE RESEARCH PURPOSES ONLY and without fee or royalty, provided that the LICENSEE agrees to comply with the following copyright notice and statements, including the disclaimer, and that the same appear on ALL copies of the software and documentation
2. This software is provided ‘as is’, and CREFACS make no representations or warranties, express or implied. By way of example, but not limitation, CERFACS and IFP make no representations or warranties of merchantability or fitness for any particular purpose or that the use of the licensed software or documentation will not infringe any third party patents, copyrights, trademarks or other rights. The licensee accepts responsibility for the use to which this software is put and indemnifies CERFACS and IFP against all and any costs,
Consortium OCFIA
49/60
claims, demands or liabilities consequent upon or arising out of the use of the software.
3. The names of CERFACS or IFP may NOT be used in advertising or publicity pertaining to the use of AVBP without authorisation of CERFACS and IFP.
4. Publications of results obtained with AVBP shall acknowledge the use of AVBP when appropriate.
5. Title to copyright in this software and any associated documentation shall at all times remain with CERFACS and IFP, and LICENSEE agrees to preserve same.
6. The LICENSEE agrees not to distribute source code or parts or derivatives thereof, nor compiled versions of these, without the written agreement of CERFACS and IFP. The LICENSEE agrees not to distribute any part of the AVBP documentation, user’s guide or associated web pages without the written agreement of CERFACS and IFP.
7. The LICENSEE accepts responsibility for the proper use of this software by its employees and guests and shall ensure that they are aware of the terms and conditions of this license.
8. This agreement is valid for a duration of four years.
Moyens financiers demandés / Financial resources
• I2MR: the required funds will be used primarily to finance a Engineer position (CDD)
during the project, A gross salary monthly of 3968 euros (47616 euros/an) was retained. The other stations (internal missions, services, small equipment) are lower than 5% of the required assistance (223 868 euros).
• I3M: the required financing corresponds to the wages of the doctorand which will be recruited specifically for OCFIA. A gross salary monthly of 3608 euros (43296 euros/an) was retained. The other stations (internal missions, services, small equipment) are lower than 5% of the required assistance (158 484 euros).
• ASA: ASA: the required financing corresponds to the fully charged (social and taxes included) salary of a PhD which will be recruited specifically for OCFIA. With a 2500 € monthly gross salary, fully charged one is planned at 3750 €. The other cost elements (internal missions, services, small equipment) are set below 5% of total required amount. Fixed costs estimated are in line with spreadsheet algorithm. Ratio used to get to requested funding (237541 €) is set as for a small company (TPE) in ANR guidelines at 60%.
• Need for a small size dedicated cluster: Project plan is highly dependant on the ability to quickly identify major algorithm and code optimizations (work package 1). There is also a need for identification of the most appropriate architecture to run as fast as possible within a given hardware investment budget. Current runs, with a magnitude well below what will be needed, are performed on existing CINES (Centre Informatique National de l’Enseignement Supérieur, Montpellier, France) facilities (up
Consortium OCFIA
50/60
to 32 processors 1.8 GHz single core), when queuing lines for job processing permits. This leads to a limited quantity of iterations per week on currently available hardware. More over, it's most likely that the targeted architecture, as defined as an output of the work package will not be the one invested at CINES or IDRIS (Institut du développement et des ressources en informatique scientifique), neither technology wise nor size wise. To that extent, a 40 K€ investment budget is planned (that would today allow a 12 nodes dual processor, quadricore configuration) for 24 by 7 runs to be implemented in Toulouse INSERM/CHU facility, close to MRI department. Such an investment would definitively prove the fact that overall data treatment can be run efficiently and timely prior to a given person surgical act. It could, close to project completion, even be used for urgent analysis of a given patient. Production like equipment (with the ultimate cluster size) being later on invested on hospital operating budgets i.e. not requested to ANR.
Experts / Experts
Suggestion d'expert pour l'évaluation2
Prénom Nom Courriel Affiliation
(labo/entreprise/..)
Domaine(s)
d'expertise
2 Si possible prévoir des experts étrangers.
Consortium OCFIA
51/60
REFERENCES [1] Caro, C., Fitz-Gerald, J., Schroter, R., 1969. Arterial wall shear and distribution of early atheroma in man. Nature 211 (223), 1159–1160. [2] Roberto Corti, MD, Lina Baldimon, PhD, Valentin Fuster, MD, PhD and Juan José Badimon, PhD, Endothelium, flow, and atherothrombosis, Assessing and Modifying the vulnerable atherosclerotic plaque, American Heart Association, ed Valentin Fuster, MD, PhD, 2002 [3] Hayden Huang, DSc and Richard T Lee, MD, Stress and Strain: biomechanical guides for imaging plaque stability [4] Aaron J. Hall, Edward F.G. Busse, Don J. McCarville, John J. Burgess, Aortic wall tension as a predictive factor for abdominal aortic aneurysm rupture: improving the selection of patients for abdominal aneurysm repair, An Vasc Surg, 2000,(14)2:152-157 [5] Steinmann, D: Image-Based Computational Fluid Dynamics Modelling in Realistic Arterial Geometries, J Biomed Eng, 30:483-437, 2002. [6] S. de Putter, B.J.B.M. Wolters, M.C.M. Rutten, M. Breeuwer F.A. Gerritsen, F.N. van de Vosse, Patient-specific initial wall stress in abdominal aortic aneurysms with a backward incremental method, Journal of Biomechanics, 2006 [7] Stuhne G, Steinmann D: Finite Element Modelling of the Hemodynamics of Stented Aneurysms, J Biomech Eng, 126:382-390, 2004 [8] Humphrey JD, Na S: Elastodynamics and Arterial Wall Stress, Ann Biomed Eng, 30-4:509 –523, 2002 [9] Holzapfel, GA et al: Anisotropic Material Properties of Tissue Components in Human Atherosclerotic Plaques, J Biomech Eng, 126:657-665, 2002 [10] Schulze-Bauer C et al: Assessment of plaque stability based on high-resolution magnetic resonance, Comp. Bioeng.: Current Trends and Appl., Imperial College Press, pp101-115. 2004 [11] Tang D et al, Effect of Surrounding Tissue on Vessel Fluid and Solid Mechanics, Ann Biomed Eng; 32:947-60, 2001 [12] Sethian JA: Level Set Methods and Fast Marching Methods, Cambridge University Press, 1999 [13] Antiga L et al: Geometric reconstruction for computational mesh generation of arterial bifurcations from CT angiography. Computerized medical imaging and graphics, 26:227-235, 2002. [14] Moreno R, Nicoud F, Veunac L, Rousseau H. Level set methods to build moving meshes for patient specific blood flow simulations. Computer Methods In Biomechanics And Biomedical Engineering, Supplement 1, 2006, Pages 201-202. [15] H. Rousseau, C. Dambrin, B. Marcheix, L. Richeux, M. Mazerolles, C. Cron, A. Watkinson, A. Mugniot, P. Soula, V. Chabbert, G. Canevet, D. Roux, P. Massabuau, G. Meites, T. Tran Van, P. Otal, Acute traumatic aortic rupture: A comparison of surgical and stent-graft repair, J Thorac Cardiovasc Surg 2005;129:1050-1055 [16] Moreno R, Nicoud F, Rousseau H, Non linear transformation field to build moving
Consortium OCFIA
52/60
meshes for patient specific blood flow simulations, European Conference on Computational Fluid Dynamics ECCOMAS CFD 2006 P. Wesseling, E. Oñate, J.Périaux (Eds) © TU Delft, The Netherlands, 2006. ISBN: 90-9020970-0 [17] Nicoud, F., H. Vernhet and M. Dauzat, A numerical assessment of wall shear stress changes after endovascular stenting, Journal of Biomechanics 38, No. 10, pp. 2019-2027, 2005 [18] Nicoud, F. and Schönfeld, T., Integral Boundary Conditions for Unsteady Biomedical CFD Applications. Int. J. Numerical Meth. In Fluids, 40(457-465), 2002 [19] M. Chau, P. Spitéri, H.C. Boisson, Parallel numerical simulation for the coupled problem of continuous flow electrophoresis, International Journal for Numerical Methods in Fluids [20] Ming Chau, D. El Baz, Ronan Guivarch, Pierre Spitéri. MPI implementation of parallel subdomain methods for linear and nonlinear convection-diffusion problems. Journal of Parallel and Distributed Computing, Elsevier, 2007 [21] F. Nicoud, H. Vernhet, A. Pérez, M. Dauzat, R. Moreno, Arterial Stenting : from hemodynamics and wall mechanics to restenosis – experimental, in vivo and theoretical approaches, §13, 141-150 ESVB 2005, New technologies in vascular biomaterials, Fundamentals about Stents, (ed). Nabil Chakfé, Bernard Durand, Jean-Georges Kretz. [22] Hervé Rousseau, Jean-Philippe Verhoye, Jean-François Heautot (Eds.), Thoracic aortic disease, SPRINGER, 2006 [23] L. Veunac, R.Moreno, S. Jeetoo, D. Gensanne, G. Herigault, T. Lemettre, D. Vincensini, H. Rousseau, Characterisation of Arteriosclerosis Plaque in Carotid Artery with MRI Quantitative Sequence, CIRSE, Daily news, 2005, 5. [24] P. Otal, T. Smayra , C. Bureau, JM. Peron, V. Chabbert, P. Chemla, F. Joffre, JP Vinel and H. Rousseau, Preliminary results of a new expanded Polytetrafluoroethylene-Covered Stent-Graft for Transjugular Intrahepatic Portosystemic Shunts, AJR Am J. Roentgenol, 178(1):141-7, 2002. [25] V. Chabbert, S. Doussau-Thuron, P. Otal, l. Bouchard, A. Didier, F. Joffre and H. Rousseau, Endovascular treatment of aberrant systemic arterial supply to normal basilar segments of the right lower lobe, Cardiovasc Intervent Radiol 25(3):212-5, 2002. [26] Surgical treatment of an aortic arch aneurysm without cardio-pulmonary bypass: endovascular stent-grafting after extra-anatomic bypass of supra-aortic vessels. DAMBRIN C, MARCHEIX B, HOLLINGTON L, ROUSSEAU H. Eur J Cardiothorac Surg. 2005 Jan;27(1):159-61. [27] Acute traumatic aortic rupture: a comparison of surgical or stent-graft repair H ROUSSEAU, C DAMBRIN, B MARCHEIX, L RICHEUX, M MAZEROLLES, C CRON, A WATKINSON, A MUGNIOT, P SOULA, V CHABBERT, G CANEVET, D ROUX, P MASSABUAU, G MEITES, T TRAN VAN,P. OTAL,. J Thorac Cardiovasc Surg. 2005 May;129(5):1050-5 [28] Third International Summit on Thoracic Aortic Endografting: lessons from long-term results of thoracic stent-graft repairs. MITCHELL RS, ISHIMARU S, CRIADO FJ, EHRLICH MP, IVANCEV K, LACHAT M, MALINA M, MAY J, OREND KH, ROUSSEAU H, WILLIAMS DM. J Endovasc Ther. 2005 Feb;12(1):89-97. [29] Stent-graft repair of thoracic aortic aneurysms. H ROUSSEAU,JP BOLDUC , C
Consortium OCFIA
53/60
DAMBRIN, B MARCHEIX, G CANEVET,P. OTAL,. Tech Vasc Interv Radiol. 2005 Mar;8(1):61-72 [30] Midterm results of aortic diameter outcomes after thoracic stent-graft implantation for aortic dissection: a multicenter study. GAXOTTE V, THONY F, ROUSSEAU H, LIONS C, OTAL P, WILLOTEAUX S, RODIERE M, NEGAIWI Z, JOFFRE F, BEREGI JP. J Endovasc Ther. 2006 Apr;13(2):127-38. [31] Results of endovascular repair of the thoracic aorta with the Talent Thoracic stent graft: the Talent Thoracic Retrospective Registry. FATTORI R, NIENABER CA, ROUSSEAU H, BEREGI JP, HEIJMEN R, GRABENWOGER M, PIQUET P, LOVATO L, DABBECH C, KISCHE S, GAXOTTE V, SCHEPENS M, EHRLICH M, BARTOLI JM; J Thorac Cardiovasc Surg. 2006 Aug;132(2):332-9. [32] Mid term results of endovascular treatment of atherosclerotic aneurysms of the descending thoracic aorta. B MARCHEIX, C DAMBRIN, J P BOLDUC, V CHABBERT, C ARNAUD, C CRON, A MUGNIOT, P SOULA, M BENNACEUR, P MASSABUAU, P OTAL, A CÉRÈNE, H ROUSSEAU J Thorac Cardiovasc Surg. 2006 Nov;132(5):1030-6. [33] Endovascular repair of traumatic rupture of the aortic isthmus: Midterm results. B MARCHEIX, C DAMBRIN, J P BOLDUC, C ARNAUD, L HOLLINGTON, C CRON, A MUGNIOT, P SOULA, M BENNACEUR, V CHABBERT, P OTAL, A CÉRÈNE AND H ROUSSEAU, J Thorac Cardiovasc Surg. 2006 Nov;132(5):1037-41. [34] M.A. Fernandez, J.-F. Gerbeau, and C. Grandmont. A projection semi-implicit scheme for the coupling of an elastic structure with an incompressible fluid. Technical report, INRIA RR-5700, 2005. To appear in Int. J. Num. Meth. Engng. [35] P. Causin, J.-F. Gerbeau, and F. Nobile. Added-mass effect in the design of partitioned algorithms for fluid-structure problems. Comp. Meth. Appl. Mech. Engng., 194(42-44), 2005. [36] B. Koobus, H. Tran, and C. Farhat, Computation of Unsteady Viscous Flows Around Moving Bodies Using the k-e Turbulence Model on Unstructured Dynamic Grids, Computer Methods in Applied Mechanics and Engineering, Vol. 190, pp. 1441-1466, 2000. [37] B. Koobus and C. Farhat, Second-Order Time-Accurate and Geometrically Conservative Implicit Schemes for Flow Computations on Unstructured Dynamic Meshes, Computer Methods in Applied Mechanics and Engineering, Vol. 170, pp. 103-130, 1999. [38] B. Koobus and C. Farhat, On the implicit time integration of semi-discrete viscous fluxes on unstructured dynamic meshes, International Journal for Numerical Methods in Fluids, Vol.29, 975-996, Issue 8, 1999. [39] F. Ben Bouallegue, J.-F. Crouzet , B. Mohammadi, C. Comtat, D. Mariano-Goulart, (2007), « Extended and Recursive Fourier Rebinning Algorithms for 3-D PET Data », IEEE Transactions on Medical Imaging, Accepté pour publication. [40] D. Mariano-Goulart, J.-F. Crouzet , (2005), « A new reconstruction method in the Fourier domain for 3D positron emission tomography », C.R. Physique 6, pp 133 - 137. [41] C. Caderas De Kerleau, J.-F. Crouzet , E. Ahronovitz, M. Rossi, D. Mariano-Goulart, (2004), « Automatic Generation of Noise-Free Time-Activity Curve with Gated Blood-Pool Emission Tomography Using Deformation of a Reference Curve », IEEE Transactions on Medical Imaging , Vol. 23, no. 4, pp. 485 – 491. [42] P. Redont, H. Attouch et J. Bolte, Optimizing properties of an inertial dynamical system
Consortium OCFIA
54/60
with Hessian-driven damping. Link with proximal methods, Proceedings of the 8th Workshop on Well-Posedness in Optimization and Related Topics, Control \& Cybernetics, vol. 31 (2002) no. 3, pp 643-657; [43] P. Redont, H. Attouch, J. Bolte, M. Teboulle) Singular Riemannian Barrier Methods and Gradient-Projection Dynamical Systems for Constrained Optimization, Optimization, vol. 53 (2004) no. 5-6, pp. 435-454. [44] P. Redont, B. Ivorra, B. Mohammadi, L. Dumas) Semi-Deterministic versus Genetic Algorithms for Global Optimization of Multichannel Optical Filters, International Journal of Computational Science and Engineering (IJCSE), édition spéciale sur "Computational Methods and Techniques for Nanoscale Technology Computer Aided Design", à paraître.
Consortium OCFIA
55/60
ANNEXE 2 – Connaissances Propres des Parties L’ Unité U858 de « l’Institut de Médecine Moléculaire de Rangueil (I2MR)» de l’INSERM dirigée par Monsieur Angelo Parini, et en particulier l’équipe 10 « athérosclérose et artériosclérose de greffe » dirigée par Mme Anne Salvayre, située au 1 avenue du Professeur Jean Poulhès, BP 84225, 31432 Toulouse a développé une expertise sous la responsabilité scientifique de M Hervé Rousseau et M. Ramiro Moreno dans les domaines de :
• L’imagerie médicale angiographique, protocoles d’imagerie (Imagerie par résonnance magnétique (IRM) ou scanner (CT) dynamique) pour la mécanique des fluides numérique (MFN).
• Le traitement des images biomédicales, méthode d’extraction des surfaces artérielles et méthode de déformation non linéaire en vue de générer des conditions réalistes pour les calculs par MFN et le calcul des contraintes de déformation sur les prothèses endo-vasculaires (Stent et Stents-Grafts utilisés en radiologie interventionnelle).
• La méthode ‘patient spécifique’ pour la MFN appliquée à l’écoulement du sang dans les artères.
L’ « Institut de mathématiques et modélisation de Montpellier» (I3M – CNRS - UMR 5149) est situé au 2, Place Bataillon, CC51, 34095 Montpellier et est dirigée par B. Mohammadi. Avec le concours scientifique de Franck Nicoud, l’institut a développé une expertise dans les domaines de :
• L’analyse et mathématiques appliquées • Calcul scientifique appliqué à la médecine et à l’industrie en relation à la MFN • Contrôle et optimisation des flux, des conditions limites, • interaction fluide / structure (FSI), modélisation physique et numérique des phénomènes
instationnaires et/ou pariétaux, La Société « Advanced Solutions Accelerator » (ASA), dont le siège social est situé 199 rue de l'Oppidum, 34170, CASTELNAU-LE-LEZ est représentée par son président et responsable du développement, Monsieur Frédéric VIART. La société a développé une expertise dans le domaine du :
• Calcul intensif incluant le calcul haute performance (HPC) • La bioinformatique • Le « tuning » et l’optimisation des codes de calcul pour le calcul parallèle.
Consortium OCFIA
56/60
ANNEXE 3 – Liste des représentants au Comité. I2MR : Prof Hervé Rousseau I3M : Prof. Franck Nicoud ASA: Mr. Frédéric Viart
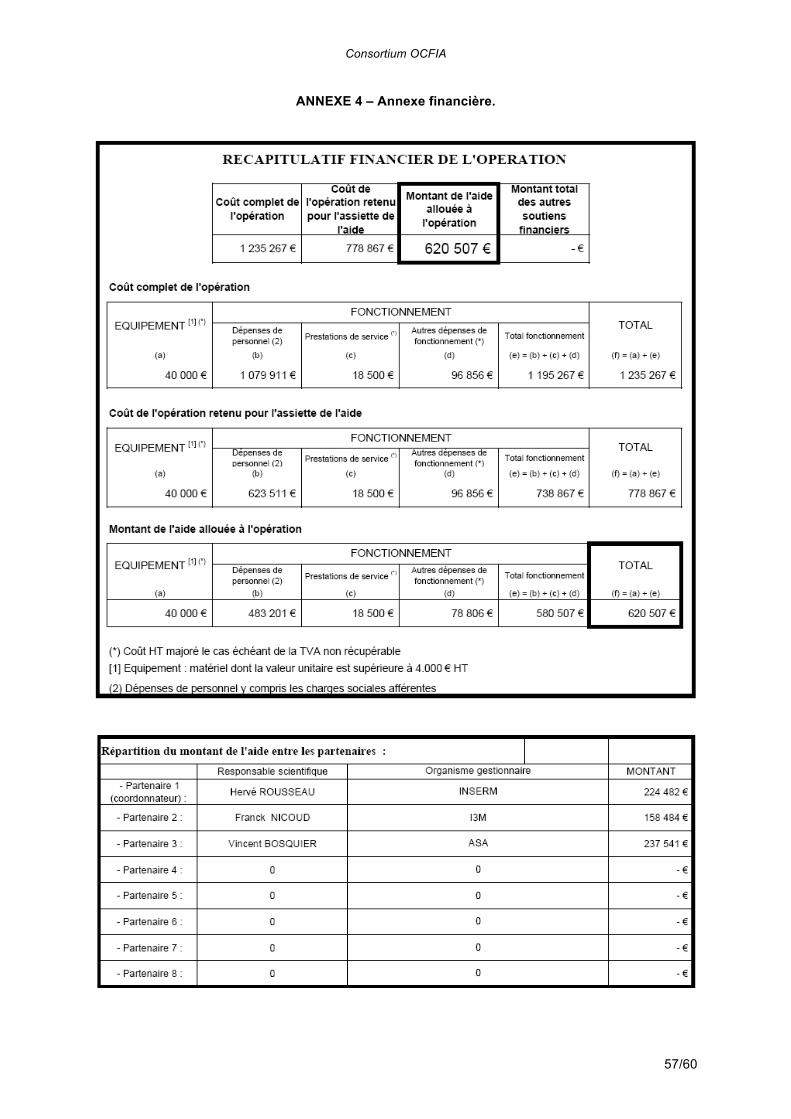
Consortium OCFIA
57/60
ANNEXE 4 – Annexe financière.
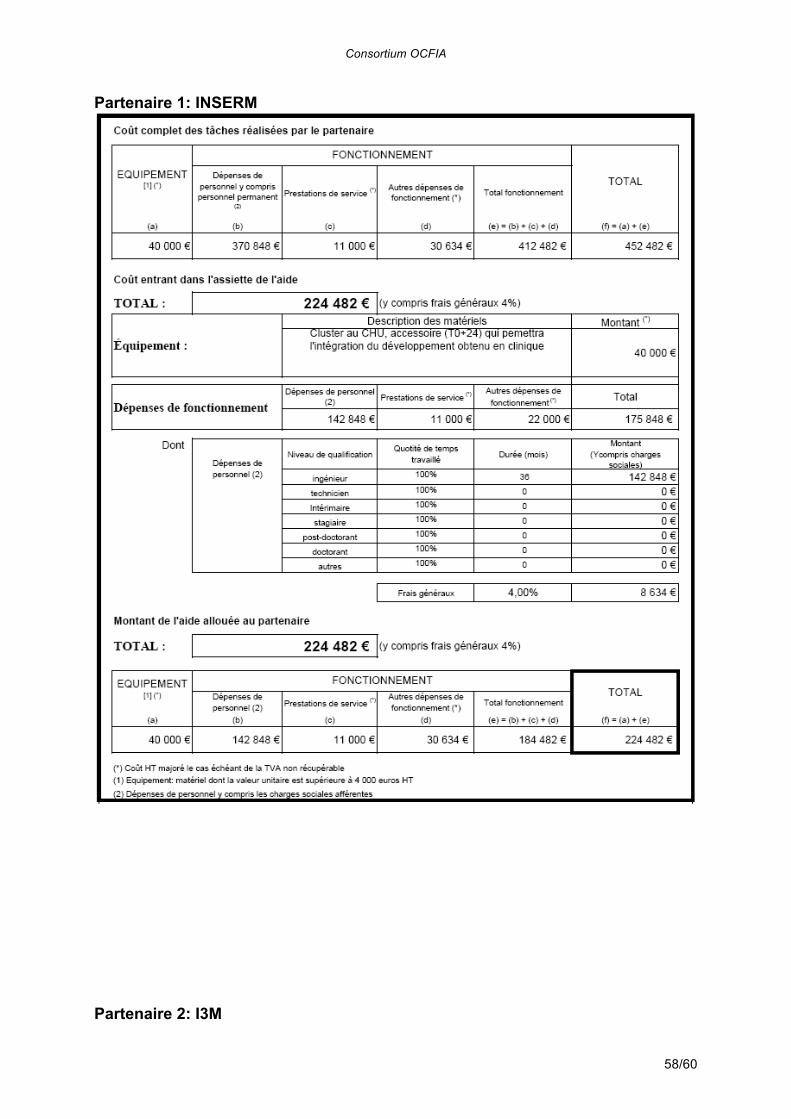
Consortium OCFIA
58/60
Partenaire 1: INSERM
Partenaire 2: I3M
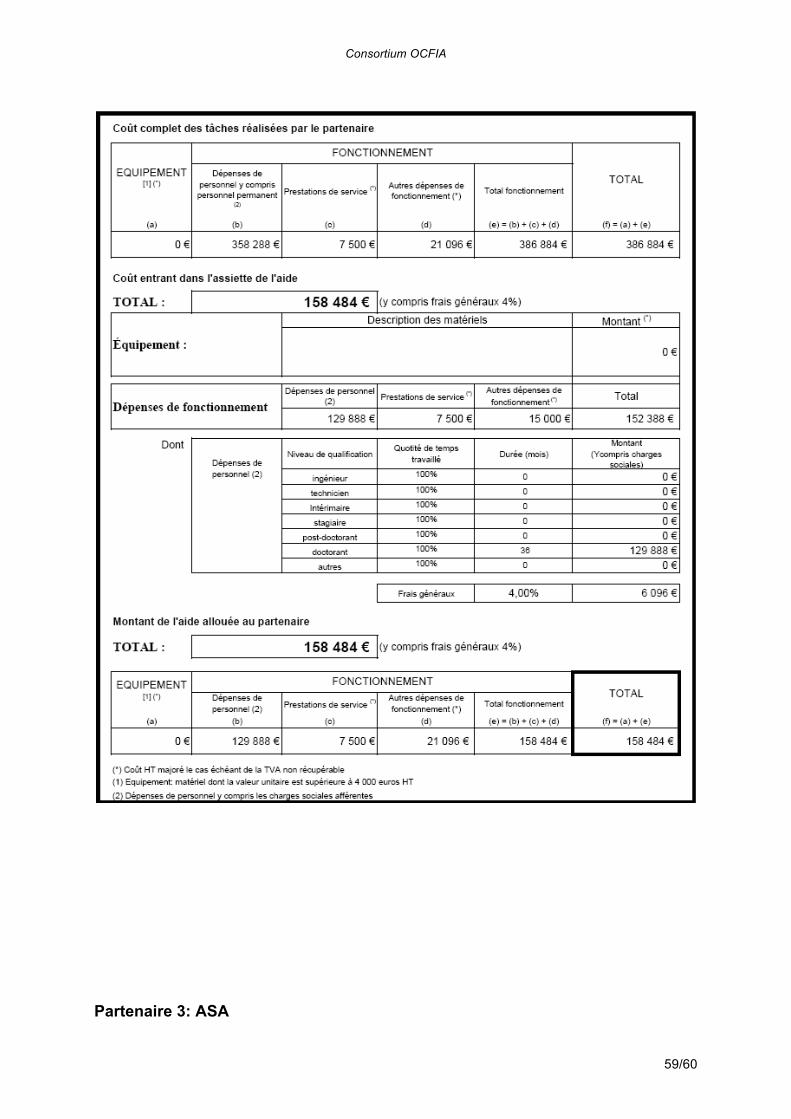
Consortium OCFIA
59/60
Partenaire 3: ASA
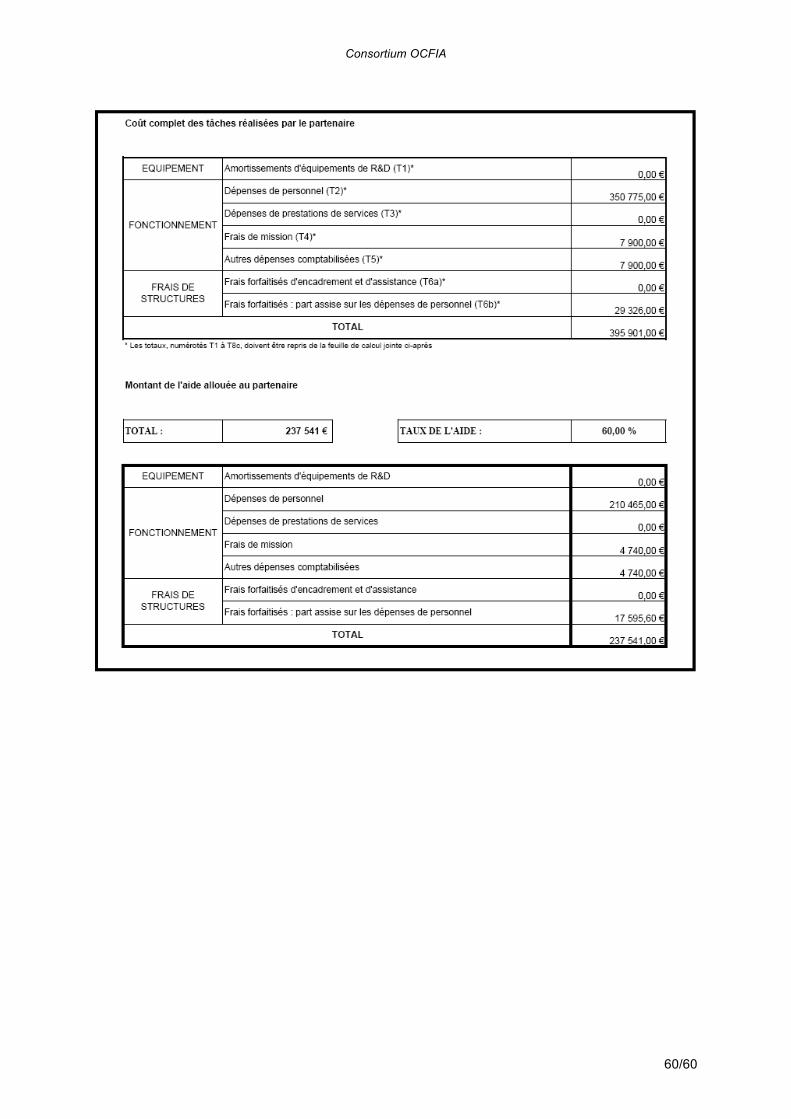
Consortium OCFIA
60/60


















