Classic reaction kinetics can explain complex patterns of ...€¦ · INFECTIOUS DISEASE Classic...
12
INFECTIOUS DISEASE Classic reaction kinetics can explain complex patterns of antibiotic action Pia Abel zur Wiesch, 1,2 * Sören Abel, 3,4 Spyridon Gkotzis, 5 Paolo Ocampo, 6,7 Jan Engelstädter, 8 Trevor Hinkley, 9 Carsten Magnus, 10 Matthew K. Waldor, 3,11 Klas Udekwu, 5 Ted Cohen 1,2,12 Finding optimal dosing strategies for treating bacterial infections is extremely difficult, and improving therapy re- quires costly and time-intensive experiments. To date, an incomplete mechanistic understanding of drug effects has limited our ability to make accurate quantitative predictions of drug-mediated bacterial killing and impeded the rational design of antibiotic treatment strategies. Three poorly understood phenomena complicate predictions of antibiotic activity: post-antibiotic growth suppression, density-dependent antibiotic effects, and persister cell for- mation. We show that chemical binding kinetics alone are sufficient to explain these three phenomena, using single- cell data and time-kill curves of Escherichia coli and Vibrio cholerae exposed to a variety of antibiotics in combination with a theoretical model that links chemical reaction kinetics to bacterial population biology. Our model reproduces existing observations, has a high predictive power across different experimental setups (R 2 = 0.86), and makes several testable predictions, which we verified in new experiments and by analyzing published data from a clinical trial on tuberculosis therapy. Although a variety of biological mechanisms have previously been invoked to explain post- antibiotic growth suppression, density-dependent antibiotic effects, and especially persister cell formation, our find- ings reveal that a simple model that considers only binding kinetics provides a parsimonious and unifying explanation for these three complex, phenotypically distinct behaviours. Current antibiotic and other chemotherapeutic regimens are often based on trial and error or expert opinion. Our “chemical reaction kinetics”–based approach may inform new strategies, which are based on rational design. INTRODUCTION Although antibiotics have been used in medicine for more than 70 years, a clear mechanistic understanding of how these agents influence micro- bial populations in the host and how their concentration affects their activity (antibiotic pharmacodynamics) has not yet been achieved. The pharmacodynamics of antibiotics have been difficult to predict even in simple settings such as the growth of Escherichia coli in vitro. In addition, the large number of possible regimens makes it nearly im- possible to test optimal dosing intervals, dose levels, and treatment du- ration in clinical settings (1, 2). Although less frequent dosing may promote patient adherence to treatment (3), antibiotics must be provided with sufficient frequency to clear pathogens. Identifying the optimal dosing frequency is challenging; for example, in the maintenance phase of tuberculosis ther- apy, it is currently unclear if intermittent therapy is inferior to daily ther- apy (4–6). Predictions of optimal dosing intervals are complicated by the fact that for some bacteria/antibiotic combinations, bacterial growth remains suppressed after removal of the antibiotic. This “post-antibiotic effect” is not easily predicted and has generally been attributed to bac- terial stress responses induced by exposure to antibiotics (7, 8). A second challenge for optimizing antibiotic therapy is the need to identify dose levels that reliably clear the infection. Several recent clinical studies have been designed to address the impact of different antibiotic concentrations on patient outcome (9, 10). Predictions of optimal dose levels are complicated by the fact that, for some bacteria/antibiotic com- binations, the dose necessary for bacterial killing can depend on initial bacterial density (11). This “inoculum effect” is again not easily pre- dicted and has been attributed to various mechanisms including density- dependent bacterial communication (12), drug-degrading enzymes (13), and/or differences in bacterial metabolic states at different densi- ties (14). Commonly used measures of bacterial susceptibility such as minimum inhibitory concentration (MIC) can vary with bacterial den- sity (11), so translating a MIC established at a specific bacterial density (15, 16) into a recommended dosing level may not produce optimal treatment outcomes. In many bacterial infections, the treatment duration necessary to prevent relapse is unclear (17–21). Excessively long treatment risks increased toxicity, incurs unnecessary costs, and may accelerate the emergence of resistance (22). Predictions of optimal treatment duration are complicated by the fact that some bacteria exhibit persistence under antibiotic pressure; this phenomenon is defined as a slowing of antibiotic- mediated bacterial killing over time and occurs in the absence of mutation- mediated resistance. A large number of mechanisms to explain the generation of “persister” cells have been proposed, but the biological basis of persistence remains an ongoing controversy in microbiology (23–35). Given the relationship of persistence to treatment duration, the inability to reliably predict persistence has challenged efforts to identify optimal lengths of antibiotic therapy. Here, we provide a simple mathematical model that links chem- ical reaction kinetics to bacterial population biology and provides a 1 Division of Global Health Equity, Brigham and Women’ s Hospital and Harvard Medical School, 641 Huntington Avenue, Boston, MA 02115, USA. 2 Department of Epidemiology of Microbial Diseases, Yale School of Public Health, 60 College Street, New Haven, CT 06510, USA. 3 Division of Infectious Diseases, Brigham and Women’ s Hospital and Harvard Medical School, 181 Longwood Avenue, Boston, MA 02115, USA. 4 Department of Pharmacy, UiT, The Arctic University of Norway, 9037 Tromsø, Norway. 5 Department of Neuroscience, Karolinska Institutet, Retzius väg 8, 17177 Stockholm, Sweden. 6 Institute of Integrative Biology, ETH Zürich, Universitätsstrasse 16, 8092 Zürich, Switzerland. 7 Department of Environmental Microbiology, EAWAG, Überlandstrasse 133, 8600 Dübendorf, Switzerland. 8 School of Biological Sciences, University of Queensland, Brisbane, Queensland 4072, Australia. 9 School of Chemistry, University of Glasgow, University Avenue, Glasgow G12 8QQ, UK. 10 Institute of Medical Virology, University of Zürich, Winterthurerstrasse 190, 8057 Zürich, Switzerland. 11 Howard Hughes Medical Institute, 181 Longwood Avenue, Boston, MA 02115, USA. 12 Department of Epidemiology, Harvard School of Public Health, 677 Huntington Avenue, Boston, MA 02115, USA. *Corresponding author. E-mail: [email protected] RESEARCH ARTICLE www.ScienceTranslationalMedicine.org 13 May 2015 Vol 7 Issue 287 287ra73 1 by guest on June 7, 2020 http://stm.sciencemag.org/ Downloaded from
Transcript of Classic reaction kinetics can explain complex patterns of ...€¦ · INFECTIOUS DISEASE Classic...

R E S EARCH ART I C L E
I N FECT IOUS D I S EASE
Classic reaction kinetics can explain complex patternsof antibiotic actionPia Abel zur Wiesch,1,2* Sören Abel,3,4 Spyridon Gkotzis,5 Paolo Ocampo,6,7 Jan Engelstädter,8
Trevor Hinkley,9 Carsten Magnus,10 Matthew K. Waldor,3,11 Klas Udekwu,5 Ted Cohen1,2,12
http://D
ownloaded from
Finding optimal dosing strategies for treating bacterial infections is extremely difficult, and improving therapy re-quires costly and time-intensive experiments. To date, an incomplete mechanistic understanding of drug effectshas limited our ability to make accurate quantitative predictions of drug-mediated bacterial killing and impededthe rational design of antibiotic treatment strategies. Three poorly understood phenomena complicate predictionsof antibiotic activity: post-antibiotic growth suppression, density-dependent antibiotic effects, and persister cell for-mation. We show that chemical binding kinetics alone are sufficient to explain these three phenomena, using single-cell data and time-kill curves of Escherichia coli and Vibrio cholerae exposed to a variety of antibiotics in combinationwith a theoretical model that links chemical reaction kinetics to bacterial population biology. Our model reproducesexisting observations, has a high predictive power across different experimental setups (R2 = 0.86), andmakes severaltestable predictions, which we verified in new experiments and by analyzing published data from a clinical trial ontuberculosis therapy. Although a variety of biological mechanisms have previously been invoked to explain post-antibiotic growth suppression, density-dependent antibiotic effects, and especially persister cell formation, our find-ings reveal that a simplemodel that considers only binding kinetics provides a parsimonious andunifying explanationfor these three complex, phenotypically distinct behaviours. Current antibiotic and other chemotherapeutic regimensare oftenbasedon trial and error or expert opinion. Our “chemical reaction kinetics”–based approachmay informnewstrategies, which are based on rational design.
stm
by guest on June 7, 2020.sciencemag.org/
INTRODUCTION
Although antibiotics have been used inmedicine for more than 70 years,a clearmechanistic understanding of how these agents influencemicro-bial populations in the host and how their concentration affects theiractivity (antibiotic pharmacodynamics) has not yet been achieved.The pharmacodynamics of antibiotics have been difficult to predicteven in simple settings such as the growth of Escherichia coli in vitro.In addition, the large number of possible regimens makes it nearly im-possible to test optimal dosing intervals, dose levels, and treatment du-ration in clinical settings (1, 2).
Although less frequent dosing may promote patient adherence totreatment (3), antibiotics must be provided with sufficient frequencyto clear pathogens. Identifying the optimal dosing frequency ischallenging; for example, in themaintenance phase of tuberculosis ther-apy, it is currently unclear if intermittent therapy is inferior to daily ther-apy (4–6). Predictions of optimal dosing intervals are complicated bythe fact that for some bacteria/antibiotic combinations, bacterial growthremains suppressed after removal of the antibiotic. This “post-antibiotic
1Division of Global Health Equity, Brigham and Women’s Hospital and Harvard MedicalSchool, 641 Huntington Avenue, Boston, MA 02115, USA. 2Department of Epidemiology ofMicrobial Diseases, Yale School of Public Health, 60 College Street, New Haven, CT 06510,USA. 3Division of Infectious Diseases, Brigham and Women’s Hospital and Harvard MedicalSchool, 181 Longwood Avenue, Boston, MA 02115, USA. 4Department of Pharmacy, UiT,The Arctic University of Norway, 9037 Tromsø, Norway. 5Department of Neuroscience,Karolinska Institutet, Retzius väg 8, 17177 Stockholm, Sweden. 6Institute of IntegrativeBiology, ETH Zürich, Universitätsstrasse 16, 8092 Zürich, Switzerland. 7Department ofEnvironmental Microbiology, EAWAG, Überlandstrasse 133, 8600 Dübendorf, Switzerland.8School of Biological Sciences, University of Queensland, Brisbane, Queensland 4072,Australia. 9School of Chemistry, University of Glasgow, University Avenue, Glasgow G128QQ, UK. 10Institute of Medical Virology, University of Zürich, Winterthurerstrasse 190, 8057Zürich, Switzerland. 11Howard Hughes Medical Institute, 181 Longwood Avenue, Boston,MA 02115, USA. 12Department of Epidemiology, Harvard School of Public Health, 677Huntington Avenue, Boston, MA 02115, USA.*Corresponding author. E-mail: [email protected]
www.Sci
effect” is not easily predicted and has generally been attributed to bac-terial stress responses induced by exposure to antibiotics (7, 8).
A second challenge for optimizing antibiotic therapy is the need toidentify dose levels that reliably clear the infection. Several recent clinicalstudies have been designed to address the impact of different antibioticconcentrations on patient outcome (9, 10). Predictions of optimal doselevels are complicated by the fact that, for some bacteria/antibiotic com-binations, the dose necessary for bacterial killing can depend on initialbacterial density (11). This “inoculum effect” is again not easily pre-dicted and has been attributed to various mechanisms including density-dependent bacterial communication (12), drug-degrading enzymes(13), and/or differences in bacterial metabolic states at different densi-ties (14). Commonly used measures of bacterial susceptibility such asminimum inhibitory concentration (MIC) can vary with bacterial den-sity (11), so translating a MIC established at a specific bacterial density(15, 16) into a recommended dosing level may not produce optimaltreatment outcomes.
In many bacterial infections, the treatment duration necessary toprevent relapse is unclear (17–21). Excessively long treatment risksincreased toxicity, incurs unnecessary costs, and may accelerate theemergence of resistance (22). Predictions of optimal treatment durationare complicated by the fact that some bacteria exhibit persistence underantibiotic pressure; this phenomenon is defined as a slowing of antibiotic-mediatedbacterial killingover time andoccurs in the absenceofmutation-mediated resistance. A large number of mechanisms to explain thegeneration of “persister” cells have been proposed, but the biologicalbasis of persistence remains an ongoing controversy in microbiology(23–35). Given the relationship of persistence to treatment duration, theinability to reliably predict persistence has challenged efforts to identifyoptimal lengths of antibiotic therapy.
Here, we provide a simple mathematical model that links chem-ical reaction kinetics to bacterial population biology and provides a
enceTranslationalMedicine.org 13 May 2015 Vol 7 Issue 287 287ra73 1

R E S EARCH ART I C L E
coherent explanation for the post-antibiotic effect, inoculum effect,and persistence. This model describes the reaction between antibioticand target molecules and the resulting effects on bacterial growth anddeath. The central principle informing this multiscale model is thatbacterial growth slows and/or death increases as a function of the frac-tion of free target.
http://stm.scie
Dow
nloaded from
RESULTS
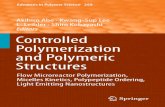
Post-antibiotic effectIn earlier work (36), we observed a pronounced post-antibiotic effect insingle E. coli cells at sub-MIC concentrations of tetracycline. We there-fore investigated post-antibiotic growth suppression by observing elon-gation and replication of single E. coli cells in microfluidic chambers.E. coli cells were grown in complex medium without antibiotics for atleast 4 hours to measure baseline rates of replication. This was followedby drug exposure for 16 hours. The mediumwas then switched back todrug-free broth for at least four more hours. For bacteria challengedwith subinhibitory concentrations of the bacteriostatic drug tetracycline(fig. S1 and movie S1), we observed slower growth, but no bacterialdeath (as defined by either lysis or failure to resume both elongationand replication in the post-antibiotic phase). The suppression of repli-cation in living cells lasted several hours longer than antibiotic exposure(Fig. 1).
We used the previous finding that after exposure to subinhibitoryconcentrations of translation inhibitors such as tetracycline, bacterial
www.Sci
by guest on June 7, 2020ncem
ag.org/
growth rate depends linearly on the fraction of free ribosomes (37) tolink bacterial replication to intracellular reaction kinetics in our bacte-riostatic model (Eq. 2 and Materials and Methods). We then used thismodel parameterized with in vitro binding data for tetracycline to ribo-somes to fit nonspecific binding rates, the critical replication threshold,and diffusion into the cytosol. From our fit, we estimated the followingfree parameters: net diffusion through inner and outer cell membraneP = 2 × 10−11 m/s, critical fraction of free ribosomes fc = 2.6%, and non-specific association rate ku,f = 50 and nonspecific dissociation rate ku,r =0.99.Note that each of these parameters aggregates several different pro-cesses and does not directly translate into a single chemical process. Themodel reproduced observed patterns of post-antibiotic growth suppres-sion at each tetracycline concentration, suggesting that the kinetics ofantibiotic-target binding are sufficient to explain this effect (Fig. 1).Twomechanisms likely underlie this phenomenon: (i) antibiotic-targetcomplexes do not dissociate immediately and intracellular antibioticmolecules only slowly diffuse across the cell membrane, and (ii) antibi-oticmolecules boundnonspecificallywith low affinity are releasedwhenthe intracellular antibiotic concentration drops and can then bind pref-erentially to specific binding sites. Together, these processes extend thetime before bacteria resume growth after antibiotic removal. Here, weassume that each daughter cell inherits, on average, one half of thebound molecules of the mother cell. Thus, as soon as the fraction ofbound antibiotics drops sufficiently to allow slow replication, new freetarget molecules are produced and the total fraction of bound targetsdecreases exponentially. This leads to a rapid increase of the replicationrate after post-antibiotic growth suppression.
Our model reproduces the concentration dependence of the post-antibiotic effect observed in (38, 39) (compare Fig. 1, A and B). Thisis becausemore antibiotic is bound both specifically and nonspecificallyat higher concentrations. Additionally, our model offers an explana-tion for why most antibiotics, with the notable exception of b-lactams,exhibit a post-antibiotic effect that is more pronounced in vivo thanin vitro (40). Usually, bacteria replicate more slowly in vivo than in vitro.As described above, reproduction of target molecules by replicationaccelerates the restoration of baseline growth rates. Thus, ourmodel pre-dicts that slower replication is associated with amore pronounced post-antibiotic effect (fig. S2).
Inoculum effectWe next used parameters obtained from our model fit to these single-cell data to predict bacterial growth in batch cultures starting from dif-ferent initial bacterial densities and exposed to different tetracyclineconcentrations. The model achieved an excellent fit (adjusted R2 =0.86; Fig. 2, A to C) for growth suppression at 12 initial bacterial den-sities and seven antibiotic concentrations (each measured in triplicate).Thus, our model predicts that the efficacy of tetracycline for suppressinggrowth depends on the initial bacterial density. We repeated the sameexperiment for four additional antibiotics with E. coli and six antibioticswith V. cholerae (Materials and Methods and table S1). In each case, an-tibiotic action declined with increasing bacterial density. Our model pre-dicts this effect because the antibiotic is not anunlimited resource, and thepool of free antibiotic is depleted as more target molecules are bound.
Although we observed an inoculum effect for all tested antibioticswith bothV. cholerae and E. coli, themagnitude of this effect differed.We hypothesized that the size of this effect is a function of differ-ences in drug-target affinity. The tighter a drug binds its target, thelower the antibiotic concentrations needed to achieve sufficient binding.
0 5 10 15 20
02
46
6.25 mg/liter tetracycline
Time [h]
Rep
licat
ion
s [/
h]
Exp. meanModelExp. min. & max
0 5 10 15 20
02
46
12.5 mg/liter tetracycline
Time [h]
Rep
licat
ion
s [/
h]
A
B
Fig. 1. Post-antibiotic effect observed with single-cell microscopy andmodel fit. (A and B) Time-lapse microscopy of single E. coli cells observed
(imaging rate: one in 5min) during and after a 16-hour exposure to two con-centrations: 22 cells at a tetracycline dose of 6.25mg/liter (0.4MIC) (A) and 27cells at a tetracycline dose of 12.5 mg/liter (0.8 MIC) (B), corresponding to 0.4and 0.8MIC, respectively. The solid black line indicates themean growth rateof the observed bacterial population, and the dotted blue lines indicate theminimal andmaximal observedgrowth rate. Themodel used to fit thedata isdescribed in Eq. 2 in Supplementary Materials and Methods. Kinetic param-eters are derived from literature cited in table S2.enceTranslationalMedicine.org 13 May 2015 Vol 7 Issue 287 287ra73 2

R E S EARCH ART I C L E
The fractional change in drug availability upon binding of target mole-cules should therefore increase with drug-target affinity. Accordingly, themodel predicts that the size of the inoculum effect will depend on affinity.We tested this prediction by correlating the drug concentration needed tobind 50% of the target molecules to the strength of the inoculum effect(defined in Materials and Methods). Consistent with this prediction, foreach bacterial species, we observed a significant correlation (linear regres-sion, E. coli: P= 6.2 × 10−4, adjusted R2 = 0.58;V. cholerae: P= 6.0 × 10−4,
www.Sci
adjusted R2 = 0.50) between affinity and the magnitude of the inoculumeffect (Fig. 2, D and E). An additional factor influencing the strength ofthe inoculum effect may be the strength of off-target binding, but thisremains to be investigated.
PersistenceFor many antibiotic/bacteria pairs, the rate of bacterial killing declinesover time. The decreased susceptibility of the persistent subpopulation
enceTranslationalMedicine.org
by guest on June 7, 2020http://stm
.sciencemag.org/
Dow
nloaded from
cannot be explained by inherited differ-ences, because the same pattern is ob-served when the persisting cells are isolated,regrown, and again exposed to antibio-tics. Rather, persistence has usually beeninterpreted as evidence of two phenotyp-ically distinct bacterial subpopulations: amajority population that is killed quicklyand a persistent subpopulation that de-clines more slowly (24). Implicit in thisexplanation of persistence is that the killrate for each subpopulation, although dif-ferent from each other, remains constantover time such that each subpopulationis expected to decline exponentially dur-ing treatment.
Balaban et al. (23) developed a mod-el to describe persistence in ampicillin-treated E. coli in which they assume adistinct subpopulation of tolerant bacteriathat switch randomly between suscepti-bility and persistence. This model pre-dicts that the level of persistence will beindependent of the drug concentration(Fig. 3) because the rate of switching lim-its the rate of bacterial killing such thathigher antibiotic doses do not produceadditional killing. Analysis of experimen-tal data derived from Regoes et al. (41) (fig.S3) confirms concentration-independentpersistence for some antibiotics, includingampicillin, which was investigated withthe original model from Balaban et al.(23). However, in contrast to these exam-ples, we found that of the five antibiotics wetested, there was a strong correlation be-tween persistence and antibiotic concentra-tion for both streptomycin (P = 0.012;adjusted R2 = 0.78) and ciprofloxacin (P =0.011; adjusted R2 = 0.70), a phenomenonthat is not consistent with the model ofBalaban et al.
We investigated whether our model,which considers the reaction kinetics ofantibioticswith their targets, could explainlag phases and concentration-dependentpersistence. When E. coli is exposed to in-hibitory concentrations of streptomycin, abactericidal antibiotic that targets ribo-somes and one of the antibiotics with
10–10 10–9 10–8 10–7 10–6
0.0
0.5
1.0
1.5
2.0
Half-maximal target binding [M]
P = 6.0 10–4 , adj. R2 = 0.50
AmpGenTetCipPenRif
10–10 10–9 10–8 10–7 10–6 10–5 10–4
0.0
1.0
2.0
3.0
Half-maximal target binding [M]
P = 6.2 10–4 , adj. R2 = 0.58
AmpGenNalStrTet
D E
[Antibiotic]
[mg/liter]
124681216
0.5
0.4
0.3
0.2
0.1
0.0
0.6
Rela
tive
bac
teri
al d
ensi
ty
5.0x107
4.9x1049.8x104
2.0x1053.9x105
7.8x1051.6x106
3.1x1066.3x106
1.3x1072.5x107
2.4x104Initial bacterial density [CFU/ml]
12468
1216
[Tet
racy
clin
e] [m
g/l
iter
]
0.5
0.4
0.3
0.2
0.1
0.0
0.6
Rela
tive
bac
teri
al d
ensi
ty
5.0x107
4.9x104
9.8x104
2.0x105
3.9x105
7.8x105
1.6x106
3.1x106
6.3x106
1.3x107
2.5x107
2.4x104Initial bacterial density [CFU/ml]
BA Theoretical predictionExperimental average
[Antibiotic]
[mg/liter]
124681216
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7
0.0
0.2
0.4
0.6
Relative bacterial load(predicted)
Rela
tive
bac
teri
al lo
ad(e
xper
imen
tal)
Adj. R2 = 0.86, P < 2 10–16
C
Experiment IExperiment IIExperiment III
10 C
FU
10 C
FU
Fig. 2. Influence of bacterial density on antibiotic efficacy. These graphs show the relative bacterialpopulation size over 12 hours with different tetracycline concentrations as compared to growth in the ab-
sence of antibiotics. (A) E. coliwere grown in microtiter plates with different initial densities and exposed todifferent tetracycline concentrations (the MIC is 2 mg/liter); the graph shows relative population size in thepresence versus in the absence of antibiotic. The average of three independent experiments is shown. CFU,colony-formingunits. (B)Model prediction usingparameters fromsingle cells. (C) Predictive power ofmodel.The y axis shows the average bacterial density over 12 hours as observed by turbidity measurements inmicrotiter plates. Bacterial cultures with different initial densities were exposed to varying concentrationsof tetracycline (A). The x axis shows the theoretical prediction derived from our model parameterized withknown binding data and the parameter estimates from fitting themodel to single-cell data (Fig. 1, A and B).(D) Correlation between strength of inoculum effect (efficacy loss/log10 bacteria) and drug-target affinity(half-maximal target binding) in E. coli. For details, see Supplementary Materials and Methods, “Quantifica-tion of inoculum effect.” The experimental setupwas the same as in (A). (E) Same as in (D) for Vibrio cholerae.Amp, ampicillin; Gen, gentamicin; Nal, nalidixic acid; Str, streptomycin; Tet, tetracycline; Cip, ciprofloxacin;Pen, penicillin; Rif, rifampicin.13 May 2015 Vol 7 Issue 287 287ra73 3

R E S EARCH ART I C L E
Dow
nlo
concentration-dependent persistence, replication ceases rapidly (fig. S4and movie S2). This fast killing allows us to ignore growth during thisphase and approximates a kill curve by only following the time to deathfor individual cells. By simplifying the problem, we can create a modelthat facilitates conceptual understanding of the involved mechanismsand how its predictions are influenced by parameter changes. We usetheMIC determined for fig. S4 and data on intracellular ribosomal con-centration measured in E. coli (42), which follow a normal distributionwith 15.8% variance (Fig. 4A, Shapiro test for a departure from thenormal distribution was not significant). Streptomycin leads to the pro-duction of aberrant proteins, which accumulate and ultimately kill thecell, potentially by damage of membrane integrity (43, 44). Therefore,we assumehere a toxicmechanismof bacterial killingwhere the cells diewhen a threshold of bound target is exceeded (see Materials andMethods). To define the threshold of how many ribosomes have tobe bound by the antibiotic to cause cell death (tc), we determined thenumber of bound targets in equilibrium at theMIC for the cell with thelowest ribosomal content. This cell is least susceptible because the intra-cellular concentration of target is lowest, and therefore, the required
www.Sci
threshold will be reached latest (Eq. 5 and Supplementary Materialsand Methods). In the simplest case, this system is described by fol-lowing only the reaction of antibiotic molecules with targets. Withthis model, the kill curves predicted from the measured distribution inribosomal content do not exhibit a log-linear decay, but instead exhibita concentration-dependent convex curve (apparent multiphasic killcurve) and a lag phase (Fig. 4B). From a chemical kinetic perspective,a log-linear decay would only be expected if binding of a single targetmolecule were sufficient for bacterial killing, which is not realistic. If thebinding of more than one target molecule is needed for bacterial killing,the onset of killing is delayed because bacterial killing can only start aftersufficient target molecules are bound (fig. S5). Experimental data sug-gest that many targets must be occupied for activity; for example, withsome b-lactams, >90% of penicillin-binding proteins are occupied at MIC(45–47). A delay in the onset of antibiotic action has been frequentlyobserved for b-lactam antibiotics (12, 48).
In our model, each cell is characterized by a threshold tc represent-ing a critical amount of bound targets or toxic metabolites that elicitdeath (Fig. 4C). If the target molecule concentration (or, more general,
enceTranslationalMedicine.org
by guest on June 7, 2020http://stm
.sciencemag.org/
aded from
susceptibility as characterized by the frac-tion of occupied target eliciting bacterialdeath) varies slightly, very large variationsin the time to death can result. This is be-cause the time until the critical fraction ofbound targets is reached is not propor-tional to tc as the reaction slows downwhen the equilibrium fraction is approached(Fig. 4C). As tc nears this equilibrium frac-tion, the skew of the distribution of time todeath for each cell increases. Accordingly,bacteria that die at slightly different thresh-olds of bound target will be killed much lat-er than others, and these cells might beidentified as “persisters.” That is, even a nar-row normal distribution in bacterial suscep-tibility attributable to stochastic variation inintracellular target concentration is expectedto produce a highly skewed distribution ofthe expected time to kill in a bacterial pop-ulation. In contrast to previous mathemati-cal models, our model, which does notinclude a distinct tolerant subpopulation,predicts that persistence will be less pro-nounced at high antibiotic concentrationsbecause the expected equilibrium of boundtarget molecules rises with the antibioticconcentration.
As described above, the prevalent ex-planation for persistence assumes two dis-tinct subpopulations.We therefore usedourmodel to explore whether concentration-dependent persistence is conceptually in-compatible with subpopulations or whetherthey are merely not needed to explain thephenomenon. Here, we interpret the term“subpopulation” as a bimodal distribution(that is, two “peaks”) of a trait, in our caseantibiotic susceptibility. In the majority
Classical model
Antibiotic susceptibility0.0 0.2 0.4 0.6 0.8 1.0
# B
acte
ria
04
10
66
Phenotypic switch
BA
Bac
teri
al d
ensi
ty [C
FU/m
l]
Time [h]0 10 20 30 40 50
100
10,0
001
0.512
Antibiotic kill rate(1=100 mg/liter amp)
8
10
Fig. 3. Model of persistence as tolerant subpopulations with phenotypic switch compared toalternative model. (A) This graph shows numerical simulations of the mathematical model proposed by
Balaban et al. (23). In brief, this model assumes that there is a majority population of susceptible (“normal”)bacteria, n, and a subpopulation of persistent bacteria, p. According to the data in (23) (represented by redline), themajority populationdeclines quicklywith a rate mnof ~0.4 orders ofmagnitude per hour (mn=−1.84hour−1) at an ampicillin dose of 100mg/liter, the persister population is not affectedby the antibiotic (mp=0),andbacteria switch fromapersistent to a normal statewith a rate b=0.07 hour−1. This canbedescribedwiththe following mathematical model as presented in (23):dndt
= bp + mnn
dpdt
= −bp + mpn
The black line represents an antibiotic activity that is 50% lower than 100mg/liter; the green line indicates anantibiotic activity that is twice higher. (B) “Classical model” of persistence with a majority nonpersister pop-ulation and a minority persister population. On the x axis, the antibiotic susceptibility of individual cells isgiven relative to themean of the nonpersister population, and the y axis shows the number of bacteria withthat specific susceptibility (total population size, 107). The relativeproportion of persisters under this assump-tion is usually assumed to be several orders ofmagnitude lower than themajority population. For illustrationpurposes only, we adopt a persister frequency of 10−2 (the real frequency is much lower and would not bevisible in this figure).
10
13 May 2015 Vol 7 Issue 287 287ra73 4

R E S EARCH ART I C L E
www.ScienceTranslationalMedicine.org
by guest on June 7, 2020http://stm
.sciencemag.org/
Dow
nloaded from
population (larger peak), susceptible bacte-ria die evenwhen only a low fraction of tar-get molecules are bound, whereas in thepersistent subpopulation (smaller peak),bacteria only die when a high percentageof their targetmolecules are bound. In con-trast, we interpret a narrow normal dis-tribution of the intracellular concentrationof molecules (for example, ribosomes)as stochastic variance around the mean.There are two possible scenarios: (i) achiev-ing a sufficient amount of bound target tokill the persistent subpopulation may beimpossible. This situation may arise whentoxicity or solubility limits the antibioticconcentration; in the case of Fig. 4D, thechemical equilibriumof bound targetwouldthen be between the two peaks. Becausethe antibiotic concentration can never behigh enough to kill the less susceptible sub-population, this results in concentration-independent persistence and correspondsto the classical model as proposed by (23).
(ii) If the maximal achievable concen-tration of the antibiotic is high enoughthat the fraction of bound target necessaryto kill the less susceptible subpopulationcan be reached, we observe concentration-dependent persistence. However, with abimodal distribution of susceptibility, thekill curves exhibit a pronounced shoulderas first themore susceptible and then, aftera delay, the less susceptible subpopula-tions are killed. Such a “bumpy” patternof bacterial time-kill curves is not usuallyobserved; thus, a bimodal distribution ofsusceptibility seems a less feasible explana-tion than either the standardmodel or ouralternativemodel (Fig. 4E, compare to fig. S6).
We further illustrate concentration-dependent persistence with ciprofloxacin(Fig. 5A). To show the effects of bacterialgrowth during antibiotic exposure, wecompare these results to a model thatcaptures both bacterial growth and death(Fig. 5B). Again, we find concentration-dependent persistence as a result of slightvariance in the number of target mole-cules. Cell-to-cell variation in the numberof targets or downstream effectors is almostcertainly present (42, 49, 50). Because allbacteria must have the same number oftargets for bacterial killing to be constant,a log-linear decay is not expected. Thus, weassert that amultiphasic kill curve can be ex-plained by chemical reaction kinetics alonewhen the intracellular concentrationof targetvaries (even by as little as 2% SD, fig. S7).
B
Time [arb. units]0 2 4 6 8 10
0.1
0.5
210
50
Calculated kill curve
# Li
vin
g b
acte
ria
1/4x MIC
1x MIC (6 mg/liter)
4x MIC
[Streptomycin]
A
15,000 45,000
510
1520
[Ribosomes]in E. coli cells
Freq
uen
cy
# Ribosomes/1 µm3
35,00025,000
0
Shapiro testP = 0.21
E
0 10 20 30
Calculated kill curve
Time [arb. units]
40
12
3
40
# Li
vin
g b
acte
ria
[Lo
g10
(CFU
)] 1x MIC
4x MIC
8x MIC
[Antibiotic]
32x MIC
Threshold for death
Freq
uen
cy
% Occupied target0 100
5000
15,0
00
8040
0
20 60
D
Threshold for deathC
0 20 40 60 80 100
010
2030
40
% Occupied target
Tim
e [a
rb. u
nit
s]
Susc
epti
bili
ty
1/4x MIC
1x MIC (6 mg/L)
4x MIC
[Streptomycin]
Fig. 4. A normal distribution of target molecules can lead to multiphasic bacterial killing. (A) Histo-gram of intracellular ribosomal concentration as experimentally determined in E. coli. Raw data were ob-
tained from (42). Normal distribution was not rejected by Shapiro test, and the red line shows a normaldistribution with mean and SD obtained from the data. (B) Predicted killing over time for bacterial popula-tionmeasured in (A). Kinetic rates of streptomycin binding to ribosomeswere taken from the literature (tableS3). Timeof killingwas calculated using Eq. 4. The colors indicate antibiotic concentrations relative to theMICof E. coliMG1655. (C) Theoretical explanation ofmultiphasic kill curves. The dotted lines show the calculatedequilibrium number of bound ribosomes for three different streptomycin concentrations. The solid linesshow the time until a specific fraction of the targetmolecules is bound (Eq. 4, Materials andMethods). Black:Assumed killing threshold with a mean of 60% and variance of 10%. (D and E) These graphs show time-killcurves (E) resulting from a bimodal distribution of susceptibility (D, compare to fig. S6). The MIC wascalculated as the drug concentration that achieves binding of 99% of the cells at equilibrium (Eq. 5). Thevertical lines in (D) indicate the equilibria at givenmultiples of theMIC (green,1×MIC; yellow,4×MIC; orange,8× MIC; red,32× MIC). The same colors are used in the resulting calculated time-kill curves of a simulatedpopulation of 105 bacteria in (E). Kinetic rates are the same as in (A) to (C). The main “peak” of the bimodaldistribution in (D) corresponds to the normal distribution in fig. S6A.13 May 2015 Vol 7 Issue 287 287ra73 5

R E S EARCH ART I C L E
by guhttp://stm
.sciencemag.org/
Dow
nloaded from
Our model predicts that after an initial decline, the bacterial popu-lationmay subsequently increase, even in the absence of resistance. Thisoccurs because some cells are still able to replicate, increasing the totalnumber of target molecules. Consistent with this prediction, we ob-served consistent outgrowth in experimental replicates (Fig. 5A). Thisregrowth was not due to resistance because the MIC of cells at thebeginning of the experiment and of the cells remaining after 18 hours(table S1) was unchanged.
To investigate whether our findings regarding concentration-dependent persistence can be translated to in vivo settings, we analyzedclinical trial data from tuberculosis patients treated with increasingdoses of rifampicin (51) (Fig. 6, A to C). Patients received rifampicinmonotherapy for the first 14 days of treatment and then were switchedto standard combination therapy. Again, we observe concentration-dependent persistence. In addition to variance in the intracellular mol-ecule content of bacteria, antibiotic therapy in patientsmay lead to varyingdrug concentrations. There may be spatial variation of concentration indifferent target tissues as well as temporal variation of drug uptake. Wemodeled these differences using experimentally determined concentra-tions of rifampicin in the epithelial lining fluid of tuberculosis patients(52). We also assume that this concentration follows a normal distributionwith an SDas reported in patients receiving rifampicin (53). Again, we findconcentration-dependent persistence (Fig. 6D). Conceptually, variances indrug concentration and the concentration of targetmolecules are very sim-ilar. Both shift the chemical equilibrium, and depending on the proximityof the threshold for killing tc to the chemical equilibrium, the reaction rateslows down.
We would therefore expect that not only higher antibiotic doses butalso other mechanisms that shift the chemical equilibrium to higherproportions of bound targets lead to decreased persistence—one suchmechanism could be drugs with higher target affinity. Whereas ourfindings do not disprove that distinct subpopulations can generate per-sistence (33, 54), our model demonstrates that chemical kinetics alone
www.Sci
may account for multiphasic kill curves as well as concentration-dependent persistence.
Many biological mechanisms have been shown to underlie bacterialpersistence (29), and we therefore investigated whether our model canreproduce persistence resulting from known molecular mechanisms.Ourmodel also offers an explanation for persistence caused bymechan-isms not directly involved in target binding. Generally, any mechanismthat increases the variance of antibiotic susceptibility (even if up- ordownstream of target binding) in a bacterial population can lead toan increase of persister-like behavior at specific drug concentrations.A similar argument has been made forM. tuberculosis exposed to iso-niazid (31).
We use isoniazid as an example to illustrate how variation in anti-biotic prodrug activation can lead to persistence.M. tuberculosis persist-ence during therapy with isoniazid has been shown to decrease withincreasing partial pressure of O2 (28), as well as increasing levels ofthe prodrug activating enzyme KatG (31). Our model reproduces thesefindings (Fig. 7) and offers the following explanation: the catalase KatGrequires O2 (Fig. 7A), such that the net reaction of isoniazid (INH) ac-tivation depends linearly on the intracellular concentration of KatG andO2. This suggests that both increased levels of KatG andO2 can shift thechemical equilibrium, thereby reducing persistence (Fig. 7B). Note thata twofold increase of KatG has the same effect on the rate of prodrugactivation as a twofold increase of O2, and therefore, increasing levels ofKatGwill reduce persistence asmuch as increasing oxygen supply. Thisprediction is in accordance with experimental results linking high KatGlevels to reduced persistence (31).
Concentration-independent persistence is in concordance with pre-vious explanations and theoretical models. However, our model alsooffers a potential explanation for concentration-independent persist-ence. Here, we assume some cell-to-cell variation in the activation ofisoniazid and confirm that variance in KatG levels can lead to persist-ence (31) (Fig. 7C). When the main sources of variance in the bacterial
enceTranslationalMedicine.org
est on June 7, 2020
population are up- or downstream ofdrug-target binding such as in the caseof prodrug activation or autolysin activa-tion (55), increasing the antibiotic dosehas little effect on the least susceptiblecells. In this case, our model predictsconcentration-independent persistence.According to our model, we would expectthis type of persistence to become less ap-parent when the concentration of reactionpartners in the metabolic step with thegreatest variance is increased (such as O2
in isoniazid activation, Fig. 7). Our modelreproduces the slowdecline ofmycobacte-rial populations over several days basedon chemical kinetics of drug activationand binding alone. Thus, we can also ex-plain persistence for very long time framesup to several weeks.
DISCUSSION
Currently, we do not have sufficientunderstanding of antibiotic action and
10 9
10 8
10 7
10 6
10 5
10 4
10 3
10 2
10 1
Bac
teri
al d
ensi
ty [C
FU/m
l]
0 15105 20Time [h]
10 10
109
108
107
106
105
104
103
102
101
Bac
teri
al d
ensi
ty [C
FU/m
l]
0 15105 20Time [h]
1010
Detection limit
0
8163264128256
4
[Cip] [µg/liter]0
3035404550
20
[Cip] [µg/liter]
A B
Fig. 5. Modeling reproduces concentration-dependentpersistence. (A) Experimental time-kill curves ofE. coli with different ciprofloxacin concentrations. The MIC is 8 mg/liter (table S1). The experiment was per-
formed in biologically independent triplicates. (B) Numerical simulations of amodel combining bacteriostat-ic and bacteriocidal effects (Eqs. 7 to 10) parameterized with in vitro kinetic parameters for ciprofloxacinbinding. In the absence of known distributions of functional gyrase tetramers, we assume that the meanof this distribution is the average of the numbers given in the literature as cited in table S3. We assume anormal distribution in the absence of more detailed information (60, 61) and that the SD is the same aspublished for ribosomes.13 May 2015 Vol 7 Issue 287 287ra73 6

R E S EARCH ART I C L E
pharmacodynamics to reliably predict antibacterial action and designrational treatment strategies. Our incomplete understanding of thepost-antibiotic effect has hampered efforts to identify optimal dosingintervals, such as in the maintenance phase of tuberculosis therapy(4–6). Finding optimal dose levels is difficult without knowing howthe inoculumeffectmight change bacterial susceptibilitywith increasingdensity (9–11). In nearly all bacterial infections, persister cells have chal-lenged efforts to predictwhich treatment durations are sufficient to clearinfections (20, 55).
Here, we have developed a highly intuitive theoretical framework,based on and fit to experimental data. Our model, which provides amultiscale linkage between antibiotic chemical kinetics and bacterialpopulation biology within hosts, makes only two, easily defendable as-sumptions: (i) replication decreases and/or killing increases when the
www.Sci
fraction of bound target molecules rises, and (ii) the intracellular con-centration of molecules varies slightly (>1% SD in a normaldistribution) between bacteria in the same clonal population. Ourmodel exhibits high predictive power and reproduces a series ofphenomena that have typically been explained through unrelatedbiological mechanisms. Accordingly, this model may facilitate a moreunified understanding of the relationship between drug-target bindingkinetics and drug effects (Table 1). We note that our work does not dis-prove previous biological explanations of post-antibiotic effect, inocu-lum effect, and persistence, but does challenge the implicit notion thatbiological mechanisms must underlie these complex phenomena.
A better grasp of themechanisms underlying post-antibiotic growthsuppressionwould enable us tomake better predictions regarding treat-ment frequency. In contrast to previous studies attributing the post-
enceTranslationalMedicine.org
by guest on June 7, 2020http://stm
.sciencemag.org/
Dow
nloaded from
antibiotic effect to biologicalmechanisms(7, 8), we show here that it may be ex-plained by chemical processes alone.Our modeling framework makes testablepredictions regarding the strength of thepost-antibiotic effect that may be used todesign antibiotics that can be given lessfrequently. On the basis of our results,we would expect that (i) tight drug-targetbinding, (ii) difficulty in crossing the bac-terial cell envelope, and (iii) having alarge reservoir of nonspecifically bounddrugs could prolong post-antibioticgrowth suppression. However, the finaltwo properties may have other repercus-sions: difficulties in crossing the bacterialcell envelope also would imply that thedrug may not penetrate the bacteria inthe first place, and a large amount of non-specific binding sites make higher drugconcentrations necessary.
Our model attributes the inoculum ef-fect to the depletion of antibiotic mole-cules that occurs as they are bound to alarge number of targetmolecules.We pre-dict that the degree to which antibioticslose their efficacy with changing bacterialconcentrations depends on the strength ofdrug-target binding, and we were able toverify this theoretical prediction experi-mentally. Moreover, our model makeshighly accurate predictions regarding an-tibiotic efficacy (R2 = 0.86) even whencalibrated and tested in very differentexperimental systems. On the basis of thismodel, we would predict that for antibio-tics that bind their target very tightly, doselevels should be adjusted to the expectedbacterial load in the target tissue.
A very large number of biological mech-anisms underlying persistence have beendescribed, but the nature and causes ofpersistence remain controversial (23–35).Commonly observed nonlinear patterns
0–3
–2–1
1–4
0 1210864 142
Dose rifampicin5 mg/kg
Days after treatmentinitiation
Log 10
(CFU
) rel
ativ
e to
bas
elin
e
A
0–3
–2–1
1–4
0 1210864 142
Dose rifampicin20 mg/kg
Days after treatmentinitiation
Log 10
(CFU
) rel
ativ
e to
bas
elin
e
C
0–3
–2–1
1–4
0 1210864 142
Dose rifampicin10 mg/kg
Days after treatmentinitiation
Log 10
(CFU
) rel
ativ
e to
bas
elin
e
B
40
32
1
Time [arb. units]
0 4020 60
1/2x Standard therapy1x Standard therapy (5.25 mg/liter in ELF) 2x Standard therapy
[Rifampicin]
D
# Li
vin
g b
acte
ria
[log
10(C
FU)]
Fig. 6. Concentration-dependent persistence in tuberculosis patients receiving increasing rifampi-cin dosages. (A to C) CFU counts ofMycobacterium tuberculosis in sputum during treatment as reported in
(51). Patients with previously untreated, smear-positive pulmonary tuberculosis due to drug-sensitive strainsreceived 14 days of initial monotherapy and then a standard multidrug regimen. Sputum was collectedovernight on two consecutive nights before treatment was started and then after 2, 4, 6, 8, 10, 12, and14 days of the allocated regimen. Patients received rifampicin at doses of (A) 5 mg/kg, (B) 10 mg/kg (rifam-picin dosage in standard regimen), and (C) 20 mg/kg. (D) Calculated time-kill curves within patients (simu-lated population of 104 bacteria, Eqs. 4 and 5). The effective drug concentration in extracellular lining fluidwas obtained from (52). The MIC for rifampicin in drug-susceptible strains was assumed to be 0.1 mg/liter(62). The available drug concentration was assumed to follow a normal distribution with a 22.5% SD (53).13 May 2015 Vol 7 Issue 287 287ra73 7

R E S EARCH ART I C L E
www.Sci
by guest on June 7, 2020http://stm
.sciencemag.org/
Dow
nloaded from
of bacterial killing have been cited as evidence of a distinct sub-population of persister cells in bacterial populations. However, ourmodel leads us to conclude that a decline of bacterial killing over timeis expected even in the absence of special subpopulations, at least with-in a certain range of drug concentrations. This only requires smallcell-to-cell variation in target molecules, drug concentration, or mole-cules involved up- or downstream of drug-target binding, which is al-most certain to be present.
Here, we distinguish between two types of nonlinear bacterial killing:(i) concentration-dependent persistence, where higher doses reduce thenumbers of bacteria that are killed more slowly, and (ii) concentration-independent persistence, where the time-kill curves converge at the endof the experiment and the bacterial population declines at the same slowrate independent of antibiotic dosage. When the main source of vari-ance comes from reaction partners directly involved in drug-targetbinding, our model predicts concentration-dependent persistence. Thiswould arise if the number of target molecules varies, as we show withpublished data for ribosomes (42). The same pattern would also resultfrom variation in the local concentration of drugs, which we would ex-pect in patients on treatment or when there is heterogeneity in druguptake or permeability in the bacterial population. Models for persist-ence that rely on distinct subpopulations of cells cannot easily explainconcentration-dependent persistence, which we have observed both inin vitro and in clinical data.
Although concentration-independent persistence is compatible withprevious explanations and theoretical models of persistence, our modelalso offers an alternative explanation for this phenomenon. If there isstrong variance inmolecules up- or downstreamof drug-target binding,we expect concentration-independent persistence.
Our aim here is not to disprove well-establishedmechanisms of per-sister formation (23–35, 56, 57) but to caution against the assumptionthat multiphasic kill curves provide evidence of distinct subpopulationsof bacterial cells. It has recently been suggested that many differentmechanisms rather than a single common one can lead to bacterial per-sistence and that therefore the generation of persisters is a generic featureof bacteria challenged with antibiotics (29). Our work supports this viewin that it subsumes a large variety ofmechanismsunder the single conceptof variance in cellular susceptibility, for example, by variance in intra-cellular molecule content. If any of the previously reported mechanismsincreases the variance in the intracellular concentration of any moleculeinvolved in antibiotic-mediated killing, more persistence would result. If,for example, the downstream mechanisms of antibiotic action are cellcycle–dependent and therefore susceptibility is dependent on active repli-cation, ourmodelwouldpredict that a greater variance in replication rateswould lead to increased persistence. Thus, our results are in concordancewith the seminal paper by Balaban et al. (23).
Here, we have shown that even small variance in the number of tar-gets, downstream effectors, and/or cellular susceptibility is sufficient toexplain a multiphasic kill curve from a conceptual point of view andshould thus be the expected response of bacterial populations upon ex-posure to finite quantities of antibiotic molecules. This prediction is tes-table experimentally by quantifying the distribution of intracellularmolecular content in a bacterial population, as has been done before(31). We have analyzed published data from clinical trials in tuberculo-sis patients and find concentration-dependent persistence whenfollowing bacterial load in patients’ sputum, which is consistent withour theoretical framework. Our work has direct implications for antibi-otic therapy, as we predict that higher antibiotic doses, increasing
Ak f
k r
KatG, O2
INH NADINH + NAD
B
Time [days]
Persistence and oxygen saturation
01
23
45
0 5 10 15 20 25
100%50%25%
Oxygen saturation
# L
ivin
g b
acte
ria
[lo
g1
0(C
FU)]
C
0 5 10 15 20 25
01
23 1x MIC (0.1 mg/liter)
2x MIC3x MIC
Time [days]
# L
ivin
g b
acte
ria
[lo
g1
0(C
FU)]
Fig. 7. Model of isoniazid (INH) action and resulting kill curves. (A) INHforms a NAD (nicotinamide adenine dinucleotide) adduct (red spheres) with
a rate, which depends on the enzymeKatG andO2 saturation. INH-NAD thenreacts with its target InhA (blue crescents). (B) Time-kill curves resulting fromcalculating the expected time until 60% (with 10% SD) of the target mole-cules are bound (simulated population of 106 bacteria; Eq. 6; Materials andMethods). Black indicates the same intracellular oxygen content as in thecell-free experimental setup in (63), red 50% O2 saturation, and green 25%O2 saturation. (C) Time-kill curves for variance in intracellularly available KatGby 30% simulated population of 104 bacteria. All other parameters from (63).Black indicates theMIC forM. tuberculosis (28), red 2×MIC, and green 3×MIC.enceTranslationalMedicine.org 13 May 2015 Vol 7 Issue 287 287ra73 8

R E S EARCH ART I C L E
by guest on June 7, 2020http://stm
.sciencemag.org/
Dow
nloaded from
drug-target affinity, or the concentration of metabolites involved indrug action might aid in reducing persistence and thereby allowingfor shortened antibiotic treatment courses. Recent work has shownthat variance in intracellular molecule content contributes to persist-ence for cancer cells challenged with chemotherapeutic agents (58), afinding that is consistent with the results we report here.
Together, our reaction-kinetic model replicates complex patterns ofantibiotic action that have typically been attributed to disparatebiological mechanisms. This simple model successfully predicted anti-biotic efficacy across different systems and made testable qualitative
www.ScienceTranslationalMedicine.org
predictions that we subsequently verifiedexperimentally. Our model may thereforeoffer a useful platform to generate new in-sights into the formulation of rationalstrategies not only for antibiotic use but al-so for cancer chemotherapy.
MATERIALS AND METHODS
A full description of the experimentalmethods and the mathematical modelingframework can be found in Supplemen-tary Materials and Methods; a brief sum-mary is given in the following.
Experimental methodsThe specific details of themicrofluidic sys-temused in this study have been describedpreviously (36). E. coliMG1655 cells weregrown in a flow of medium. After a briefbaseline growth period without antibio-tics, an antibiotic was added to the medi-um, followed by an antibiotic-freeincubation time. Phase-contrast micro-graphs were acquired from different fieldsof view, and cell size as well as divisionrates were analyzed with the MMJ pluginfor ImageJ. Time-kill curves based onCFU of E. coli MG1655 were performedin biologically independent triplicates asdescribed previously (11, 59). For asses-
sing the inoculum effect, bacterial growth was followed by turbiditymeasurements at 600 nm inmicrotiter plates. Antibiotic concentrationswere chosen such that the highest concentration did not clear all bacte-rial densities and the lowest suppressed at least the lowest density.
Mathematical modelOurmathematicalmodel describes both the reaction between antibioticand target molecules and the effects of this reaction on bacterial growthand death (Fig. 8, fig. S8, Materials and Methods, and SupplementaryMaterials andMethods). The central principle underlying this model is
Table 1. Overview of phenomena with previous explanations and explanations suggested here.
Phenomenon
Current explanations Alternative explanationPost-antibiotic effect
Bacterial stress Extended target occupancy due to transmembrane diffusionand unspecifically bound reservoirInoculum effect
Density-dependent growth stages, quorum-sensing Reduced ratio of antibiotics/target at higher bacterial densitiesConcentration-dependentpersistence
Exposure to antibiotics at sub-MIC concentrationsstimulates generation of persisters
Small variance in drug-target binding
Concentration-independentpersistence
Phenotypic switch between persistent and“normal” populations
Small variance in processes up- or downstream of drug-targetbinding
A
kf
kr
Antibiotics
Targets
B
dB
dtr B 1 –
B
Kd B= –
[T]
[AT] + [T]
[T]
[AT] + [T]
Survival threshold Toxic threshold Toxic threshold
Tox
... ... BnBn–1
kf
n kr
A
Bx
(n–x+1) kf
x kr
(n–x) k f
(x+1) kr
A A
A
B0 B1
n kf
kr
A
C
D
Essential function: important how many target molecules are free
Primary toxic: important how many molecules are bound
Secondary toxic: important how many noxious metabolites (tox) are created
D
A A AFig. 8. Schematic of themodel. (A and B) Model overview. A bacterial cell with targetmolecules, T (in thiscase, ribosomes, blue crescents), and antibiotic molecules, A (red circles), is shown. Antibiotics must diffuse
through the bacterial cell envelopewith a diffusion constant, p, to bind their targets with an association rate,kf, to form a complex, AT, which may dissociate with a rate, kr (0 for irreversible reactions). (C) Differentmechanisms can lead to bacterial killing. Bacterial cells are shown as black oval, target molecules are shownas blue crescents, and antibiotic molecules are shown as red circles. (D) Chemical reactions of bacterial cells.For an explanation of the parameters, see main text. The color of the reaction arrow is used to highlight thecorresponding equations in Eq. 7 in the Supplementary Materials and Methods.13 May 2015 Vol 7 Issue 287 287ra73 9

R E S EARCH ART I C L E
that bacterial growth (r) decreases and/or bacterial death (d) increasesas a function of the fraction of free target molecules; [A] representsthe concentration of intracellular antibiotics, [T] is the target, [AT] is thedrug-target complex, B is the number of living bacteria, and K is thecarrying capacity (Fig. 8B). We assume that bacteria have a set numberof target molecules that may vary between individual bacterial cells.We investigated several mechanisms that underlie bacterial killingand growth suppression (Fig. 8C). In the simplest case, we ignore down-stream processes and only describe antibiotic and target molecules:Aþ T⇌
kf
krAT , with kf and kr (0 in the case of irreversible reactions) the
association and dissociation rates, respectively. If the target is intra-cellular, the antibioticmust first reach the target location, whichwe sim-plify in a single diffusion rate, p (Fig. 8A). Variables and parameters ofthe model are explained in table S4.
by guest on June 7http://stm
.sciencemag.org/
Dow
nloaded from
SUPPLEMENTARY MATERIALS
www.sciencetranslationalmedicine.org/cgi/content/full/7/287/287ra73/DC1Materials and MethodsFig. S1. Analysis of single-cell time-lapse microscopy data E. coli MG1655 cells exposed totetracycline.Fig. S2. Baseline growth rate affects length of post-antibiotic growth suppression.Fig. S3. Time-kill curves of E. coli CAB1 exposed to five different classes of antibiotics in variousconcentrations.Fig. S4. Analysis of single-cell time-lapse microscopy data for E. coli MG1655 cells exposed tostreptomycin.Fig. S5. Simulated time-kill curves under different assumptions.Fig. S6. Distribution of drug susceptibility and expected time-kill curve.Fig. S7. Effect of variance in target molecule content.Fig. S8. Overview of kill mechanisms, chemical reactions, and compartmental models used inthis study.Table S1. Ciprofloxacin persisting E. coli have not acquired higher resistance to the antibiotic.Table S2. Antibiotic concentrations used for experiments.Table S3. Kinetic parameters for different antibiotics.Table S4. Explanation of variables and parameters.Movie S1. Single-cell microscopy data for E. coli MG1655 cells exposed to tetracycline (12.5 mg/liter)(0.8× MIC).Movie S2. Single-cell microscopy data for E. coli MG1655 cells exposed to streptomycin (25 mg/liter)(2× MIC).References (64–82)
, 2020
REFERENCES AND NOTES
1. K. E. Dooley, C. D. Mitnick, M. A. DeGroote, E. Obuku, V. Belitsky, C. D. Hamilton, M. Makhene,S. Shah, J. C. M. Brust, N. Durakovic, E. Nuermberger, Old drugs, new purpose: Retooling existingdrugs for optimized treatment of resistant tuberculosis. Clin. Infect. Dis. 55, 572–581 (2012).
2. G. L. Drusano, Antimicrobial pharmacodynamics: Critical interactions of “bug and drug”.Nat. Rev. Microbiol. 2, 289–300 (2004).
3. K. S. Ingersoll, J. Cohen, The impact of medication regimen factors on adherence to chron-ic treatment: A review of literature. J. Behav. Med. 31, 213–224 (2008).
4. D. Menzies, A. Benedetti, A. Paydar, I. Martin, S. Royce, M. Pai, A. Vernon, C. Lienhardt,W. Burman, Effect of duration and intermittency of rifampin on tuberculosis treatmentoutcomes: A systematic review and meta-analysis. PLOS Med. 6, e1000146 (2009).
5. K. C. Chang, C. C. Leung, J. Grosset, W. W. Yew, Treatment of tuberculosis and optimaldosing schedules. Thorax 66, 997–1007 (2011).
6. A. Bose, S. Kalita, W. Rose, P. Tharyan, Intermittent versus daily therapy for treating tuber-culosis in children. Cochrane Database Syst. Rev. 1, CD007953 (2014).
7. E. Gelman, J. D. McKinney, N. Dhar, Malachite green interferes with postantibiotic recoveryof mycobacteria. Antimicrob. Agents Chemother. 56, 3610–3614 (2012).
8. I. Odenholt-Tornqvist, Studies on the postantibiotic effect and the postantibiotic sub-MICeffect of meropenem. J. Antimicrob. Chemother. 31, 881–892 (1993).
9. A. Zumla, P. Nahid, S. T. Cole, Advances in the development of new tuberculosis drugs andtreatment regimens. Nat. Rev. Drug Discov. 12, 388–404 (2013).
www.Scie
10. J. A. Roberts, S. K. Paul, M. Akova, M. Bassetti, J. J. De Waele, G. Dimopoulos, K. M. Kaukonen,D. Koulenti, C. Martin, P. Montravers, DALI: Defining antibiotic levels in intensive care unitpatients: Are current b-lactam antibiotic doses sufficient for critically ill patients? Clin. Infect.Dis. 58, 1072–1083 (2014).
11. K. I. Udekwu, N. Parrish, P. Ankomah, F. Baquero, B. R. Levin, Functional relationship be-tween bacterial cell density and the efficacy of antibiotics. J. Antimicrob. Chemother. 63,745–757 (2009).
12. J. M. Yarwood, D. J. Bartels, E. M. Volper, E. P. Greenberg, Quorum sensing in Staphylococ-cus aureus biofilms. J. Bacteriol. 186, 1838–1850 (2004).
13. L. D. Sabath, C. Garner, C. Wilcox, M. Finland, Effect of inoculum and of beta-lactamase onthe anti-staphylococcal activity of thirteen penicillins and cephalosporins. Antimicrob.Agents Chemother. 8, 344–349 (1975).
14. D. L. Stevens, S. Yan, A. E. Bryant, Penicillin-binding protein expression at different growthstages determines penicillin efficacy in vitro and in vivo: An explanation for the inoculumeffect. J. Infect. Dis. 167, 1401–1405 (1993).
15. P. A. zur Wiesch, R. Kouyos, J. Engelstädter, R. R. Regoes, S. Bonhoeffer, Populationbiological principles of drug-resistance evolution in infectious diseases. Lancet Infect.Dis. 11, 236–247 (2011).
16. Performance Standards for Antimicrobial Susceptibility Testing (Clinical and LaboratoryStandards Institute, Wayne, PA, 2005).
17. Y. H. Lee, G. Liu, D. M. Thiboutot, D. L. Leslie, J. S. Kirby, A retrospective analysis of theduration of oral antibiotic therapy for the treatment of acne among adolescents:Investigating practice gaps and potential cost-savings. J. Am. Acad. Dermatol. 71, 70–76(2014).
18. D. R. Cranendonk, B. C. Opmeer, J. M. Prins, W. J. Wiersinga, Comparing short to standardduration of antibiotic therapy for patients hospitalized with cellulitis (DANCE): Studyprotocol for a randomized controlled trial. BMC Infect. Dis. 14, 235 (2014).
19. A. Hohn, S. Schroeder, A. Gehrt, K. Bernhardt, B. Bein, K. Wegscheider, M. Hochreiter, Procalcitonin-guided algorithm to reduce length of antibiotic therapy in patients with severe sepsis andseptic shock. BMC Infect. Dis. 13, 158 (2013).
20. A. I. Zumla, S. H. Gillespie, M. Hoelscher, P. P. J. Philips, S. T. Cole, I. Abubakar, T. D. McHugh,M. Schito, M. Maeurer, A. J. Nunn, New antituberculosis drugs, regimens, and adjuncttherapies: Needs, advances, and future prospects. Lancet Infect. Dis. 14, 327–340 (2014).
21. G. Dimopoulos, G. Poulakou, I. A. Pneumatikos, A. Armaganidis, M. H. Kollef, D. K. Matthaiou,Short- vs long-duration antibiotic regimens for ventilator-associated pneumonia: A systematicreview and meta-analysis. Chest 144, 1759–1767 (2013).
22. D. Guillemot, C. Carbon, B. Balkau, P. Geslin, H. Lecoeur, F. Vauzelle-Kervroëdan, G. Bouvenot,E. Eschwége, Low dosage and long treatment duration of b-lactam: Risk factors for carriageof penicillin-resistant Streptococcus pneumoniae. JAMA 279, 365–370 (1998).
23. N. Q. Balaban, J. Merrin, R. Chait, L. Kowalik, S. Leibler, Bacterial persistence as a phenotypicswitch. Science 305, 1622–1625 (2004).
24. N. Q. Balaban, K. Gerdes, K. Lewis, J. D. McKinney, A problem of persistence: Still morequestions than answers? Nat. Rev. Microbiol. 11, 587–591 (2013).
25. N. R. Cohen, M. A. Lobritz, J. J. Collins, Microbial persistence and the road to drugresistance. Cell Host Microbe 13, 632–642 (2013).
26. T. Dörr, K. Lewis, M. Vulić, SOS response induces persistence to fluoroquinolones in Escherichiacoli. PLOS Genet. 5, e1000760 (2009).
27. J. Feng, D. A. Kessler, E. Ben-Jacob, H. Levine, Growth feedback as a basis for persisterbistability. Proc. Natl. Acad. Sci. U.S.A. 111, 544–549 (2014).
28. S. S. Grant, B. B. Kaufmann, N. S. Chand, N. Haseley, D. T. Hung, Eradication of bacterialpersisters with antibiotic-generated hydroxyl radicals. Proc. Natl. Acad. Sci. U.S.A. 109,12147–12152 (2012).
29. P. J. T. Johnson, B. R. Levin, Pharmacodynamics, population dynamics, and the evolution ofpersistence in Staphylococcus aureus. PLOS Genet. 9, e1003123 (2013).
30. G. R. Stewart, B. D. Robertson, D. B. Young, Tuberculosis: A problem with persistence. Nat.Rev. Microbiol. 1, 97–105 (2003).
31. Y. Wakamoto, N. Dhar, R. Chait, K. Schneider, F. Signorino-Gelo, S. Leibler, J. D. McKinney,Dynamic persistence of antibiotic-stressed mycobacteria. Science 339, 91–95 (2013).
32. T. Dörr, M. Vulić, K. Lewis, Ciprofloxacin causes persister formation by inducing the TisBtoxin in Escherichia coli. PLOS Biol. 8, e1000317 (2010).
33. K. Lewis, Persister cells, dormancy and infectious disease. Nat. Rev. Microbiol. 5, 48–56(2007).
34. O. Fridman, A. Goldberg, I. Ronin, N. Shoresh, N. Q. Balaban, Optimization of lag time un-derlies antibiotic tolerance in evolved bacterial populations. Nature 513, 418–421 (2014).
35. J. L. Martínez, F. Baquero, D. I. Andersson, Predicting antibiotic resistance. Nat. Rev. Microbiol. 5,958–965 (2007).
36. P. S. Ocampo, V. Lázár, B. Papp, M. Arnoldini, P. Abel zur Wiesch, R. Busa-Fekete, G. Fekete,C. Pál, M. Ackermann, S. Bonhoeffer, Antagonism between bacteriostatic and bactericidalantibiotics is prevalent. Antimicrob. Agents Chemother. 58, 4573–4582 (2014).
37. M. Scott, C. W. Gunderson, E. M. Mateescu, Z. Zhang, T. Hwa, Interdependence of cellgrowth and gene expression: Origins and consequences. Science 330, 1099–1102 (2010).
nceTranslationalMedicine.org 13 May 2015 Vol 7 Issue 287 287ra73 10

R E S EARCH ART I C L E
by guest on June 7, 2020http://stm
.sciencemag.org/
Dow
nloaded from
38. S. Gudmundsson, S. Einarsson, H. Erlendsdottir, J. Moffat, W. Bayer, W. A. Craig, The post-antibiotic effect of antimicrobial combinations in a neutropenic murine thigh infectionmodel. J. Antimicrob. Chemother. 31 (Suppl. D), 177–191 (1993).
39. M. G. Täuber, O. Zak, W. M. Scheld, B. Hengstler, M. A. Sande, The postantibiotic effect inthe treatment of experimental meningitis caused by Streptococcus pneumoniae in rabbits.J. Infect. Dis. 149, 575–583 (1984).
40. W. A. Craig, Post-antibiotic effects in experimental infection models: Relationship to in-vitrophenomena and to treatment of infections in man. J. Antimicrob. Chemother. 31 (Suppl. D),149–158 (1993).
41. R. R. Regoes, C. Wiuff, R. M. Zappala, K. N. Garner, F. Baquero, B. R. Levin, Pharmacodynamicfunctions: A multiparameter approach to the design of antibiotic treatment regimens.Antimicrob. Agents Chemother. 48, 3670–3676 (2004).
42. S. Bakshi, A. Siryaporn, M. Goulian, J. C. Weisshaar, Superresolution imaging of ribosomesand RNA polymerase in live Escherichia coli cells. Mol. Microbiol. 85, 21–38 (2012).
43. L. Molinengo, The curve doses vs survival time in the evaluation of acute toxicity. J. Pharm.Pharmacol. 31, 343–344 (1979).
44. S. Magnet, J. S. Blanchard, Molecular insights into aminoglycoside action and resistance.Chem. Rev. 105, 477–498 (2005).
45. R. Williamson, R. Hakenbeck, A. Tomasz, In vivo interaction of beta-lactam antibiotics withthe penicillin-binding proteins of Streptococcus pneumoniae. Antimicrob. Agents Chemother.18, 629–637 (1980).
46. H. F. Chambers, M. J. Sachdeva, C. J. Hackbarth, Kinetics of penicillin binding to penicillin-binding proteins of Staphylococcus aureus. Biochem. J. 301 (Pt. 1), 139–144 (1994).
47. T. J. Dougherty, K. Kennedy, R. E. Kessler, M. J. Pucci, Direct quantitation of the number of individualpenicillin-binding proteins per cell in Escherichia coli. J. Bacteriol. 178, 6110–6115 (1996).
48. R. C. Li, Simultaneous pharmacodynamic analysis of the lag and bactericidal phases exhibitedby beta-lactams against Escherichia coli. Antimicrob. Agents Chemother. 40, 2306–2310(1996).
49. N. E. Freed, O. K. Silander, B. Stecher, A. Böhm, W.D. Hardt, M. Ackermann, A simple screen toidentify promoters conferring high levels of phenotypic noise. PLOS Genet. 4, e1000307 (2008).
50. O. K. Silander, N. Nikolic, A. Zaslaver, A. Bren, I. Kikoin, U. Alon, M. Ackermann, A genome-wide analysis of promoter-mediated phenotypic noise in Escherichia coli. PLOS Genet. 8,e1002443 (2012).
51. A. Jindani, C. J. Doré, D. A. Mitchison, Bactericidal and sterilizing activities of antituberculosisdrugs during the first 14 days. Am. J. Respir. Crit. Care Med. 167, 1348–1354 (2003).
52. H. M. Ziglam, Rifampicin concentrations in bronchial mucosa, epithelial lining fluid, alve-olar macrophages and serum following a single 600 mg oral dose in patients undergoingfibre-optic bronchoscopy. J. Antimicrob. Chemother. 50, 1011–1015 (2002).
53. J. J. Wilkins, R. M. Savic, M. O. Karlsson, G. Langdon, H. McIlleron, G. Pillai, P. J. Smith, U. S. Simonsson,Population pharmacokinetics of rifampin in pulmonary tuberculosis patients, including a semi-mechanistic model to describe variable absorption. Antimicrob. Agents Chemother. 52,2138–2148 (2008).
54. D. Shah, Z. Zhang, A. Khodursky, N. Kaldalu, K. Kurg, K. Lewis, Persisters: A distinct phys-iological state of E. coli. BMC Microbiol. 6, 53 (2006).
55. E. Maisonneuve, K. Gerdes, Molecular mechanisms underlying bacterial persisters. Cell 157,539–548 (2014).
56. B. Javid, F. Sorrentino, M. Toosky, W. Zheng, J. T. Pinkham, N. Jain, M. Pan, F. Deighan,E. J. Rubin, Mycobacterial mistranslation is necessary and sufficient for rifampicin phenotypicresistance. Proc. Natl. Acad. Sci. U.S.A. 111, 1132–1137 (2014).
57. G. Manina, N. Dhar, J. D. McKinney, Stress and host immunity amplify Mycobacteriumtuberculosis phenotypic heterogeneity and induce nongrowing metabolically active forms.Cell Host Microbe 17, 32–46 (2015).
58. S. L. Spencer, S. Gaudet, J. G. Albeck, J. M. Burke, P. K. Sorger, Non-genetic origins of cell-to-cellvariability in TRAIL-induced apoptosis. Nature 459, 428–432 (2009).
59. B. R. Levin, D. E. Rozen, Non-inherited antibiotic resistance. Nat. Rev. Microbiol. 4, 556–562(2006).
60. J. K. Patel, C. B. Read, Handbook of the Normal Distribution (Taylor & Francis, London, ed. 2, 1996).61. D. J. C. MacKay, Information Theory, Inference and Learning Algorithms (Cambridge Univ.
Press, Cambridge, 2003).62. S. Chanwong, N. Maneekarn, L. Makonkawkeyoon, S. Makonkawkeyoon, Intracellular
growth and drug susceptibility of Mycobacterium tuberculosis in macrophages. Tuberculosis87, 130–133 (2007).
63. B. Wiseman, X. Carpena, M. Feliz, L. J. Donald, M. Pons, I. Fita, P. C. Loewen, Isonicotinic acidhydrazide conversion to isonicotinyl-NAD by catalase-peroxidases. J. Biol. Chem. 285,26662–26673 (2010).
64. M. Nilsson, L. Bülow, K. G. Wahlund, Use of flow field-flow fractionation for the rapid quan-titation of ribosome and ribosomal subunits in Escherichia coli at different protein produc-tion conditions. Biotechnol. Bioeng. 54, 461–467 (1997).
65. H. Bremer, P. P. Dennis, in In Escherichia coli and Salmonella typhimurium: Cellular andMolecular Biology, F. C. Neidhardt, Ed. (American Society for Microbiology, Washington,DC, 1987), pp. 1553–1569.
www.Scie
66. B. Epe, P. Woolley, The binding of 6-demethylchlortetracycline to 70S, 50S and 30S ribosomalparticles: A quantitative study by fluorescence anisotropy. EMBO J. 3, 121–126 (1984).
67. B. Zakeri, G. D. Wright, Chemical biology of tetracycline antibiotics. Biochem. Cell Biol. 86,124–136 (2008).
68. M. Pioletti, F. Schlünzen, J. Harms, R. Zarivach, M. Glühmann, H. Avila, A. Bashan, H. Bartels,T. Auerbach, C. Jacobi, T. Hartsch, A. Yonath, F. Franceschi, Crystal structures of complexes ofthe small ribosomal subunit with tetracycline, edeine and IF3. EMBO J. 20, 1829–1839 (2001).
69. T. R. Tritton, Ribosome-tetracycline interactions. Biochemistry 16, 4133–4138 (1977).70. F. Tangy, M. Moukkadem, E. Vindimian, M. L. Capmau, F. Le Goffic, Mechanism of action of
gentamicin components. Characteristics of their binding to Escherichia coli ribosomes. Eur.J. Biochem. 147, 381–386 (1985).
71. B. Llano-Sotelo, R. P. Hickerson, L. Lancaster, H. F. Noller, A. S. Mankin, Fluorescentlylabeled ribosomes as a tool for analyzing antibiotic binding. RNA 15, 1597–1604 (2009).
72. F. N. Chang, J. G. Flaks, Binding of dihydrostreptomycin to Escherichia coli ribosomes: Ki-netics of the reaction. Antimicrob. Agents Chemother. 2, 308–319 (1972).
73. D. Lando, M. A. Cousin, T. Ojasoo, J. P. Raymond, Paromomycin and dihydrostreptomycinbinding to Escherichia coli ribosomes. Eur. J. Biochem. 66, 597–606 (1976).
74. B. G. Spratt, Distinct penicillin binding proteins involved in the division, elongation, andshape of Escherichia coli K12. Proc. Natl. Acad. Sci. U.S.A. 72, 2999–3003 (1975).
75. M. Terrak, T. K. Ghosh, J. van Heijenoort, J. Van Beeumen, M. Lampilas, J. Aszodi, J. A. Ayala,J. M. Ghuysen, M. Nguyen-Distèche, The catalytic, glycosyl transferase and acyl transferasemodules of the cell wall peptidoglycan-polymerizing penicillin-binding protein 1b of Escherichiacoli. Mol. Microbiol. 34, 350–364 (1999).
76. T. Maier, A. Schmidt, M. Güell, S. Kühner, A. C. Gavin, R. Aebersold, L. Serrano, Quantifica-tion of mRNA and protein and integration with protein turnover in a bacterium. Mol. Syst.Biol. 7, 511 (2011).
77. J. Malmström, M. Beck, A. Schmidt, V. Lange, E. W. Deutsch, R. Aebersold, Proteome-widecellular protein concentrations of the human pathogen Leptospira interrogans. Nature 460,762–765 (2009).
78. W. Wehrli, Kinetic studies of the interaction between rifampicin and DNA-dependent RNApolymerase of Escherichia coli. Eur. J. Biochem. 80, 325–330 (1977).
79. B. D. Bennett, E. H. Kimball, M. Gao, R. Osterhout, S. J. Van Dien, J. D. Rabinowitz, Absolutemetabolite concentrations and implied enzyme active site occupancy in Escherichia coli.Nat. Chem. Biol. 5, 593–599 (2009).
80. Y. Taniguchi, P. J. Choi, G. W. Li, H. Chen, M. Babu, J. Hearn, A. Emili, X. S. Xie, Quantifying E.coli proteome and transcriptome with single-molecule sensitivity in single cells. Science329, 533–538 (2010).
81. M. Wilming, K. Johnsson, Spontaneous formation of the bioactive form of the tuberculosisdrug isoniazid. Angew. Chem. Int. Ed. Engl. 38, 2588–2590 (1999).
82. R. Rawat, A. Whitty, P. J. Tonge, The isoniazid-NAD adduct is a slow, tight-binding inhibitorof InhA, the Mycobacterium tuberculosis enoyl reductase: Adduct affinity and drugresistance. Proc. Natl. Acad. Sci. U.S.A. 100, 13881–13886 (2003).
Acknowledgments: Wewould like to acknowledge A. Jindani, R. Regoes, and S. Bakshi for providingpreviously published raw data. We are grateful toM. Lipsitch, S. Hatzios, and T. Dörr for critical readingand helpful comments. Funding: This work was supported by Swiss National Science Foundation(www.snf.ch) grant PBEZP3_140163 and German Academic Exchange Service (www.daad.org) grantD/11/45747 (P.A.z.W.), NIH U54GM088558 from the National Institute of General Medical Sciences andNIH DP2OD006663 from the Office of the Director (T.C.), Bill & Melinda Gates Foundation grantOPP1111658 (T.C. and P.A.z.W.), Swiss Foundation for Grants in Biology and Medicine (www.samw.ch) grant PASMP3_142724/1 (S.A.), NIH R37 AI-042347 from the National Institute of Allergy and Infec-tious Diseases and Howard Hughes Medical Institute (M.K.W.), Deutsche Forschungsgemeinschaftgrant MA 5320/1-1 (C.M.), and Swedish Research Council junior investigator grant 621-2012-3564(K.U.). The content is solely the responsibility of the authors and does not necessarily represent theofficial views of the National Institute of General Medical Sciences or the Office of the Director of theNIH. The funders had no role in study design, data collection and analysis, decision to publish, orpreparation of the manuscript. Author contributions: P.A.z.W. conceived the idea and developedthe mathematical modeling framework; P.A.z.W., S.A., and K.U. designed experiments; S.A., S.G.,and P.O. performed the experiments; J.E. and T.H. extended the modeling framework; C.M. andP.A.z.W. derived analytical solutions; P.A.z.W., S.A., K.U., and T.C. interpreted the results; P.A.z.W.,S.A., M.K.W., and T.C. wrote the manuscript; T.C., M.K.W., and K.U. contributed material.Competing interests: The authors declare that they have no competing interests.
Submitted 7 February 2015Accepted 13 March 2015Published 13 May 201510.1126/scitranslmed.aaa8760
Citation: P. Abel zur Wiesch, S. Abel, S. Gkotzis, P. Ocampo, J. Engelstädter, T. Hinkley,C. Magnus, M. K. Waldor, K. Udekwu, T. Cohen, Classic reaction kinetics can explain complexpatterns of antibiotic action. Sci. Transl. Med. 7, 287ra73 (2015).
nceTranslationalMedicine.org 13 May 2015 Vol 7 Issue 287 287ra73 11

Classic reaction kinetics can explain complex patterns of antibiotic action
Matthew K. Waldor, Klas Udekwu and Ted CohenPia Abel zur Wiesch, Sören Abel, Spyridon Gkotzis, Paolo Ocampo, Jan Engelstädter, Trevor Hinkley, Carsten Magnus,
DOI: 10.1126/scitranslmed.aaa8760, 287ra73287ra73.7Sci Transl Med
design of antibiotic treatment strategies.experimentally and with data from a tuberculosis clinical trial. This model may help optimize dosing and aid rationalmodel that links chemical reaction kinetics to bacterial population biology and validate this model both growth suppression, density-dependent antibiotic effects, and persister cell formation. They report a theoreticalkinetics can explain three effects of antibiotics previously considered to have different causes: post-antibiotic
now report that simple chemical bindinget al.leading to development of drug-resistant bacteria. Abel zur Wiesch Antibiotics are powerful tools in fighting bacterial infection, but overuse and misuse are taking their tolls,
Antibiotics, pure and simple
ARTICLE TOOLS http://stm.sciencemag.org/content/7/287/287ra73
MATERIALSSUPPLEMENTARY http://stm.sciencemag.org/content/suppl/2015/05/11/7.287.287ra73.DC1
CONTENTRELATED
http://science.sciencemag.org/content/sci/367/6474/200.fullhttp://science.sciencemag.org/content/sci/367/6474/141.fullhttp://science.sciencemag.org/content/sci/360/6387/387.1.fullhttp://science.sciencemag.org/content/sci/357/6354/879.fullhttp://science.sciencemag.org/content/sci/348/6239/1106.fullhttp://stm.sciencemag.org/content/scitransmed/5/180/180ra49.fullhttp://stm.sciencemag.org/content/scitransmed/5/192/192ra85.full
REFERENCES
http://stm.sciencemag.org/content/7/287/287ra73#BIBLThis article cites 78 articles, 24 of which you can access for free
PERMISSIONS http://www.sciencemag.org/help/reprints-and-permissions
Terms of ServiceUse of this article is subject to the
registered trademark of AAAS. is aScience Translational MedicineScience, 1200 New York Avenue NW, Washington, DC 20005. The title
(ISSN 1946-6242) is published by the American Association for the Advancement ofScience Translational Medicine
Copyright © 2015, American Association for the Advancement of Science
by guest on June 7, 2020http://stm
.sciencemag.org/
Dow
nloaded from