CENTRE HEPATO-BILIAIRE HÔPITAL PAUL BROUSSE VILLEJUIF · CENTRE HEPATO-BILIAIRE HÔPITAL PAUL...
22
HIV and HBV/HCV coinfection and liver transplantation: Results Jean-Charles Duclos-Vallée CENTRE HEPATO-BILIAIRE HÔPITAL PAUL BROUSSE VILLEJUIF
Transcript of CENTRE HEPATO-BILIAIRE HÔPITAL PAUL BROUSSE VILLEJUIF · CENTRE HEPATO-BILIAIRE HÔPITAL PAUL...
-
HIV and HBV/HCV coinfectionand liver transplantation:
ResultsJean-Charles Duclos-Vallée
CENTRE HEPATO-BILIAIREHÔPITAL PAUL BROUSSE
VILLEJUIF
-
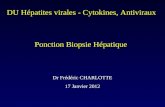
HIV Coinfection Shortens the Survival of Patients with HCV Decompensated Cirrhosis
MedianMedian survivalsurvival = 16 = 16 monthsmonths
Pineda et al. Pineda et al. HepatologyHepatology 20052005
Surv
ival
Surv
ival
prob
abili
typr
obab
ility
335511111919303046467575180180HIV positiveHIV positive
99626213313320820831331342942961961910371037HIV HIV negativenegative
NN°° atat riskrisk
ProbabilityProbability ofof patient patient survivalsurvivalaccordingaccording to HIV to HIV serostatusserostatus
44%44%61%61%74%74%HIVHIV--
25%25%40%40%54%54%HIV+HIV+
55--yearyear22--yearyear11--yearyearSurvivalSurvival
0 10 20 30 40 50 60 700.0
0.2
0.4
0.6
0.8
1.0
HIV negative
HIV positive
Months
-
Liver Transplantation in Adults Coinfected with HIV under HAART
Preliminary ExperiencePrachalias et al. Transplantation 2001
Liver Transplantation in Adults Coinfected with HIV under HAART
Preliminary ExperiencePrachalias et al. Transplantation 2001
Alive(4 months)
NANB5
Alive(24 months)
HBV4
Died (6 months)
HCV3
Died(15 months)
HCV2
Died (25 months)
HCV1
OutcomePost LT
DiagnosisPatients
-
LIVER TRANSPLANTATION IN HIV-HCV PATIENTSPittsburgh and Miami (1997-2001)
AliveNov 200115AliveOct 200114AliveJan 200113AliveOct 200012
CR/HCV Died (570 days)Mar199910
Acute CRDied (12 days)Jan 19999AliveDec 19988AliveSept 19977AliveMay 20016
CauseOutcomeOLT datePatient
Neff et al. Liver Transpl 2003
-
LIVER TRANSPLANTATION IN HIV-HBV PATIENTSPittsburgh and Miami (1997-2001)
AliveNov 200115AliveOct 200114AliveJan 200113AliveOct 200012
CR/HCV Died (570 days)Mar199910
Acute CRDied (12 days)Jan 19999AliveDec 19988AliveSept 19977AliveMay 20016
CauseOutcomeOLT datePatient
Neff et al. Liver Transpl 2003
-
PRETRANSPLANT INCLUSION AND EXCLUSION CRITERIA
Inclusion:
HIV viral load -Limited or no opportunistic
complicationsCD4+ > 250/mL for the past 6 monthsHistory of compliance with medical
protocol
Exclusion:
Ongoing opportunistic infection or cancer
History of any neoplasm except hepatocellular carcinoma
-
Paul Brousse ExperienceNovember 2000 - October 2005
Paul Brousse ExperienceNovember 2000 - October 2005
n = 41patients transplanted
HBV Cirrhosis n=6
(Delta coinfection: n=2)(HCC: n=1)
HCV Cirrhosis
n=34(HCC: n=3)
Fulminant Hepatitis: n=1
-
8 patients died
HCV recurrence and mitochondrial toxicity: n=5Acute pancreatitis: n=1
Pancreatic adenocarcinoma: n=1Cerebral hemorrhage: n=1
Paul Brousse ExperienceNovember 2000 - October 2005
Paul Brousse ExperienceNovember 2000 - October 2005
n = 41patients transplanted
-
0
1
2
3
4
5
6
7
8
9
D0 D15 M1 M3 M6 M12 M18 M24 M36
post LT
HCV RNA log10
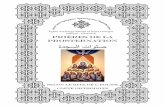
HCV viral recurrenceHCV viral load
HCV viral recurrenceHCV viral load
5,6
5,8
6
6,2
6,4
6,6
6,8
Viral load at 6 months
6. 8 ± 0.4
6. 0 ± 1
P=0.03
Co-infectedMonoinfected
-
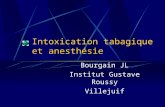
HCV viral recurrenceSeverity of fibrosisJanuary 1999 - June 2004
n= 23 HIV/HCV +
HCV viral recurrenceSeverity of fibrosisJanuary 1999 - June 2004
n= 23 HIV/HCV +
0
5
10
15
20
25
30
35
F=3
%
5/2322%
3/2313%
F=4
Rate of Fibrosis between M12 and M16= Time from LT/Metavir F
0
0,20,4
0,60,8
1
1,2
1,4
1,6
Coinfected(n=23)
Monoinfected (n=44)
1.5 ±1.4
0.8 ± 0.5
P=0.03
M4, M6, M16,M20, M21Post LT
M24, M24,M18
Post LT
Fibrosing cholestasis Hepatitis n=1
M24Post LT
-
HCV viral recurrenceEffect of Antiviral TherapyHCV viral recurrence
Effect of Antiviral Therapy
10/14 (71%)3/13 (23%)Virological response
14/44 (32 %)13/22 (59 %)Pegylated interferon a 2-b + ribavirin
Monoinfected patients
Co-infected patients
-
Secondary effect of anti-HCV therapy
Anti Anti HCV HCV therapy wastherapy wasstopped stopped in 5 patientsin 5 patients
•• Pancreatitis Pancreatitis : n = 1: n = 1•• Lethal lactic acidosis Lethal lactic acidosis : n = 1: n = 1
•• Intense Intense Asthenia Asthenia : n = 3: n = 3
13/22 (59%) treated
-
Mitochondrial toxicityMicrovesicular steatosis
Microvesicular steatosis range (10%-50%)
observed in 8/19 (42%) patients
-
Mitochondrial toxicityComparison of Liver mtDNA
in HIV+/HCV+ Patients and HIV Negative Controls
Mitochondrial toxicityComparison of Liver mtDNA
in HIV+/HCV+ Patients and HIV Negative Controls
Liver mt DNA (copies number/ng total DNA)
Patients
19 5235(203207-611111)
p=0.01
HIV-/HCV+(1 year post LT)
(n=8)
26 511 (5817-143010)
HIV+/HCV+ (n=5)
Duclos-Vallee J Hepatol 2005
IV complexActivity
0
-
CD4 Count and HIV viral load During the Post-LT Course
n=7
Cells/mm3
0
200
400
600
800
1000
1200
0 5 10 15 20
Log 10
0
1
2
3
4
5
6
7
0 5 10 15 20months
-
Bacterial and opportunistic infections
Bacterial and opportunistic infections
Coinfected Patients
3/23(13%)
p=0.03
Monoinfected Patients
16/44(36%)
Bacterial infection
Coinfected Patients
Oesophagal candidosis:
n=1
Monoinfected Patients
P. Carinii: n=2Syst.
Candidosis: n=2
Opportunistic infections
-
Drug InteractionIn HIV Liver Transplant Patients
Teicher et al. Submitted
0
100
200
300
400
500
600
Alone + ARV
NUCLPVLPVLPVLPVEFVEFV
Tacr
olim
us o
ral c
lear
ance
-ml/m
in
+ LPV/RTV ⇒ Tacrolimus
0.5mg / 10 or 15 days
-
Figure 1A
0
0.2
0.4
0.6
0.8
1
0 1 2 3 4 5
HIV-HCV+
HIV+HCV+
Survival analysisSurvival analysis
2-year survival:`
HIV+/HCV (n=23): 72%HIV-/HCV (n=44): 92%Log rank p=0.07
-
1.0
0.8
0.6
0.4
0.2
0.0
0 6 12 18 24 30 36 48 60
HCV+/HIV-/OLTXHCV+/HIV+/OLTX
p = 0.06
57%
80%
Months since OLTX
Prop
ortio
n su
rviv
ing
Survival of Transplanted Monoinfected HCV (4062 Unos) and Coinfected HCV-HIV (15)
RagniRagni M et al, J Infect Dis, 2003;188:1412M et al, J Infect Dis, 2003;188:1412––2020
-
Liver Transplantation In HIV-HBV Patientsn=5
HBIg+Lam+Tenof.
HBIg+Lam+Tenof.
HBIg+Lam+Tenof.
HBIg+Lam+Tenof.
HBIg+Lam+Tenof.Post LT HBV therapy
WellM12GREY.
WellM12MONG.
WellM24BON.
WellM31MAH.
WellM36ALE.Clinical status Follow-up Patients
-
ConclusionsConclusions
• Feasible• HBV-HIV: Excellent• HCV-HIV: Difficult
– Mitochondrial toxicity»Avoid DDI, D4T, AZT»Change HAART if microvesicular steatosis
– HCV recurence»Early Antiviral therapy
-
A Multidisciplinary Approach A Multidisciplinary Approach
Centre Hépato-Biliaire
D CastaingD SamuelR Adam
D AzoulayC FerayF SalibaP Ichai
B RocheT AntoniniM GigouC Danet
E PasdeloupC Tanguy
G BerthelotNurses …
Virology UnitAM Roque-Afonso
V MackiewiczE Dussaix
Pathology UnitM SebaghMP BraletC Guettier
Department of Infectious DiseasesE Teicher
D Vittecoq
Biochemistry UnitC Jardel
A Lombès
Department of AnesthesiologyC JosseA Mirand
MC Gillon