Cas$clinique$de$cancer$du$colon$ métastaque$:$ … · sigmoïde$ • Histoire$de$lamaladie$ –...
49
Cas clinique de cancer du colon métasta2que : RCP en temps réel K. Bentabak (1), M. Oukkal (2), SA. Faraoun (3) 1. Service de Chirurgie Oncologique, CPMC, Alger 2. Service d’Oncologie Médicale, COMAZ, Alger 3. Service d’Imagerie Médicale, CPMC, Alger Cours Intensif de Cancérologie Diges2ve FFCDSAHGEED Alger, les 16 et 17 Septembre 2016
Transcript of Cas$clinique$de$cancer$du$colon$ métastaque$:$ … · sigmoïde$ • Histoire$de$lamaladie$ –...

Cas clinique de cancer du colon métasta2que : RCP en temps réel
K. Bentabak (1), M. Oukkal (2), SA. Faraoun (3)
1. Service de Chirurgie Oncologique, CPMC, Alger 2. Service d’Oncologie Médicale, COMAZ, Alger 3. Service d’Imagerie Médicale, CPMC, Alger
Cours Intensif de Cancérologie Diges2ve FFCD-‐SAHGEED
Alger, les 16 et 17 Septembre 2016

• Mr T.M., âgé de 69 ans (64 kg / 175 cm), hypertendu, adressé (12/12/13) pour métastases hépa2ques synchrones d’un adénocarcinome du sigmoïde
• Histoire de la maladie – Douleur de l’HCDt depuis 6 mois – Pas de troubles du transit
• Echographie et TDM abdominal (14/11/13)
– Foie siège de 3 volumineux nodules au niveau du lobe droit
• PBF écho-‐guidée (25/11/13) – Métastases hépa2ques d’un adénocarcinome d’origine colique
• Coloscopie (08/12/13) – Processus tumoral ulcéro-‐bourgeonnant du sigmoïde non sténosant
• An2gène carino-‐embryonnaire = 533 ng/ml

Bilan d’extension Scan TAP (16/12/13)
• Foie – Mul2ples lésions nodulaires sur le lobe droit dont les plus volumineuses
– Segment VIII et IV de 96 mm, segment VII – Segment V et VI de 117 mm
– Pas de nodules sur les segments I, II et III
• Colon gauche – Epaississement bourgeonnant hémi circonféren2el de 34x18 mm – Ganglions dans le méso colon
• Pas de carcinose péritonéale
• Thorax sans lésions secondaires


Q1: Comment classez-‐vous les métastases hépa2ques?
1. Résécables
2. Poten2ellement résécables
3. Non résécables

R1: Comment classez-‐vous les métastases hépa2ques?
1. Résécables
2. Poten2ellement résécables
3. Non résécables

Comment définir la résécabilité?
Possibilité de réséquer l’ensemble des lésions (résec2on R0) tout en laissant un parenchyme hépa2que bien vascularisé (in flow et out flow) et suffisant en volume



Q2: Quelle traitement préconisez-‐vous pour ce pa2ent?
1. Chimiothérapie pallia2ve d’emblée car vous considérez les métastases hépa2ques comme jamais résécables sachant que la tumeur primi2ve est asymptoma2que
2. Chimiothérapie associée à une thérapie ciblée d’emblée avec pour objec2f de rendre résécable les lésions hépa2ques
3. Chirurgie de la tumeur primi2ve pour prévenir une complica2on éventuelle suivie d’une chimiothérapie pallia2ve
4. Chirurgie de la tumeur primi2ve pour prévenir une complica2on éventuelle suivie d’une chimiothérapie associée à une thérapie ciblée pour tenter de rendre résécables les lésions hépa2ques

R2: Quelle traitement préconisez-‐vous pour ce pa2ent?
1. Chimiothérapie pallia2ve d’emblée car vous considérez les métastases hépa2ques comme jamais résécables sachant que la tumeur primi2ve est asymptoma2que
2. Chimiothérapie associée à une thérapie ciblée d’emblée avec pour objec2f de rendre résécable les lésions hépa2ques
3. Chirurgie de la tumeur primi2ve pour prévenir une complica2on éventuelle suivie d’une chimiothérapie pallia2ve
4. Chirurgie de la tumeur primi2ve pour prévenir une complica2on éventuelle suivie d’une chimiothérapie associée à une thérapie ciblée pour tenter de rendre résécables les lésions hépa2ques

Survie à long terme des métastases hépa2ques rendues résécables après chimiothérapie néoadjuvante
Adam R. & al. Ann Surg. 2004; 4: 644-‐658

MHS non résécables avec CCR asymptoma2que
Etude US (Memorial, NY)
• 233 pts, 2000-‐2006 • 207 pts (89%)
– Pas de chirurgie du primi2f • Survie médiane de 18 mois • 16 pts (7%)
– Chirurgie en urgence • 47 pts (20%)
– Chirurgie des métastases – Survie médiane 44 mois
â Résultats très en faveur de la chimiothérapie première
Poultsides GA et al. JCO 2009; 27: 3379-‐84

• 20 pa2ents dont 11 cancers rectaux – 16 pa2ents opérés
• 8/11 cancers du rectum avec RT-‐CT après la la chirurgie hépa2que
– 1 récidive locale • Survie actuarielle des pa2ents réséqués
– 100% à 1 an et 89% à 3 ans
• Survie actuarielle de tous les pa2ents – 89% à 1 an et 71% à 3 ans
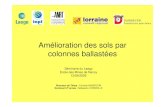
Stratégie REVERSE: Chimiothérapie à Résec2on hépa2que à Résec2on du primi2f

787 pa2ents 2000-‐2010
729 pa2ents Stratégie classique Nbre moy MH = 4,8
Traitement complet 30% Survie globale à 5 ans = 46%
Survie sans récidive à 5 ans = 26%
58 pa2ents Stratégie reverse
Nbre moy MH = 4,2
Traitement complet 80% Survie globale à 5 ans = 48%
Survie sans récidive à 5 ans = 30%
ORIGINAL ARTICLES FROM THE ESA PROCEEDINGS
A Survival Analysis of the Liver-First Reversed Managementof Advanced Simultaneous Colorectal Liver Metastases
A LiverMetSurvey-Based Study
Axel Andres, MD,∗ Christian Toso, MD, PhD,∗ Rene Adam, MD, PhD,† Eduardo Barroso, MD,‡Catherine Hubert, MD,§ Lorenzo Capussotti, MD,|| Eric Gerstel, MD,∗ Arnaud Roth, MD,∗ Pietro E. Majno, MD,∗
and Gilles Mentha, MD∗
Background: Liver-first reversed management (RM) for the treatment of pa-tients with simultaneous colorectal liver metastases (CRLM) includes liver-directed chemotherapy, the resection of the CRLM, and the subsequent re-section of the primary cancer. Retrospective data have shown that up to 80%of patients can successfully undergo a complete RM, whereas less than 30%of those undergoing classical management (CM) do so. This registry-basedstudy compared the 2 approaches.Methods: The study was based on the LiverMetSurvey (January 1, 2000 toDecember 31, 2010) and included patients with 2 or more metastases. Allpatients had irinotecan and/or oxaliplatin-based chemotherapy before liversurgery. Patients undergoing simultaneous liver and colorectal surgery wereexcluded.Results: A total of 787 patients were included: 729 in the CM group and 58in the RM group. Patients in the 2 groups had similar numbers of metastases(4.20 vs 4.80 for RM and CM, P = 0.231) and Fong scores of 3 or more (79%vs 87%, P = 0.164). Rectal cancer, neoadjuvant rectal radiotherapy, and theuse of combined irinotecan/oxaliplatin chemotherapy were more frequent inthe RM group (P < 0.001), whereas colorectal lymph node involvement wasmore frequent in the CM group (P < 0.001). Overall survival and disease-freesurvival were similar in the RM and CM groups (48% vs 46% at 5 years, P =0.965 and 30% vs 26%, P = 0.992).Conclusions: Classical and reversed managements of metastatic liver diseasein colorectal cancer are associated with similar survival when successfullycompleted.
Keywords: colorectal cancer, colorectal surgery, reversed management,simultaneous liver metastases
(Ann Surg 2012;256: 772–779)
C olorectal cancer (CRC) is the third most common malignanttumor in the Western world and accounts for 10% of all cancer
From the ∗Abdominal and Transplantation Surgery, Geneva University Hospi-tal, Geneva, Switzerland; †AP-HP Hopital Paul Brousse, Centre Hepato-Biliaire, Villejuif, France; ‡Centro Hepato-bilio-pancreatico e de Transplan-tacao do Hospital de Curry Cabral, Lisboa, Portugal; §Department of Abdom-inal Surgery and Transplantation, Division of Hepato-Biliary and PancreaticSurgery, Cliniques Universitaires Saint-Luc, Universite catholique de Louvain,Brussels, Belgium; and ||Department of Hepatopancreatobiliary and DigestiveSurgery, Ospedale Mauriziano Umberto I, Turin, Italy.
LiverMetSurvey is supported by an unrestricted grant from Sanofi-Aventis.C.T. was supported by the Swiss National Science Foundation (SCORE grant
3232230-126233).None of the authors declare any conflict of interest.Disclosure: The authors declare that they have nothing to disclose.Reprints: Gilles Mentha, MD, Transplantation Unit, Geneva University Hospital,
Rue Gabrielle-Perret-Gentil 4, 1211 Geneve 14, Geneva, Switzerland. E-mail:[email protected].
Copyright C⃝ 2012 by Lippincott Williams & WilkinsISSN: 0003-4932/12/25605-0772DOI: 10.1097/SLA.0b013e3182734423
deaths. Approximately 25% of patients with CRC present with livermetastases at the time of primary diagnosis.
Complete surgical removal of all colorectal liver metastaseshas been shown to carry a survival advantage over chemotherapyalone.1 Until recently, classical treatment included resection of theprimary tumor, followed by chemotherapy. Metastases were subse-quently removed, pending an appropriate response to chemotherapy(absence of progression and appropriate downstaging in previouslynonresectable lesions). Unfortunately, this treatment may take manymonths, and some patients progress beyond liver resectability beforereaching liver surgery. In addition, complications of the managementof the primary tumor may prevent chemotherapy, for example, inrectal cancer, only half of the patients complete chemotherapy aftersurgery for the primary tumor.2
Sequential liver and colorectal surgery may be better than acombined procedure, with lower risks of recurrence3 and similarrates of side effects,4,5 particularly in high-morbidity patients withmultiple advanced simultaneous colorectal cancer liver metastases(CRLM).6
In 2006, this group published the “reversed” strategy, begin-ning with a liver-directed neoadjuvant chemotherapy, followed by theresection of all CRLM and finally treatment of the primary cancer.6–8
The survival of patients undergoing this management is promising,but these results were based on a retrospective analysis, comparedonly with historical series.9 The aim of this study was to comparesurvival after reversed versus classical treatment of patients with ad-vanced simultaneous CRLM, using the LiverMetSurvey registry.
PATIENTS AND METHODSThe aim of this LiverMetSurvey-based study was to assess
survival in patients with advanced synchronous CRLM undergoingtreatment by reversed and classical management.10 The LiverMet-Survey is a prospective international registry of patients undergoingsurgery for CRLM. Data are entered prospectively according to anonline standardized questionnaire in 219 centers from 59 countries.Centers that registered the majority of the patients (≥10 per cen-ter) for this study were Hopital Paul Brousse-Centre hepatobiliaire,Paris, France (102 patients), Centro Hepato-bilio-pancreatico e deTransplantacao do Hospital de Curry Cabral, Lisbon, Portugal (64),UCL St Luc, Brussels, Belgium (53), Ospedale Mauriziano UmbertoI, Turin, Italy (41), Hospital Saint-Andre, Bordeaux, France (39),Catholic University-School of Medicine, Rome, Italy (26), HospitalJosep Trueta, Girona, Spain (26), Hospital de Fuenlabrada, Madrid,Spain (20), University Hospitals of Geneva, Geneva, Switzerland(20), Institut Gustave Roussy, Cancer Center, Villejuif, France (18),Essen University Hospital, Essen, Germany (17), Transplantation andLiver Surgery, Helsinki University Hospital, Helsinki, Finland (17),National Research Center of Surgery, Moscow, Russia (14), UO diChirurgia Epato-Biliare, Milano, Italy (13), CHUQ-Hotel Dieu deQuebec, Quebec, Canada (12), Erasmus Medical Center, Rotterdam,
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
772 | www.annalsofsurgery.com Annals of Surgery ! Volume 256, Number 5, November 2012
P=0.965 P=0.992
Andres et al Annals of Surgery ! Volume 256, Number 5, November 2012
FIGURE 2. Kaplan-Meier survival curves depending on reversed or classical treatment groups. A, Overall survival after CRLMdiagnosis, P = 0.960. B, Overall survival after the last operation, P = 0.965. C, Disease-free survival after CRLM diagnosis, P =0.992. D, Disease-free survival after the last operation, P = 0.839.
has been developed to avoid CRLM progression beyond resectabilityduring the management of the primary cancer, one might expect asignificant improvement in intention-to-treat survival after reversedtreatment. A Dutch study reported completion of reversed treatmentin 16 of 22 patients with rectal cancer, which is higher than the ratesreported in classical management.24–26
In this registry-based study, OS and DFS were similar be-tween reversed and classical treatments in patients successfully com-pleting all treatment steps. Of note, the real benefit of the reversedtreatment is its expected ability to offer a complete curative treatmentof patients who could progress beyond resectability during lengthyclassical management. This study cannot address this hypothesis,which would require a large prospective randomized study. Becausethe resection of the CRLM is one of the most frequent indications forliver resection in the West, we believe that it is now appropriate toperform such a trial.
ACKNOWLEDGMENTSThe authors thank Valerie Delvart and all 250 centers from 52
countries that contributed to LiverMetSurvey: Graeme Poston, Uni-
versity Hospital Aintree, United Kingdom; Darius F Mirza, Birming-ham Queen Elizabeth, United Kingdom; Gennaro Nuzzo, CatholicUniversity, School of Medicine, Italy; Jnm Ijzermans, Erasmus Med-ical Center, the Netherlands; Theo Ruers, University Medical CentreSt Radboud, the Netherlands; Lorenzo Capussotti, Ospedale Maur-iziano Umberto I, Italy; Jean-Francois Ouellet, Chuq-Hotel Dieu DeQuebec, Canada; Christophe Laurent, Hopital Saint-Andre, France;Esteban Cugat, Hospital Mutua De Terrassa, Spain; Pierre Em-manuel Colombo, CRLC Val d’Aurelle, France; Miroslav Milice-vic, HPB and Liver Transplant Center, First Surgical Clinic, Clin-ical Center of Serbia, Serbia; Mauro Salizzoni, Chirurgia Generale,Centro Trapianti Di Fegato, Ospedale Molinette Torino, Italy; OlegSkipenko, National Research Center of Surgery, Russia; SantiagoLopezben, Hospital Josep Trueta, Spain; Javier Herrera, NavarraHospital, Spain; Irinel Popescu, Center of General Surgery and LiverTransplantation, Fundeni Clinical Institute, Romania; Irinel Popescu,National Cancer Institute of Brazil, Brazil; Elie Housseau, Hopi-tal De Hautepierre, France; Lloyd Mckie, Mater Hospital, UnitedKingdom; Thomas Gruenberger, Medical University of Vienna, Aus-tria; Francisco Garcia Borobia, Consorci Hospitalari Parc Tauli,
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
776 | www.annalsofsurgery.com C⃝ 2012 Lippincott Williams & Wilkins
Annals of Surgery ! Volume 256, Number 5, November 2012 Simultaneous Colorectal Liver Metastases
Netherlands (12), Chirurgia Generale-Centro Trapianti di fegato-Ospedale Molinette Torino, Turin, Italy (11), Clinica Universitariade Navarra, Pamplona, Spain (11), Departement de Chirurgie diges-tive et de l’Urgence de Grenoble (11), Medical University Vienna,Vienna, Austria (11), Servico Cirurgia III-HUC, Coimbra, Portugal(11), and Navarra Hospital, Pamplona, Spain (10). Data included vari-ables related to patient demographics, primary tumor characteristicsand management, CRLM number, size, location and managementtime and nature of recurrence, and survival.
DefinitionsReversed treatment was defined as a sequential management,
including CRLM-directed chemotherapy, the resection of all CRLM,and the subsequent resection of the primary CRC (with or withoutneoadjuvant radiotherapy for rectal cancer).
Classical treatment was defined as sequential management,including resection of the primary CRC (with or without neoadjuvantradiotherapy for rectal cancer), CRLM-directed chemotherapy, andsubsequent resection of all CRLM.
As a reversed management can be performed only in patientspresenting with synchronous liver metastases, the maximum timebetween CRLM and primary CRC diagnoses was defined as 30 daysor less.
Survival (overall survival [OS] or recurrence, for disease-freesurvival [DFS]) was assessed from the time of CRLM diagnosisand from the last surgical procedure. Procedures performed for thetreatment of recurrences were not taken into account.
Inclusion criteria were as follows: first CRLM resection be-tween January 1, 2000 and December 31, 2010, synchronous CRLM(diagnosed <30 days from the CRC diagnosis), 2 or more CRLM(2 metastases if only 2 liver lobes involved), oxaliplatin and/oririnotecan-based neoadjuvant chemotherapy before liver surgery (ir-respective of duration and number of cycles of chemotherapy), delaybetween hepatectomy and colorectal resection more than 10 days, andR0 resection of both CRLM and primary CRC.
Exclusion criteria were as follows: simultaneous combinedCRLM and colorectal resection (including the combination of col-orectal surgery with the first stage of a 2-stage liver resection) andpatients in whom there were missing diagnoses or surgery dates,either for CRLM or for the primary cancer.
Study Design and Statistical AnalysisPatients were grouped according to reversed and classical man-
agement as defined previously. Patient, CRLM, and primary CRCcharacteristics were compared between groups. The time between thevarious steps of each management and overall duration of treatmentwere assessed and compared. X2 and Student t tests were used forcategorical and continuous variables. DFS and OS were assessed us-ing Kaplan-Meier analysis. Modification of groups’ survivals wereassessed using a Cox regression model.
To assess the effect of the classical versus reversed manage-ment on survival, propensity score was used to adjust for confoundingand selection bias. The probability of reversed management groupwas estimated using a logistic regression model with the follow-ing variables: sex, age, primary location, precolectomy radiotherapy,chemotherapy regimen, T stage of the primary, primary lymph nodestatus, CEA (>200 or <200), CRLM localization, number of metas-tases, date of diagnosis of CRLM, and Fong score. The Fong ClinicalRisk Score represents the sum of 5 items, each equivalent to 1 point:CEA more than 200, more than 1 metastases, delay between colec-tomy and diagnosis of CRLM less than 12 months, positive primarylymph nodes, and size of the largest metastasis greater than 5 cm.9
An adjusted hazard ratio (HR) of the event (death or recur-rence) was obtained with a multivariate Cox regression model, in-
cluding propensity score and group allocation. To assess the impactof each variable on OS and DFS, we performed a cross match of eachvariable and applied the result in a Cox regression for both OS andDFS. The assumption of proportionality of the hazards was checkedwith Schoenfeld residuals. A standard P value of 0.05 was consideredfor significance. Data were reported as mean ± standard deviation. Ana posteriori power analysis was performed to determine the ability todetect the superiority of one treatment group to the other. Univariateand multivariate Cox regression statistical analyses were performedwith SPSS 17.0 (IBM Corporation, New York, NY). The propensityscore matching and the power calculation were performed with Stata10.1 (StataCorp, College station, TX).
RESULTSDemographics
At the time of the study, the LiverMetSurvey registry included13,562 patients between January 1, 1974 and December 31, 2010.Seven hundred eighty-seven of these 787 fulfilled the inclusion cri-teria, 58 with a reversed management and 729 with a classical man-agement (Fig. 1).
Both groups were similar with regard to age and sex (Table 1).In addition, CRLM characteristics were similar with regard to num-ber, size, CEA concentration, and Fong score. The survival of patientspresenting with 2 versus more than 2 metastases was analyzed sepa-rately. OS and DFS between the reversed and classical managementgroups were similar for patients with 2 and more than 2 metastases(data not shown, P = NS).
There were more rectal cancers and treatment with neoadju-vant radiotherapy in the reversed treatment group. Conversely, morepatients had colorectal lymph node metastases in the classical group.
Oxaliplatin-based chemotherapy was the most frequent reg-imen in both groups, but the combination of both oxaliplatin andirinotecan was more frequent in the reversed group.
No difference in the overall duration of treatment was found be-tween groups, although differences between the groups were presentwith respect to individual components of treatment (Table 2).
SurvivalsOS was similar in both reversed and classical groups, regard-
less of whether it was calculated from the time of diagnosis (reversedgroup: 98%, 91%, 76%, 62%, and 42%; classical group: 98%, 91%,77%, 64%, and 55% at 1, 2, 3, 4, and 5 years, P = 0.960, Fig. 2A)or from last surgery (reversed group: 91%, 72%, 68%, 48%, and48%; classical group: 92%, 78%, 65%, 54%, and 46%, P = 0.965,Fig. 2B).
DFS was also similar in both groups from the time of diagnosis(reversed group: 88%, 58%, 49%, 30%, and 30%; classical group:91%, 57%, 41%, 34%, and 29%, P = 992, Fig. 2C) and from lastsurgery (reversed group: 68%, 46%, 30%, 30%, and 30%; classicalgroup: 59%, 41%, 33%, 28%, and 26%, P = 839, Fig. 2D).
The crude and adjusted HRs of death (OS) and recurrence(DFS) for the reversed management group compared with classicalmanagement group are presented in Table 4. The adjusted HR of deathwas lower in the reversed management group for survival calculatedfrom both CRLM diagnosis and last operation, suggesting a survivaladvantage over the classical management group (P = NS). The HR ofrecurrence was similar between both groups (reversed/classical): 1.01for DFS from CRLM diagnosis and 0.99 for DFS from last operation.
Survival was not altered by the patient, CRLM, and CRC char-acteristics listed in Tables 1 and 2, as assessed by a cross match test.No significant influence on survival was found with respect to typeof management (reversed or classical), location of primary tumor
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C⃝ 2012 Lippincott Williams & Wilkins www.annalsofsurgery.com | 773

Ann Surg 2012;255:237–247
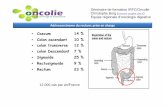
Sans traitement à 70%-‐90% des pa2ents sont non résécables Objec2f à Augmenter le taux de réponse

Plus la ligne de chimiothérapie est efficace, meilleurs sont les résultats de la chirurgie
Études incluant des pa2ents non sélec2onnés (ligne pleine) (r=0.74; p<0.001)
Études incluant des pa2ents sélec2onnés (seulement métastases hépa2ques, sans maladie extrahepa2que) (r=0.96; p=0.002)
Études Phase III incluant des pa2ents non sélec2onnés (ligne poin2llée) (r=0.67; p=0.024)
Folprecht G, et al. Ann Oncol 2005;16:1311–1319
Response rate
0.9 0.8 0.7 0.6 0.5 0.4 0.3
Resec2on
rate
0.6
0.5
0.4
0.3
0.2
0.1
0
70%
50%

Q3 : Quel examen de biologie moléculaire est indispensable pour le choix thérapeu2que ?
1. EGFR 2. KRAS 3. NRAS 4. RAS 5. BRAF

R3 : Quel examen de biologie moléculaire est indispensable pour le choix thérapeu2que ?
1. EGFR 2. KRAS 3. NRAS 4. RAS 5. BRAF

Based on Douillard JY, et al. N Engl J Med 2013; 369:1023-34; Oliner KS, et al. EJC 2013; 49 (suppl 3):abstract 2275 (and poster).
2004
An2-‐VEGF An2-‐EGFR
2006
Muta2on KRAS Exon 2 An2-‐EGFR si KRAS non muté
2013
Muta2on Exons 3 et 4 KRAS, NRAS, BRAF… (PRIME et FIRE3)
An2-‐EGFR pour super RAS non muté

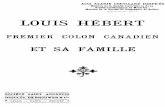
Extracellular
Intracellular
Ligand
EGF-‐R
PI3K
Akt
Raf
MEK
MAPK
Cell Mo2lity
Metastasis Angiogenesis Prolifera2on
Cell survival DNA
Ras
PTEN


Q4: Une chimiothérapie de conversion est indiquée. Quel traitement proposeriez-‐vous?
1. Folfoxiri
2. An2-‐VEGF (Bevacizumab) associée à chimiothérapie (Oxalipla2ne)
3. An2-‐EGFR (Cetuximab) associé à une chimiothérapie (Irinotecan)
4. An2-‐EGFR (Panitumumab) associé à une chimiothérapie (Oxalipla2ne)

R4: Une chimiothérapie de conversion est indiquée. Le KRAS est non muté (Exon 2). Quel traitement proposeriez-‐vous?
1. Folfoxiri
2. An2-‐VEGF (Bevacizumab) associée à chimiothérapie (Oxalipla2ne)
3. An2-‐EGFR (Cetuximab) associé à une chimiothérapie (Irinotecan)
4. An2-‐EGFR (Panitumumab) associé à une chimiothérapie (Oxalipla2ne)


OS PFS

Q5: Après combien de cures vous évaluez votre pa2ent?
1. Après 4 cures
2. Après 6 cures
3. Après 8 cures
4. Après 12 cures

R5: Après combien de cures vous évaluez votre pa2ent?
1. Après 4 cures
2. Après 6 cures
3. Après 8 cures
4. Après 12 cures

Recommanda2ons 2012 : Chimiothérapie néoadjuvante
• L’objec2f de la chimiothérapie néoadjuvante est de rendre résécable et non d’obtenir une réponse complète
• Si progression après 1ère ligne de chimiothérapie ou stabilité après 4 mois de traitement, une 2ème ligne de chimiothérapie doit être considérée
• Le moment op2mum pour évaluer la réponse à la chimiothérapie est de tous les 2 mois (4 cures)
• La chimiothérapie préopératoire devant induire une résécabilité doit être la plus courte possible et elle devra être con2nué en postopératoire
• Un total de 6 mois (12 cures) de chimiothérapie périopératoire est recommandé (préopératoire et postopératoire)
* The Oncologist 2012;17:1-‐15

La chimiothérapie préopératoire altère le parenchyme hépa2que, et au-‐delà de 6 cycles augmente la morbidité après hépatectomie majeure.

Dilata2on sinusoïdale (Oxalipla2ne) Nodule de régénéra2on
Stéatose hépa2que (Irinotecan)

Traitement
• Panitumumab (Vec2bix) + CAPOX – Vec2bix = 6 mg/kg J1-‐J15 – Capecitabine = 1000 mg/m2, J1 à J14 – Oxalipla2ne = 130 mg/m2, J1-‐J28
• 6 cycles – C1 = 13/01/14 – C4 = 07/04/14 – C6 = 09/06/14
• Bonne tolérance du traitement
• An2gène carcino-‐embryonnaire: 533 ng/ml à 7,68 ng/ml

Scan TAP à 4 cures (31/03/14)
• Lobe droit – Segment VIII et IVa: nodule de 70 mm calcifiée – Segment IVb: 3 nodules de 16, 12 et 6 mm – Segment V: nodule de 60 mm – Segment VI: nodule de 14 mm – Segment VII: nodule de 9 mm
• Pas de nodules sur les segments I, II et III

Scan TAP à 6 cures (14/06/14) Réponse par2elle
• Lobe droit – Segment VIII et IVa: nodule de 49 mm calcifiée – Segment IVb: 3 nodules de 14, 10 et 2 mm – Segment V: nodule de 51 mm – Segment VI: nodule de 6 mm – Segment VII: nodule de 5 mm
• Pas de nodules sur les segments I, II et III

Volumétrie hépa2que total = 1505 cc
• Foie gauche (I, II, III et IV) = 541 cc soit 36% (0,8% du poids du corps) • Foie droit (V, VI, VII, VIII) = 964 cc soit 64 • Loge gauche (II et III) + segment I = 450 cc soit 30% (0,6% du poids du corps)
Volumétrie du foie restant limite

Q6: Que feriez-‐vous à l’issue de ce bilan?
1. Vous considérez que le pa2ent est toujours non résécable et vous con2nuez le même protocole pour réduire encore le volume tumoral
2. Vous con2nuez le même traitement, jusqu’à obten2on d’une réponse complète vue que le pa2ent répond bien au traitement
3. Vous pensez que le pa2ent est devenu résécable et vous demandez un
avis à un chirurgien hépa2que

R6: Que feriez-‐vous à l’issue de ce bilan?
1. Vous considérez que le pa2ent est toujours non résécable et vous con2nuez le même protocole pour réduire encore le volume tumoral
2. Vous con2nuez le même traitement, jusqu’à obten2on d’une réponse complète vue que le pa2ent répond bien au traitement
3. Vous pensez que le pa2ent est devenu résécable et vous demandez un
avis à un chirurgien hépa2que

Objec2f = Résec2on R0
• Lobectomie droite emportant les segments 4,5,6,7 et 8
• Préserver le lobe gauche (II et III) et le segment I (450 cc soit 29%)
• Mais volumétrie du foie restant limite et
foie de chimiothérapie
è Faire appel à des moyens techniques pour augmenter le futur foie restant • Embolisa2on portale • ALPPS

ALPPS Associa2ng Liver Par22on and Portal vein liga2on for Stagest hepatectomy

Interven2on (02/07/14)

1er temps du ALPPS (02/07/14)
Veine porte droite
Sec2on parenchymateuse

TDM à J11 post ALPPS (13/07/14)

2ème temps du ALPPS à J21 (23/07/14)
• Lobectomie droite • Résec2on sigmoïdienne • Rétablissement de la con2nuité diges2ve
• Suites opératoires simples • Sor2e à J8 de la 2e interven2on • Durée totale du séjour 1 mois

Résultat anatomo-‐pathologique
• Adénocarcinome bien différencié du sigmoïde de stade pT3N1aM1a • 3 nodules hépa2ques de 70 mm, 55 mm et 10 mm • Réponse post-‐chimiothérapie TRG4 • Marge de résec2on à 1 mm


Scan TAP à J48 (10/09/14)
Pas de nodules hépa2que gauche Hypertrophie compensatrice gauche

Q7: Que proposez-‐vous ?
1. CAPOX 2. CAPOX + an2 EGFR 3. CAPIRI 4. CAPIRI + An2 VEGF 5. Abstension

R7: Que proposez vous ?
1. CAPOX 2. CAPOX + an2 EGFR 3. CAPIRI 4. CAPIRI + An2 VEGF 5. Absten2on