Artériopathie : méthodes et indications de revascularisation · revascularisation for severe limb...
78
Artériopathie : méthodes et indications de revascularisation Julien GAUDRIC Pitié-Salpêtrière, Paris.
Transcript of Artériopathie : méthodes et indications de revascularisation · revascularisation for severe limb...

Artériopathie:méthodesetindicationsderevascularisation
JulienGAUDRICPitié-Salpêtrière,Paris.



L’ARTERIOPATHIEDIABETIQUE• Généralités
• Artéritejambière• Atteinteassociéedel’AFP• N’empêchepasleslésionsd’artérite«banale»• Etenduedesplaiesaggravéesparlaneuropathie
• «PIEDDIABETIQUE»• Contrôledusepsis
• Chirurgical(drainage,débridement,amputation)• Médical(antibiothérapie)
• Evaluationdelapartischémique?• P<50mmHg+douleurrepos/P<70mmHg+ulcère?• TcPO2?• ➔Peucorrélésàl’histoirenaturelleourisqued’amputation
Abolitiondespouls+évolutiondelaplaie
INDICATIONREVASCULARISATION:TROUBLETROPHIQUE/SAUVETAGEDEMEMBRE

ISCHÉMIE INFECTION
ETENDUEDESLESIONS
TRAITEMENTLOCALPUR? REVASCULARISATION?
?
QUIREVASCULARISER?

SAUVEGARDERL’APPUI REVASCULARISER

CLAUDICATION/ISCHEMIECRITIQUE:2PRESENTATIONS/2TRAITEMENTS
CLAUDICATION
• Traitementmédicald’abord• Bilanpréopératoire• Objectifs:
• Qualitédevie• Revascularisationpérenne
ISCHEMIECRITIQUE
• «Pseudo»urgence• Pasd’évaluationcoronairepré-opératoire• Lésionsjambièresprédominantes• Sepsis• Objectifs:
• Revascularisationrapide• Lamoinsinvasivepossible• Permettantuneremobilisationrapide• «Passeruncap»
ENDO?CHIRURGIE?

MORBIDITECHIRURGICALE
TASCII
L’analysedesrésultatsenchirurgievasculairedoittenircomptedelapriseenchargepériopératoiredecesmaladespolyvasculaires.Pasdescoreprédictifdemorbi-mortalitéfiableenchirurgievasculaire.Définitiondespatientsàhautrisquechirurgicaltrèsimparfaite.

RÉSULTATSDESREVASCULARISATIONSARTERIELLESDESMEMBRESINFERIEURSCHIRURGICALESETENDOVASCULAIRES

TASCIIENDOVASCULAIRE
ENDOVSCHIR?
ENDOVSCHIR?
CHIRURGIE

LESIONSJAMBIERES:ISCHEMIECRITIQUE
OBJECTIF:SAUVETAGEDEMEMBRE
• Revascularisationobligatoire• Risqued’amputationmajeur• Pronosticconditionnéparlaveine• Comorbiditésfréquentes(diabeteévolué,IR,alitementprolongé…)
• Dustrictpointdevuedescomorbiditésetducaractèresemi-urgent: intérêtdutraitementendovasculaire;• Dupointdevueanatomique:
Difficultésparticulières,artèresdepetitcalibre,lésionsextensives…

AXEDONNEUR AXERECEVEUR
PONTAGE DISTAL=PRELEVEMENT
DE VEINE SAPHENE

Outflow:Artèrepédieuse

ArtèretibialePostérieurerétromalléolaire

Lésionsjambières:pontagepoplité-pédieux Lésions-fémoro-jambieres:pontageFemoro-jambier

Pontagecomposite



PRELEVEMENT SAPHENE INTERNE

PRÉLÈVEMENT SAPHÈNE : SAPHENOSCOPIE

ROLEDEL’ANGIOPLASTIE?

RESULTATSPONTAGESVSANGIOPLASTIE?
PONTAGES

RESULTATSPONTAGESVSANGIOPLASTIE?ANGIOPLASTIE

RESULTATSPONTAGESVSANGIOPLASTIE?
• MAISEXTENSIONDESLESIONSDIFFERENTE• POPULATIONMIXTE:DOULEURDECUBITUSVSULCÈRES• TAUXDEDIABETIQUES?


Articles
IntroductionIn most developed countries, the incidence of severe limbischaemia, which is the presence of tissue loss(ulceration, gangrene) and pain at rest or at night, isestimated to be 50–100 per 100000 every year and leads topronounced morbidity and mortality as well as to theconsumption of many health-care and social-careresources.1 Ageing populations, the increasing prevalenceof diabetes and its lower-limb-related complications, andthe failure thus far to substantially reduce tobaccoconsumption, mean that despite advances in medicaltherapies, the numbers of patients needing lower limbrevascularisation for severe limb ischaemia will probablyincrease in the foreseeable future. 2,3
Two treatments are currently available; bypass surgeryand balloon angioplasty. Those who favour surgeryusually emphasise good long-term anatomical patencyand clinical durability.4–6 However, this preference couldcome at the cost of high morbidity and mortality as wellas substantial resource use.7 Furthermore, this durabilitycould depend heavily on routine ultrasonography-basedgraft surveillance, often leading to repeated prophylacticre-interventions, and the use of good-quality veins for
grafting.8,9 Unfortunately, adequate vein is oftenunavailable and the long-term results of bypassesconstructed with prosthetic materials are much lesssatisfactory.4,10 By contrast, proponents of balloonangioplasty point to the advantages of low proceduralmorbidity and mortality, reduced costs, the speed withwhich the procedure can be undertaken, and a shortenedhospital stay.11 Furthermore, supporters will claim thatfailed angioplasty does not jeopardise subsequentsurgery and that, unlike bypass surgery, it preservescollaterals so that even if the angioplasty site occludes,symptoms might not return.11–13 Apart from the limitedpatency of angioplasty, critics will state that only a fewpatients may be suitable for use of the transluminaltechnique, and that although a subintimal approachcould increase applicability, the procedure is sotechnically demanding in these patients that satisfactoryresults might not be widely achievable. 14–19
However, these differing opinions are based on littleor no evidence. In previous studies6,20–24 that haveattempted to compare surgery and angioplasty forvarious degrees of lower limb ischaemia, all had one ormore major methodological problems. 16,18–21,25–32
Lancet 2005; 366: 1925–34Published online November 24, 2005DOI:10.1016/S0140-6736(05)67704-5See Comment page 1905*Trial participants listed at end ofreportCorrespondence to: Prof Andrew W Bradbury,Department of Vascular Surgery,University of Birmingham, Heartof England NHS FoundationTrust, Birmingham B9 5SS, [email protected]
www.thelancet.com Vol 366 December 3, 2005 1925
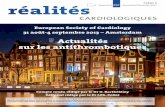
Bypass versus angioplasty in severe ischaemia of the leg(BASIL): multicentre, randomised controlled trialBASIL trial participants*
SummaryBackground The treatment of rest pain, ulceration, and gangrene of the leg (severe limb ischaemia) remainscontroversial. We instigated the BASIL trial to compare the outcome of bypass surgery and balloon angioplasty insuch patients.
Methods We randomly assigned 452 patients, who presented to 27 UK hospitals with severe limb ischaemia due toinfra-inguinal disease, to receive a surgery-first (n=228) or an angioplasty-first (n=224) strategy. The primary endpointwas amputation (of trial leg) free survival. Analysis was by intention to treat. The BASIL trial is registered with theNational Research Register (NRR) and as an International Standard Randomised Controlled Trial, numberISRCTN45398889.
Findings The trial ran for 5·5 years, and follow-up finished when patients reached an endpoint (amputation of trial legabove the ankle or death). Seven individuals were lost to follow-up after randomisation (three assigned angioplasty,two surgery); of these, three were lost (one angioplasty, two surgery) during the first year of follow-up. 195 (86%) of228 patients assigned to bypass surgery and 216 (96%) of 224 to balloon angioplasty underwent an attempt at theirallocated intervention at a median (IQR) of 6 (3–16) and 6 (2–20) days after randomisation, respectively. At the end offollow-up, 248 (55%) patients were alive without amputation (of trial leg), 38 (8%) alive with amputation, 36 (8%) deadafter amputation, and 130 (29%) dead without amputation. After 6 months, the two strategies did not differsignificantly in amputation-free survival (48 vs 60 patients; unadjusted hazard ratio 1·07, 95% CI 0·72–1·6; adjustedhazard ratio 0·73, 0·49–1·07). We saw no difference in health-related quality of life between the two strategies, but forthe first year the hospital costs associated with a surgery-first strategy were about one third higher than those with anangioplasty-first strategy.
Interpretation In patients presenting with severe limb ischaemia due to infra-inguinal disease and who are suitable forsurgery and angioplasty, a bypass-surgery-first and a balloon-angioplasty-first strategy are associated with broadlysimilar outcomes in terms of amputation-free survival, and in the short-term, surgery is more expensive thanangioplasty.
Articles
IntroductionIn most developed countries, the incidence of severe limbischaemia, which is the presence of tissue loss(ulceration, gangrene) and pain at rest or at night, isestimated to be 50–100 per 100000 every year and leads topronounced morbidity and mortality as well as to theconsumption of many health-care and social-careresources.1 Ageing populations, the increasing prevalenceof diabetes and its lower-limb-related complications, andthe failure thus far to substantially reduce tobaccoconsumption, mean that despite advances in medicaltherapies, the numbers of patients needing lower limbrevascularisation for severe limb ischaemia will probablyincrease in the foreseeable future. 2,3
Two treatments are currently available; bypass surgeryand balloon angioplasty. Those who favour surgeryusually emphasise good long-term anatomical patencyand clinical durability.4–6 However, this preference couldcome at the cost of high morbidity and mortality as wellas substantial resource use.7 Furthermore, this durabilitycould depend heavily on routine ultrasonography-basedgraft surveillance, often leading to repeated prophylacticre-interventions, and the use of good-quality veins for
grafting.8,9 Unfortunately, adequate vein is oftenunavailable and the long-term results of bypassesconstructed with prosthetic materials are much lesssatisfactory.4,10 By contrast, proponents of balloonangioplasty point to the advantages of low proceduralmorbidity and mortality, reduced costs, the speed withwhich the procedure can be undertaken, and a shortenedhospital stay.11 Furthermore, supporters will claim thatfailed angioplasty does not jeopardise subsequentsurgery and that, unlike bypass surgery, it preservescollaterals so that even if the angioplasty site occludes,symptoms might not return.11–13 Apart from the limitedpatency of angioplasty, critics will state that only a fewpatients may be suitable for use of the transluminaltechnique, and that although a subintimal approachcould increase applicability, the procedure is sotechnically demanding in these patients that satisfactoryresults might not be widely achievable. 14–19
However, these differing opinions are based on littleor no evidence. In previous studies6,20–24 that haveattempted to compare surgery and angioplasty forvarious degrees of lower limb ischaemia, all had one ormore major methodological problems. 16,18–21,25–32
Lancet 2005; 366: 1925–34Published online November 24, 2005DOI:10.1016/S0140-6736(05)67704-5See Comment page 1905*Trial participants listed at end ofreportCorrespondence to: Prof Andrew W Bradbury,Department of Vascular Surgery,University of Birmingham, Heartof England NHS FoundationTrust, Birmingham B9 5SS, [email protected]
www.thelancet.com Vol 366 December 3, 2005 1925
Bypass versus angioplasty in severe ischaemia of the leg(BASIL): multicentre, randomised controlled trialBASIL trial participants*
SummaryBackground The treatment of rest pain, ulceration, and gangrene of the leg (severe limb ischaemia) remainscontroversial. We instigated the BASIL trial to compare the outcome of bypass surgery and balloon angioplasty insuch patients.
Methods We randomly assigned 452 patients, who presented to 27 UK hospitals with severe limb ischaemia due toinfra-inguinal disease, to receive a surgery-first (n=228) or an angioplasty-first (n=224) strategy. The primary endpointwas amputation (of trial leg) free survival. Analysis was by intention to treat. The BASIL trial is registered with theNational Research Register (NRR) and as an International Standard Randomised Controlled Trial, numberISRCTN45398889.
Findings The trial ran for 5·5 years, and follow-up finished when patients reached an endpoint (amputation of trial legabove the ankle or death). Seven individuals were lost to follow-up after randomisation (three assigned angioplasty,two surgery); of these, three were lost (one angioplasty, two surgery) during the first year of follow-up. 195 (86%) of228 patients assigned to bypass surgery and 216 (96%) of 224 to balloon angioplasty underwent an attempt at theirallocated intervention at a median (IQR) of 6 (3–16) and 6 (2–20) days after randomisation, respectively. At the end offollow-up, 248 (55%) patients were alive without amputation (of trial leg), 38 (8%) alive with amputation, 36 (8%) deadafter amputation, and 130 (29%) dead without amputation. After 6 months, the two strategies did not differsignificantly in amputation-free survival (48 vs 60 patients; unadjusted hazard ratio 1·07, 95% CI 0·72–1·6; adjustedhazard ratio 0·73, 0·49–1·07). We saw no difference in health-related quality of life between the two strategies, but forthe first year the hospital costs associated with a surgery-first strategy were about one third higher than those with anangioplasty-first strategy.
Interpretation In patients presenting with severe limb ischaemia due to infra-inguinal disease and who are suitable forsurgery and angioplasty, a bypass-surgery-first and a balloon-angioplasty-first strategy are associated with broadlysimilar outcomes in terms of amputation-free survival, and in the short-term, surgery is more expensive thanangioplasty.
PourlespatientsavecIschémieSévèreliéeàuneartéritedistale,angioplastieetchirurgieoffrentlesmêmesrésultatsentermedemortalitéetd’amputationles2premièresannées.

Survie>2ans70%

1.Forpatientswithlimb-threateninglowerextremityischemiaandanestimatedlife
expectancyof2yearsorlessorinpatientsinwhomanautogenousveinconduitisnot
available,balloonangioplastyisreasonabletoperformwhenpossibleastheinitial
proceduretoimprovedistalbloodflow(54).(LevelofEvidence:B)
2.Forpatientswithlimb-threateningischemiaandanestimatedlifeexpectancyof
morethan2years,bypasssurgery,whenpossibleandwhenanautogenousvein
conduitisavailable,isreasonabletoperformastheinitialtreatmenttoimprovedistal
bloodflow(54).
(LevelofEvidence:B)
NouvellesrecommandationsTASCII(2011)
Matérieldédié:• guide.O14,.O18,basprofil,• ballonslongsde1,5-4mm• Kitsdeponctionrétrograde…

LESIONSJAMBIERES+++

ARTEREPOPLITEE?

Développementdenouveauxmatérielsdédiés

ENDOVASCULAIRE: RECANALISATION

CONCEPTD’ANGIOSOME
Privilégierlarevascularisationdirecte

RECANALISATIONSMULTIPLESBOUCLEPLANTAIRE


0
23
45
68
90
YUKON DESTINY ACHILLES
STENTNUSIROLIMUS
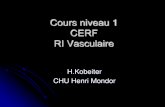
COMPARAISONSTENTSIROLIMUSVSSTENTNUPOURLESLÉSIONSJAMBIERES
Perméabilitéà1an(%)
P<0,05
MAIS:Pasdebénéficesur• mortalité• amputation
Augmentationducoût
Attentionauxétudes!Indicationsdesstentsjambiers??

ENPRATIQUE…
Lésionsjambièresexclusives:
Angioplastieenpremièreintention
Occlusionfémoro-jambièreOuechecd’angioplastie:
Pontage

• OBJECTIF:CICATRISATION/GARDERL’APPUI

CONCLUSION
• L’indicationderevascularisationestliéeàl’importancedelaplaieetàsonévolution
• Patientsauxcomorbiditésévères(avecespérancedevieréduite)
• Nombreusescombinaisonsanatomo-cliniques(sévéritédeslésions+/-corréléesauretentissement)quidoiventbienfairemesurerl’indicationopératoire
• Perméabilitéettauxd’amputationsontdifférents
• Attentionauxtechnologiesnouvellesdontlerenouvellementpermanentempêchedeconclurequantal’efficacité
• Letraitementendovasculaireaprisuneplaceimportantedanslapriseenchargedecespatients
• Lesdeuxtechniquesdoiventêtremaîtriséespourchoisirlaplusadaptée.

AAA CHEZ LE SUJET AGE
JGAUDRIC,YLeMANACH,LCHICHE,FKOSKASChirurgieVasculaire
Départementd’AnesthésieRéanimationPitié-Salpêtrière

CHIRURGIEAORTIQUE
• AAA sous rénal• Mortalité péri opératoire
• AAA asymptomatique < 2,7%• AAA symptomatique =20%• AAA rompu =50%
• Chirurgie ouverte vs endovasculaire• Diminution de la mortalité précoce /3• Pas de bénéfice à moyen/long terme (EVAR, DREAM)

CHIRURGIEAORTIQUE
CHIRURGIE OUVERTE• Pas de contrainte anatomique• Limitée par:
• Insuffisance respiratoire• Insuffisance cardiaque• Coronaropathie
CHIRURGIE ENDOVASCULAIRE• Peut être réalisée sous anesthésie locale• Limitée par:
• conditions anatomiques

Rupture : taux
0
15
30
45
60
30-35 35-40 40-45 45-50 50-55 55-60 60-65
Taux de ruptureCourbes 2
Size (mm)
%
Directlyproportionaltothesize

Anevrysme Thoracique Anevrisme Thoraco-abdominal
Autres Localisations

Traitement• Traitement Chirurgical
• Traitement Endovasculaire
Polyester Gore-tex
StentAutoexpansibleProthese

Chirurgie ouverte
• Consiste à ouvrir la portion aortique dilatée et la remplacer par une prothèse synthétique. Lorsque la prothèse est cousue aux collets proximal et distal le sac anévrismal est refermée autour de la prothèse

Chirurgie ouverte
Laparotomie médianeLAPAROTOMIE

• Voie rétro-péritonéaleVOIERETROPERITONEALE

Sous renal Sus renal Coeliaque
Clampageproximal
Clampagedistal

Prothèse aorto-aortique tubulaire
Anastomose proximale

AAA:Traitement Endovasculaire




PROJECTIONS DEMOGRAPHIQUES
DEUX FOIS PLUS DE PATIENTS AGES >80 ANS EN 2050 (11 MILLIONS)

EPIDEMIOLOGIE DES PATHOLOGIES VASCULAIRES
DOUBLEMENT DE LA PREVALENCE ENTRE 65 ET 80 ANS

ELEMENTS DECISIONNELS CHEZ UN SUJET AGE
Patient ≥ 80 ans=
Esperance de vie faible ?
Chirurgie aortique=
Chirurgie a risque élevé
Traitement AAA=
Traitement préventif
Risquederupture?Surmortalité?
Evaluationdurisque
?Diamètre?
EXISTE-T-ILUNBENEFICEAOPERERCESMALADES?
ComorbiditésFragilitéSous-groupes?
OUI,SIRISQUEOPERATOIRETRESFAIBLE

RISQUE DE RUPTURE

EVALUATION DU RISQUE OPERATOIRE?RECOMMANDATIONS AFSSAPS
Les patients à risque chirurgical élevé doivent présenter un des facteurs suivants :
-Âge supérieur ou égal à 80 ans.
-Coronaropathie (antécédent[s] d’infarctus de myocarde ou angor) avec test fonctionnel positif et
lésions coronariennes pour lesquelles un geste de revascularisation est impossible ou non indiqué.
-Insuffisance cardiaque avec manifestations cliniques patentes.
-Rétrécissement aortique serré non opérable.
-FEVG<40%.
-Insuffisance respiratoire chronique objectivée par un des critères suivants :
- VEMS < 1,2 l/sec;
- CV < 50 % de la valeur prédite en fonction de l’âge, du sexe et du poids ;
AGE COMME CRITERE INDIVIDUEL DE RISQUE?

EVALUATION DU RISQUE OPERATOIRE?
• Critères AFFSSAPS très insuffisants
• Mais pas de score prédictif fiable en chirurgie vasculaire
• Moindre tolérance aux complications (hémorragiques…)
• Moindre réserve physiologique
Evaluation du risque opératoire chez le sujet agé:
• Evaluation des facteurs de risque habituels• Et du retentissement de l'âge civil

CONCEPT DE FRAGILITE
Variables:FRAGILITE -Fonctioncognitive
• Mini-CogTest:3ItemsRecall,ClockDrawingTest -Dénutrition
• Pertedepoids>10lbs,BMI<25,Albumine -Chutes
• Chutesinexpliquées<6mois(proprioception,fonctionmusculaire) -Dépression -AnémieDÉPENDANCE
• Katzindex(Autonomiepours’habiller,toilette,alimentation,transfert, continence)CO-MORBIDITÉS -CharlsonIndex(IDM,IC,AOMI,démence,AVC,IRC,diabete,IHC,VIH…) -ASA

CONCEPT DE FRAGILITE
Chez le sujet âgé, la part de fragilité et de dépendance habituellement évaluées par l’appréciation clinique, indépendamment des comorbidités observées, font l’objet de scores prédictifs.

RESULTATS PITIE-SALPÊTRIERE
Augmentation du nombre de patients > 80 ans. Chirurgie aortique

RESULTATS PITIE-SALPÊTRIERE
Diminution de la part des >80 ans dans les décès post-op• Prise en charge réanimatoire?• Sélection des indications?
Taux décès post-op: 2,7%
Age = Faux problème?

RESULTATS PITIE-SALPÊTRIERE
Taux de comorbidités comparablesEvaluation du risque identique quel que soit l’âge

AGE COMME CRITERE INDIVIDUEL DE RISQUE ?
Impact de l’âge sur la mortalité après chirurgie d’un AAA en France (source PMSI 2009) sans et après ajustement par les facteurs de risque associés.
En l’absence de prise en compte des facteurs de fragilité, on ne constate pas de surmortalité après 80 ans. L'âge ne semble donc pas être un facteur individuel de risque.

CHIRURGIE REGLEE AAA Eff. > 80 ans < 80 ans
Treiman, Am J Surg 1982 35 8,6 % 4,3 %
Glock, J Cardiovasc Surg 1990 29 6,9 % 4,3 %
Dean, Ann Surg 1993 18 5,6 %
Paty, Am J Surg 1993 77 3 % 2 %
O’Hara, JVS 1995 94 9,6 %
Pizzetti, Recenti Prog Med 1995 4,68 %
Soisalon-Soinimen, Vasa 1998 12 8 % 8 %
Van Damme, Acta Chir Belg 1998 52 5,7 % 3,6 %
Kazmers, Ann Vasc Surg 1998 206 8,25 % 4,1 %
Mailapur, J Cardiovasc Surg 2001 62 1,4 %
Dainese, Eur J Vasc Endovasc Surg 2005 30 3,1 %
Haug, Eur J Endovasc Surg 2005 105 10,5 %
Rigberg, J Vasc Surg 2006 1200 7,2 % 3,6 %
Woo, J Vasc Surg 2011 65 6 %
Total 1985 7,2 % 4,3 %
RESULTATS DE LA CHIRURGIE OUVERTE >80 ANS

RESULTATS DU TT ENDOVASCULAIRE >80 ANS
Surmortalité, mais…Résultats acceptables
Pas de différence liée à l'âge chez les patients à haut risque

RESULTATS DU TT ENDOVASCULAIRE >80 ANS
Indication de choix si conditions anatomiques favorables?Bénéfice / chirurgie ouverte ?

ETUDES COMPARATIVES ENDO VS CHIRURGIE

ETUDES COMPARATIVES ENDO VS CHIRURGIE
Avantage systématique au tt endovasculaire sur mortalité et morbidité++

ETUDES COMPARATIVES ENDO VS CHIRURGIE

TRAITEMENT ENDOVASULAIRE vs CHIRURGIE OUVERTE

Le bénéfice périopératoire au traitement endovasculaire existe dans tous les groupes et s’accroit avec l'âge.

CONCLUSION
• L'âge en soit n’est pas un facteur décisionnel de non indication chirurgicale.
• La surmortalité observée est cependant en nette diminution depuis plusieurs années
• L’élément pronostic principal reste le degré de comorbidités associées, logiquement plus important que pour les populations plus jeunes.
• L’évaluation clinique pré opératoire doit donc tenir compte des comorbidités habituelles et évaluer la fragilité du sujet âgé par des échelles spécifiques.

CONCLUSION
• Le risque encouru doit être corrélé au risque de ruptureIl est donc licite de ne proposer un traitement qu’à partirde 6 cm de diamètre.
• Le traitement endovasculaire doit être privilégié si les conditions anatomiques le permettent, mais le vieillissementest aussi responsable de rigidité du système artériel exposant à plus de complications de navigation et de largage
• Le traitement chirurgical doit être simplifié en ne traitant que les lésions menaçantes (tube aorto-aortique plutot queaorto-biiliaque si atteinte modérée des iliaques)

Espérance de vie/Risque chirurgical
NULLE / ELEVE < 100%
AAA > 80 ANS
CHIRURGIE CURATIVE CHIRURGIE PREVENTIVE
Espérance de vie/Risque chirurgical
FAIBLE / ELEVE ?
CHIR / ENDO
risque connu? Bénéfice?DECISION: -Ethique-Economique?-Familiale?
Symptomatique Asymptomatique
ELEMENTS DECISIONNELS CHEZ UN SUJET AGE

Registre suedois 1987-20058663 AAAMortalité J30 • <80=3,8% (chir + endo)• >80=6,8% (chir + endo)
EFFET DU TRAITEMENT SUR LA SURVIE
Survie relative >80 comparable à Population générale <80
Biais de sélection?