Annexure - gmscl.gujarat.gov.in · Annexure : B . Installation completion Certificate cum Detail...
6
Transcript of Annexure - gmscl.gujarat.gov.in · Annexure : B . Installation completion Certificate cum Detail...


Annexure – A
5|DF65+ sGM\W o VF5GF VlWS lGIFDSzL DFZOT[ DMS,L VF5JFG]\ ZC[X[ f
VFYL 5|DF65+ VF5JFDF\ VFJ[ K[ S[4
s!f ;NZ AL,G]\ R]SJ6]\ V+[GL SR[ZL wJFZF SZFJDF\ VFJ[, GYL VG[
ElJQIDF\ SZJFDF\ VFJX[ GCLP
sZf AL,DF\ NXF"J[, ;FWG VM0"Z DF\ NXF"J[, :5[XLOLS[XG D]HA K[P
s#f ;FWGG]\ .g:8M,[XG VG[ 0[DM:8=[XG ;\TMQFSFZS ZLT[ YI[, K[ VG[ ;FWG
RF,] CF,TDF\ K[P
s$f ;FWG V+[GL SR[ZLGF 0[0 :8MS ZHL:8ZGF 5[H G\AZPPPPPPPPPPPPPPPPPPPPP
p5Z S|D G\AZPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPP p5Z GM\WJFDF\ VFJ[, K[P
s5f ;FWG V+[GL SR[ZLDF\ TFPPPPPPPPPPPPPPPPPPPPPPPPPPPPP GF ZMH D/[, K[4 T[DH
TFPPPPPPPPPPPPPPPPPPPPPPPPPPPPPGF ZMH >g:8M, s5|:YFl5Tf YI[, K[P
s&f ;LPV[DP;LP DF8[GM VM0"Z G\AZ PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPP
PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPTFPPPPPPPPPPPPPPPPPPPPP T[DH TFPPPPPPPPPPPPPPPPP
YL TFPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPP NZdIFG 5[-L äFZF ;\TMQFSFZS q
V;\TMQFSFZS ;lJ"; VF5[, K[P
s*f AL,G]\ R]SJ6]\ SZJF E,FD6 SZJFDF\ VFJ[ K[P
;1FD VlWSFZLGL ;CL VG[ ;LSSM
admin
Typewritten Text
admin
Typewritten Text
Bill no:_____________ date:_____________
admin
Typewritten Text
admin
Typewritten Text
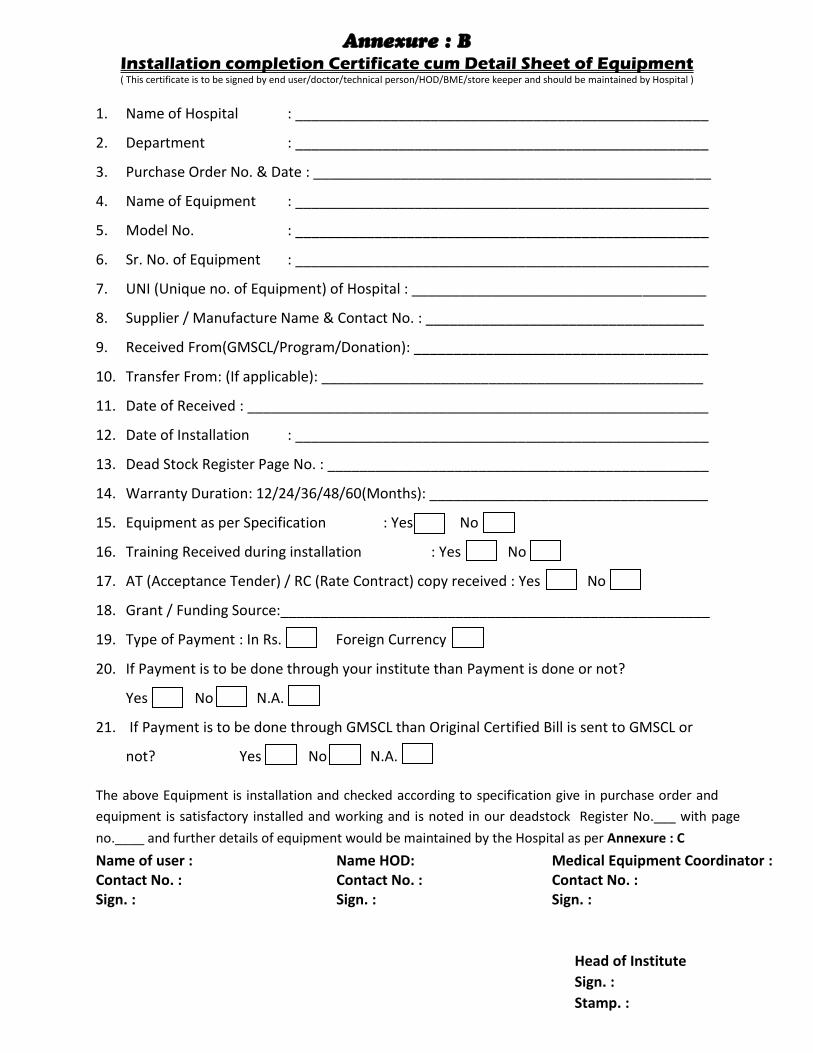
Annexure : B
Installation completion Certificate cum Detail Sheet of Equipment ( This certificate is to be signed by end user/doctor/technical person/HOD/BME/store keeper and should be maintained by Hospital )
1. Name of Hospital : ____________________________________________________
2. Department : ____________________________________________________
3. Purchase Order No. & Date : __________________________________________________
4. Name of Equipment : ____________________________________________________
5. Model No. : ____________________________________________________
6. Sr. No. of Equipment : ____________________________________________________
7. UNI (Unique no. of Equipment) of Hospital : _____________________________________
8. Supplier / Manufacture Name & Contact No. : ___________________________________
9. Received From(GMSCL/Program/Donation): _____________________________________
10. Transfer From: (If applicable): ________________________________________________
11. Date of Received : __________________________________________________________
12. Date of Installation : ____________________________________________________
13. Dead Stock Register Page No. : ________________________________________________
14. Warranty Duration: 12/24/36/48/60(Months): ___________________________________
15. Equipment as per Specification : Yes No
16. Training Received during installation : Yes No
17. AT (Acceptance Tender) / RC (Rate Contract) copy received : Yes No
18. Grant / Funding Source:______________________________________________________
19. Type of Payment : In Rs. Foreign Currency
20. If Payment is to be done through your institute than Payment is done or not?
Yes No N.A.
21. If Payment is to be done through GMSCL than Original Certified Bill is sent to GMSCL or
not? Yes No N.A.
The above Equipment is installation and checked according to specification give in purchase order and
equipment is satisfactory installed and working and is noted in our deadstock Register No.___ with page
no.____ and further details of equipment would be maintained by the Hospital as per Annexure : C
Name of user : Contact No. : Sign. :
Name HOD: Contact No. : Sign. :
Medical Equipment Coordinator : Contact No. : Sign. :
Head of Institute
Sign. :
Stamp. :

Annexure – c
Service Satisfaction Certificate
(This certificate is to be signed by end user/doctor/technical person/HOD/BME/store keeper and should be maintained year wise by Hospital)
(During Warranty / CMC)
Equipment under warranty or CMC: ___________________________________________
(1) Purchase Order No. & Date: ________________________________________________
(2) Name of Equipment : __________________________________________________
(3) Model No. : __________________________________________________
(4) Sr. No. of Equipment : __________________________________________________
(5) UNI (Unique no. of Equipment) of Hospital : ___________________________________
(6) Supplier / Manufacture Name & Contact No. : __________________________________
(7) Date of Installation : __________________________________________________
(8) No. of test details of usage of Equipment : _____________________________________
(9) CMC done by (Local / GMSCL) : ___________________(if under CMC)
(10) Service provider / Maintenance Contact No. / Address :
_______________________________________________________________________
(11) No. of Year of Warranty / CMC : _____ year
(12) Period of Warranty / CMC : _____________ to ____________
Free Preventive Maintenance Services Details during Warranty / CMC:
Sr. No. Services Number
Date of Service Service Engineer
contact and contact number
Hospital authorized person sign
Remarks
1
2
3
4
Other break down details:
This is to certify that above given Information related service of Equipment during
warranty has been ________ (given/Not given) by company & all service report and record
would be maintained by Hospital.
Name of user : Contact No. : Sign. :
Name HOD: Contact No. : Sign. :
Medical Equipment Coordinator : Contact No. : Sign. :
Head of Institute
Sign. :
Stamp. :
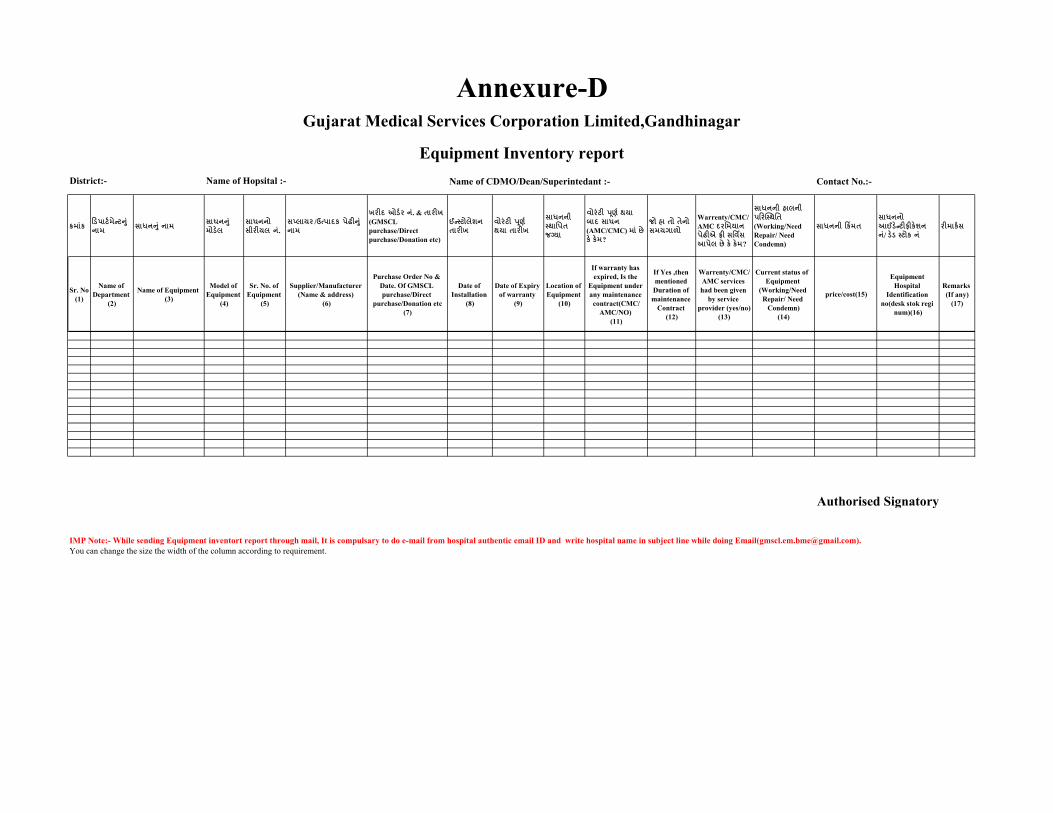
Name of CDMO/Dean/Superintedant :- Contact No.:-
ક્રમ ાંક ડિપ ર્ટ મેન્ર્ન ાં ન મ સ ધનન ાં ન મ સ ધનન ાં
મોિેલસ ધનનો સીરીયલ નાં.
સપ્લ યર /ઉત્પ દક પેઢીન ાં ન મ
ખરીદ ઓિટર નાં. & ત રીખ
(GMSCL
purchase/Direct
purchase/Donation etc)
ઈન્્ર્ોલેશન
ત રીખવોરાંર્ી પરૂ્ટ થય ત રીખ
સ ધનની ્થ પપત
જગ્ય
વોરાંર્ી પરૂ્ટ થય બ દ સ ધન
(AMC/CMC) મ ાં છે
કે કેમ?
જો હ તો તેનો સમયગ ળો
Warrenty/CMC/
AMC દરપમય ન
પેઢીએ ફ્રી સપવિસ
આપેલ છે કે કેમ?
સ ધનની હ લની પડરસ્્થપત
(Working/Need
Repair/ Need
Condemn)
સ ધનની ડકિંમતસ ધનનો આઈિેન્ર્ીફીકેશન
નાં/ િેિ ્ર્ોક નાંરીમ કટસ
Sr. No
(1)
Name of
Department
(2)
Name of Equipment
(3)
Model of
Equipment
(4)
Sr. No. of
Equipment
(5)
Supplier/Manufacturer
(Name & address)
(6)
Purchase Order No &
Date. Of GMSCL
purchase/Direct
purchase/Donation etc
(7)
Date of
Installation
(8)
Date of Expiry
of warranty
(9)
Location of
Equipment
(10)
If warranty has
expired, Is the
Equipment under
any maintenance
contract(CMC/
AMC/NO)
(11)
If Yes ,then
mentioned
Duration of
maintenance
Contract
(12)
Warrenty/CMC/
AMC services
had been given
by service
provider (yes/no)
(13)
Current status of
Equipment
(Working/Need
Repair/ Need
Condemn)
(14)
price/cost(15)
Equipment
Hospital
Identification
no(desk stok regi
num)(16)
Remarks
(If any)
(17)
Authorised Signatory
IMP Note:- While sending Equipment inventort report through mail, It is compulsary to do e-mail from hospital authentic email ID and write hospital name in subject line while doing Email([email protected]).
You can change the size the width of the column according to requirement.
Gujarat Medical Services Corporation Limited,Gandhinagar
Equipment Inventory report
District:- Name of Hopsital :-
Annexure-D
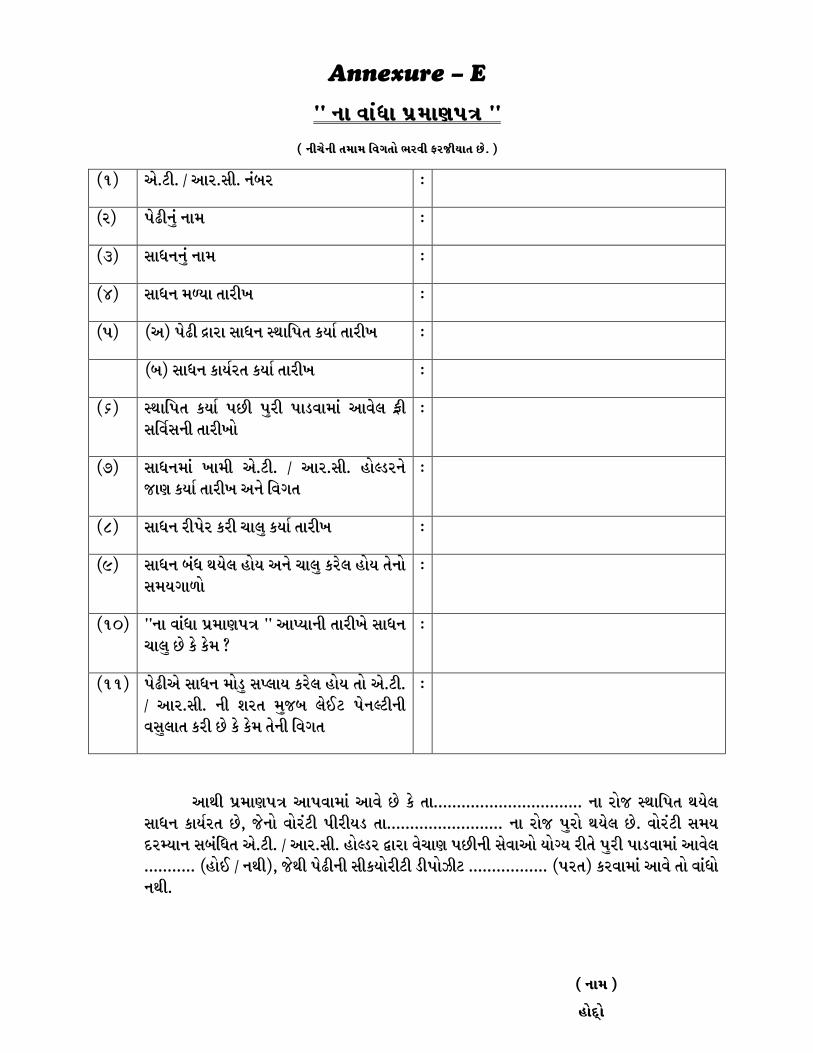
Annexure – E
cc GF JF\WF 5|DF65+ cc
s GLR[GL TDFD lJUTM EZJL OZHLIFT K[P f
s!f V[P8LP q VFZP;LP G\AZ o
sZf 5[-LG]\ GFD o
s#f ;FWGG]\ GFD o
s$f ;FWG D?IF TFZLB o
s5f sVf 5[-L ãFZF ;FWG :YFl5T SIF" TFZLB o
sAf ;FWG SFI"ZT SIF" TFZLB o
s&f :YFl5T SIF" 5KL 5]ZL 5F0JFDF\ VFJ[, O|L ;lJ";GL TFZLBM
o
s*f ;FWGDF\ BFDL V[P8LP q VFZP;LP CM<0ZG[ HF6 SIF" TFZLB VG[ lJUT
o
s(f ;FWG ZL5[Z SZL RF,] SIF" TFZLB o
s)f ;FWG A\W YI[, CMI VG[ RF,] SZ[, CMI T[GM ;DIUF/M
o
s!_f ccGF JF\WF 5|DF65+ cc VF%IFGL TFZLB[ ;FWG RF,] K[ S[ S[D m
o
s!!f 5[-LV[ ;FWG DM0] ;%,FI SZ[, CMI TM V[P8LP q VFZP;LP GL XZT D]HA ,[.8 5[G<8LGL J;],FT SZL K[ S[ S[D T[GL lJUT
o
VFYL 5|DF65+ VF5JFDF\ VFJ[ K[ S[ TFPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPP GF ZMH :YFl5T YI[, ;FWG SFI"ZT K[4 H[GM JMZ\8L 5LZLI0 TFPPPPPPPPPPPPPPPPPPPPPPPPP GF ZMH 5]ZM YI[, K[P JMZ\8L ;DI NZdIFG ;A\lWT V[P8LP q VFZP;LP CM<0Z äFZF J[RF6 5KLGL ;[JFVM IMuI ZLT[ 5]ZL 5F0JFDF\ VFJ[, PPPPPPPPPPP sCM. q GYLf4 H[YL 5[-LGL ;LSIMZL8L 0L5MhL8 PPPPPPPPPPPPPPPPP s5ZTf SZJFDF\ VFJ[ TM JF\WM GYLP
s GFD f
CMNŸM