Anglani Et Al_2010

of 8
Transcript of Anglani Et Al_2010
-
7/26/2019 Anglani Et Al_2010
1/8
The Regenerative Potential of the Kidney: What Can We
Learn from Developmental Biology?
Franca Anglani &Federica Mezzabotta &Monica Ceol &
Rosalba Cristofaro &Dorella Del Prete &
Angela DAngelo
Published online: 17 August 2010# Springer Science+Business Media, LLC 2010
Abstract Cell turnover in the healthy adult kidney is very
slow but the kidney has a strong capacity for regenerationafter acute injury. Although many molecular aspects of this
process have been clarified, the source of the newly-formed
renal epithelial cells is still being debated. Several studies
have shown, moreover, that the repair of injured renal
epithelium starts from mature tubular cells, which enter into
an activated proliferative state characterized by the reappear-
ance of mesenchymal markers detectable during nephro-
genesis, thus pointing to a marked plasticity of renal epithelial
cells. The regenerative potential of mature epithelial cells
might stem from their almost unique morphogenetic process.
Unlike other tubular organs, all epithelial and mesenchymal
cells in the kidney derive from the same germ layer, the
mesoderm. In a fascinating view of vertebrate embryogenesis,
the mesoderm might be seen as a cell layer capable of
oscillating between epithelial and mesenchymal states, thus
acquiring a remarkable plasticity that lends it an extended
potential for innovation and a better control of three-
dimensional body organization. The renal papilla contains a
population of cells with the characteristic of adult stem cells.
Mesenchymal stromal stem cells (MSC) have been found to
reside in the connective tissue of most organs, including thekidney. Recent studies indicate that the MSC compartment
extends throughout the body postnatally as a result of its
perivascular location. Developmental biology suggests that
this might be particularly true of the kidney and that the
papilla might represent the perivascular renal stem cell niche.
The perivascular niche hypothesis fits well with the evolving
concept of the stem cell niche as an entity of action. It is its
dynamic capability that makes the niche concept so important
and essential to the feasibility of regenerative medicine.
Keywords Renal adult stem cells . Kidney development.
EMT . Cell plasticity . Pericytes . Perivascular niche
Introduction
The adult mammalian renal tubular epithelium exists in a
relatively quiescent to slowly replicating state, and cell turnover
in the healthy adult kidney is very slow. The kidney has a strong
capacity for regeneration, despite the postnatal mammalian
kidney being unable to generate new nephrons in response to
nephron loss. No new nephrons are generated after 36 weeks of
gestation in humans, but a renal stem cell system is supposed to
contribute to the replacement of postnatal cell types [1].
The anatomical and functional recovery of renal integrity
after injury is accompanied by the activation of sophisti-
cated processes that have yet to be fully understood, by
means of which damaged tubular cells are replaced by
normal, well-functioning cells that reorganize their archi-
tecture to recreate a normal tubule. Although many of the
molecular details of this process have been clarified over
the last 20 years, the cellular source of the newly-formed
renal epithelial cells is still being debated. Some studies
F. Anglani :F. Mezzabotta :M. Ceol : R. Cristofaro
Laboratory of Kidney Histomorphology and Molecular Biology,
Department of Medical and Surgical Sciences, University of Padua,
Padua, Italy
D. Del Prete :A. DAngelo
Division of Nephrology, Department of Medical and Surgical
Sciences, University of Padua,
Padua, Italy
F. Anglani (*)
Divisione di Nefrologia, Policlinico IV piano,
Laboratorio di Istomorfologia e Biologia Molecolare del Rene,
Via Giustiniani n2,
35128 Padova, Italy
e-mail: [email protected]
Stem Cell Rev and Rep (2010) 6:650657
DOI 10.1007/s12015-010-9186-6
-
7/26/2019 Anglani Et Al_2010
2/8
showed that novel cells derive from the division of
differentiated cells [2, 3]; others claimed that subpopula-
tions of renal tubular cells act as progenitor cells [ 47]; and
yet others demonstrated that hematopoietic stem cells and
circulating mesenchymal stem cells can repopulate the
tubular cell system [8, 9]. Indeed, a wide variety of
potential progenitor or adult stem cell populations have
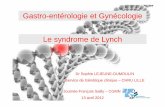
been identified in human and rodent kidneys on the basis oftheir functional and/or phenotypic characteristics in the
glomerular and in the tubular/interstitial compartments
(reviewed in [10]) (Fig.1). Many organs, particularly those
with a high cell turnover, are believed to harbor a stem cell
population that sustains normal organ structure and con-
tributes to repair, and some of these organs contain several
types of stem/precursor cells that provide new cells for
specific locations and functions. Recent studies have shown
in organs such as the skin [21] and liver [22] that the
precursor cells responsible for homeostatic cell turnover
differ from those responsible for cell replacement after
injury. Given the complexity of the renal architecture andthe numerous cell types involved, the kidney probably has
multiple mechanisms of cell renewal and regeneration too.
Cell renewal and regeneration
Most data on the origin of new tubular epithelial cells in the
kidney derive from studies on the regeneration/repair
process after tubular necrosis due to ischemic injury. Since
the S3 segment of the proximal tubule is the part of the
nephron most susceptible to injury and appears to have the
highest proliferation rate (in young rats at least), most
studies on regenerative nephrogenesis have focused on the
proximal tubular epithelial cells (TECs). Vogetseder et al.
[2325] showed that cell proliferation in the healthy kidney
of young rats relies on differentiated TEC division. Moreimportantly, in a recent study using a refined technique
called genetic fate mapping, Humphereys et al. [26] clearly
demonstrated that differentiated TECs surviving after
ischemia-reperfusion injury generated most, if not all, new
tubular epithelial cells.
Taking a morphological approach, Vogetseder et al. [23]
showed that, in the healthy kidney, the slow cycling cells in
the S3 segments (label retaining cells, LRCs)identifiable
from their ability to retain BrdUexpressed markers of
terminal differentiation and a typical tubular cell polarity.
This study showed that the cell proliferation pattern in the
S3 segment fails to display the characteristic features of astem cell system. The authors also found that the
proliferative capacity of renal TECs comes from a large
reserve of cells in the G1 phase, which ensures a rapid
proliferative response when needed. This was a theory first
advanced by Lin et al. [27] who tagged renal TECs with
green fluorescent protein and provided compelling evidence
of mature TECs having a leading role in the regeneration
process in the post-ischemic kidney. The findings reported
Fig. 1 Distribution of stem/progenitor cells within the adult kidney. The different cell types involved are indicated. Studies conducted on mouse
or human kidney [47,1120] evidence a distributed presence of renal stem/progenitor cells
Stem Cell Rev and Rep (2010) 6:650657 651
-
7/26/2019 Anglani Et Al_2010
3/8
by Humphereys et al. [26] substantially confirm these data,
elegantly demonstrating that no extratubular cells or intra-
tubular stem/progenitor cells contribute to the repair
process. They did not address, however, the possibility that
there may be distinct differences in the regenerative
potential among tubular cells.
So where or what does this regenerative potential of mature
epithelial cells come from? Developmental biology couldprovide the answer.
Epithelial-to-mesenchymal transition in developmental
processes
Several studies have shown that the repair of injured renal
epithelium begins when surviving tubular cells enter into an
activated proliferative state characterized by the reappear-
ance of mesenchymal markers detectable during nephro-
genesis [28]. After injury, therefore, the conversion of
TECs to a more mesenchymal phenotype suggests that anepithelial-to-mesenchymal transition does indeed occur.
Epithelial-to-mesenchymal transition (EMT) is a complex,
extreme manifestation of epithelial plasticity. It is now
widely recognized as a fundamental process in pathological
conditions (oncogenesis and fibrogenesis) as well as in
physiological events such as morphogenesis [29, 30].
During the development of the vertebrate embryo,
EMTs are a source of mesenchyme in various places and
stages throughout embryonic morphogenesis, but espe-
cially in the mesodermal domains [31]. It is currently
accepted that the epithelia precede both evolutionary and
ontogenetically the mesenchyme, and that the mesen-
chyme was originally an epithelial derivative [32]. Thus,
the epithelium is the earliest type of embryonic organiza-
tion, and the primitive epiblast represents the earliest
epithelial state in vertebrate development. The first EMT
occurs at gastrulation, when a subset of epiblast cells
undergo EMT and internalize to generate mesoderm and
endoderm, while those remaining in the epiblast become
ectoderm [33]. Mesoderm and endoderm contribute to
many tissues in the adult body that subsequently undergo
several rounds of EMT and MET (the latter being reverse
of EMT i.e. mesenchymal-to-epithelial transition). Imme-
diately after the primary mesenchyme has formed, most
mesoderm and all endoderm become reorganized in
primitive epithelia. These secondary epithelia give rise to
secondary mesenchymal cells in a series of EMTs. In
particular, intermediate mesoderm generates the nephro-
genic mesenchyme, which coalesces in tertiary epithelial
structures such as nephrones and nephric ducts [34].
In a very interesting model proposed by Perez-Pomares
et al. [31], the vertebrate embryo is considered as a two-
state system of which epithelium and mesenchyme repre-
sent the stable and unstable states, respectively. In partic-
ular, mesoderm might be seen as a cell layer capable of
oscillating between the plastic and exploratory behavior of
the mesenchyme and the stability of the epithelia. The
ability to go through cycles of epithelial and mesenchymal
states lends the mesoderm a greater plasticity, more
potential for innovation and a better control of three-
dimensional body organization [31]. The mesenchymederived from the chronologically earliest EMT has the
greatest developmental potential, which decreases progres-
sively in the subsequent EMTs. This model has a particular
appeal for explaining the kidneys almost exclusively
morphogenic process as well as its regenerative potential.
In this setting, some of the developmental potential of the
primitive epithelium may remain in the definitive epitheli-
um derived from the mesenchyme (as in renal epithelial
cells), enabling cells to respond quickly to micro-
environmental changes. Indeed, very recently, two papers
have proposed that EMT could be the process driving
mammary epithelial cells [35] and glomerular parietalepithelial cells [36] to adopt stem cell characteristics.
These remarks could suggest that the kidneys need for a
real stem cell compartment is less important than the cells
phenotypic flexibility, as in other mesenchymal tissues. The
plasticity of TECs resembles that of adult mesenchymal cells,
which are long-lived and constantly exposed to the extracel-
lular matrix. The matrix provides a microenvironment that
helps the cells to maintain a differentiated or undifferentiated
state, i.e. the cell plasticity of this tissue seems to serve the
same purpose as the multipotency of adult stem cells
without the need for a real stem cell compartment [37].
The renal papilla as a stem cell niche
Oliver et al. [38] found a high proliferation rate in the upper
papilla, especially laterally, adjacent to the urinary space of the
normal kidney. By staining renal tissue sections from adult 1-
yr old rats with Ki67, they found positive cells in the upper
papilla with a frequency that was low (2.6% of all cells), but
significantly higher than elsewhere in the kidney. The same
Authors also found LRCs with several characteristics of adult
stem cells in the papillary interstitium and collecting duct, that
were able to generate new cells in the normal adult kidney.
They suggested that, during normal homeostasis, interstitial
LRCs or their immediate progeny migrate to the upper papilla
and form a compartment of rapidly proliferating cells that may
have a role after acute injury.
Dekel et al. [6] also found non-tubular Sca-1+ multi-
potent/progenitor cells in the adult mouse kidney, located
mainly in the papillary interstitial space. These cells were
located in the outermost part of the papilla, close to the
tubules and sometimes adjacent to the tubular basal surface,
652 Stem Cell Rev and Rep (2010) 6:650657
-
7/26/2019 Anglani Et Al_2010
4/8
and they displayed some features of the papillary stem cells
isolated by Oliver at al. [38].
Unlike other areas of the kidney, the renal papilla displayed
no apoptosis after the ischemic insult, so the presence of
numerous LRCs within a restricted area of the papilla base
and the rapidly-proliferating cells in the upper papilla (which
can migrate to other parts of the kidney more susceptible to
the low oxygen tension) evoke the architectural arrangementof the stem cell compartments of highly-regenerative organs
such as the epidermis. Stem cells are usually located in deep,
narrow tissue niches, where the proliferative phenomena
behind self-maintenance take place. The transient zone (rich
in amplifying precursor cells) and the differentiated cells in
various stages of maturation lie respectively in the progres-
sively more distal cell layers.
The stem cell niche as a functional entity
The concept of stem cell niche is changing. The mere
location of stem cells is not sufficient to define a niche,which must have both anatomical and functional dimen-
sions [39]. This issue is particularly important as new stem
cell sites come to light. Accumulating data have challenged
the conviction that heterologous cells must necessarily
occur in niches, suggesting that for some stem cells the
niche may consist of extracellular matrix and other non-
cellular constituents that could regulate their function [39].
Both paracrine and metabolic factors could serve function-
ally as a niche, which could also be seen as a dynamic
structure capable of being formed anew and responding to
exogenous signals via a sensing system possibly consisting
of the nervous or circulatory systems. Indeed, there is a
growing body of data to indicate the perivascular site as a
stem cell niche [4042]. Whether the components of the
vasculature are niche cells (i.e. cells interacting with stem
cells) or stem cells remains to be seen.
The perivascular mesenchymal stem cell niche hypothesis
Multipotent mesenchymal stromal cells (MSCs), typically
defined as adherent fibroblastoid cells capable of differen-
tiating into osteoblasts, adipocytes and chondrocytes in
vitro, have been found to reside within the connective tissue
of most organs, including the kidney, where they have been
isolated from glomeruli and the kidney as a whole [40].
Immunophenotyping indicates that MSC populations orig-
inating from different sources share numerous surface
markers, e.g. CD29, CD44, and express SMA, a vascular
smooth muscle cell marker, pointing to a relationship with
perivascular cells [43].
These findings have prompted the suggestion that MSCs
may derive from perivascular cells. Pericytes are good
candidates to represent the MSC population within organs [41].
In resting tissues, pericytes and endothelial cells (EC) are
quiescent, slow-cycling cells, but in the angiogenic stage
they show a highly-proliferative potential, a capacity for
self renewal, and the ability to generate daughter cells, thus
behaving like adult stem cells. Pericytes isolated from
different tissues display a marked plasticity and are able to
differentiate into osteoblasts, chondroblasts, fibroblasts,
pre-adipocytes [42]. It is also worth mentioning thatpericytes have been involved in vascular and ectopic
calcification [44]. That adult organ MSCs might be
pericytes or pericyte-like cells is also supported by the fact
that they can share some markers, such as CD146, 3G5
[45]. Taking these findings as a whole, we could conclude
that the MSC compartment extends through the post-natal
body as a result of its perivascular location.
The microvasculature of the renal papilla is particularly
rich in pericytes, subendothelial cells that regulate micro-
vascular integrity in the peritubular capillary network and
give the descending vasa recta (the arteriolar segments
supplying blood to the medulla) their contractile function.Thus in the papilla might reside that MSC compartment
linked to the perivascular niche. Mesenchymal stromal stem
cells have repeatedly been isolated from the kidney [14,
4649]. Very recently Lee et al [20] have presented
evidences that progenitor cells (MKPC) with mesenchymal
stromal stem cell properties reside in the mouse kidney
interstitium of the medulla and papilla in close association
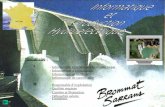
with endothelial cells. Indeed, all stem/progenitor cells
isolated from the papilla expressed markers of MSCs such
as CD 29 and showed positivity forSMA [5,6,20] which
is considered a typical marker of perycites pointing to a
possible relationship with papillary vascular pericytes [50]
(Fig. 2).
Could pericytes represent a subpopulation of these
MSCs in the kidney, and in the papilla in particular? Is
there an ancestor of the MSC natively associated with the
perivascular cells? Once again, the answer comes from
developmental biology.
Embryonic origin of stromal and vascular kidney cells
The mammalian kidney develops in three waves, only the last
of which (the metanephros) continues to exist as the adult
kidney. All three embryonic kidneys arise from the meso-
derm, one of the earliest tissues to develop in the embryo.
Nephrogenesis involves a carefully-controlled series of
morphogenic and differentiation events that start with the
interaction between two different primordial epithelial and
mesenchymal tissues both originating from the intermediate
mesoderm, i.e. the ureteric bud of Wolffian derivation grows
and invades the metanephric blastema. Factors secreted by the
ureteric bud induce this mesenchyme first to form clusters and
Stem Cell Rev and Rep (2010) 6:650657 653
-
7/26/2019 Anglani Et Al_2010
5/8
then to change into epithelium and the specialized structures
constituting the nephron. The induced mesenchyme in turn
sends signals back to the ureteric bud to make it divide and
grow (reviewed in [51]). This process of reciprocal induction
proceeds in an orderly manner, from the deep to the outer
cortex, producing branches of the collecting tree and neph-
rons, progressing from the glomerulus to the distal tubule.
The development of most tubular organs relies on signaling
between epithelial and mesenchymal stromal progenitor
populations. These two populations often derive from different
germ layers that are specified during gastrulation, well in
advance of organ condensation [52]. In kidney development,
however, the mesenchymal and epithelial lineages both derive
from the intermediate mesoderm. Moreover, the branching
morphogenesis of most tubular organs arises from pre-existing
epithelial sheets or tubules, whereas in the kidney not only do
the mesenchymal cells of metanephric blastema generate all
the epithelia of the nephron through mesenchymal-to-
epithelial transition (MET), they also drive the branching of
the ureteric bud. The metanephric blastema (also known as
metanephric mesenchyme) is composed of a non-
homogeneous population of cells that sends signals to the
Wolffian duct, which gives rise to the ureteric bud in response
[53]. One of the fundamental questions of kidney develop-
mental biology is how many cell lineages there are in the
metanephric blastema before and after it is induced by the
ureteric bud. The traditionally held view is that mesenchymal
cells that do not regain an epithelial state through MET may
differentiate and give rise to connective tissue and stromal
cells [54].
To date, the origin of renal stromal cells has remained
unknown, though there is some evidence of these cells
developing from a separate cell lineage within the meta-
nephric blastema [55]. Using fate mapping techniques,
Guillaume et al. [52] very recently demonstrated that large
populations of renal stromal cell originate from a different
part of the mesodermthe paraxial mesodermthus
indicating that renal development (like that of all other
tubular organs) depends on the integration of progenitors
from different embryonic tissues into a single rudiment. It is
noteworthy that bones, skeletal muscle and tendons
originate from paraxial mesoderm. In this light, the ability
of MSCs to differentiate into osteoblasts and chondrocytes
must be a commitment received in the very early
embryological stages.
During the reciprocal inductive stage of metanephric
development, two distinct regions of metanephric mesen-
chyme are morphologically distinguishable, i.e. the cap
mesenchymal cells, which are Pax2 positive and will form
nephrons; and the region peripheral to the cap mesenchyme,
where cells expressing Foxd1 may represent stromal progen-
itor cells, and cells that are Foxd1-negative, but Six2-, Gdnf-
and Cited1-positive, may be mesenchymal stem or progenitor
cells. When branching of the ureteric bud has begun and
nephron induction takes place, the stromal cells surrounding
the branches of the ureteric bud and the induced nephrons
Fig. 2 a The different stem cell
types isolated from the papillary
interstitium are indicated, fig-
ures were drawn from the
articles cited within parethesis. b
Histology of the renal papilla,
EE staining, 200x magnifica-
tion. c -smooth muscle stain-
ing of the renal papilla, 200X
magnification
654 Stem Cell Rev and Rep (2010) 6:650657
-
7/26/2019 Anglani Et Al_2010
6/8
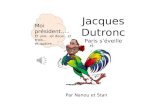
constitute the primitive interstitium [56] (Fig. 3). By late
gestation, a secondary interstitium is created with two distinct
populations, the cortical stroma and the medullary stroma,
which then differentiate to form the adult kidney interstitium,
with the cortical interstitium comprising fibroblasts and
lymphocyte-like cells, and the medullary interstitium mainly
comprising lipid-laden interstitial cells, lymphocyte-like cells
and pericytes [56,57].
From these studies, one might argue thatwhatever
their true origin (from the intermediate or paraxial meso-
derm)the mesenchymal stromal cells contain different
cell lineages, including the precursor of the vasculature.
Angioblasts (individual endothelial progenitors) are
integral to the development of the glomerular tuft, and they
are identified in the developing kidney because they
express typical vascular markers, such as vascular endo-
thelial growth factor receptor 2 (VEGFR2). Although
metanephric mesenchyme contains VEGFR2-positive cells
from the early stages of development, cross-species
transplantation studies have suggested that extrarenal cells
also contribute to the glomerular vasculature [58].
Mesoangioblasts are considered vessel-associated meso-
dermal stem cells. Originally identified in the mouse
embryonic aorta, similar but not identical cells have been
identified in postnatal vessels of several organs, such as the
skeletal muscle and heart. Interestingly, they have in common
the expression of endothelial and/or pericyte markers [59].
Mesangioblasts may be the ancestors of postnatal vessel-
associated progenitors, such as pericytes [60].
Taken together, these findings may indicate: 1) that MSCs
andpericytes are identical in that they have a common ancestor
and share the same phenotypic markers; 2) that the distribution
of MSCs throughout the body post-natally is related to their
existence in a perivascular niche; and 3) that interstitial MSCs
might reside in the microvasculature in the kidney papilla.
Conclusion
Our growing understanding of the cellular and molecular
mechanisms behind kidney regeneration and repair pro-
cessestogether with a knowledge of the embryonic origin
of renal cellsshould induce us to bear in mind that the
kidneys need for a real stem cell compartment is less
important than the cells phenotypic flexibility. One of the
major tasks of regenerative medicine will be to disclose the
molecular mechanisms underlying renal tubular plasticity
and to exploit its biological and therapeutic potential.
On the other hand, data are emerging that capillary and
microvessel walls all over the body may harbor a reserve of
MSCs; in the kidney, this might be located in the papilla.
The perivascular niche hypothesis fits well with the
evolving concept of the stem cell niche as an entity of
action. It is its dynamic capability that makes the niche
concept so important and essential to the feasibility of
regenerative medicine.
Acknowledgements This study was supported by Grant No.
CPDA085494 from the University of Padua.
Conflicts of interest The authors declare no potential conflicts of
interest.
Fig. 3 Schematic representation of renal development during em-
bryogenesis showing the different cellular components involved in theprocess of nephrogenesis and collecting duct branching. Figure is
based on Figure 4 in the Journal of Cellular and Molecular Medicine
by authors Anglani F, Forino M, Del Prete D, Tosetto E, TorregrossaR., DAngelo A [51]
Stem Cell Rev and Rep (2010) 6:650657 655
-
7/26/2019 Anglani Et Al_2010
7/8
References
1. Little, M. H. (2006). Regrow or repair: potential regenerative
therapies for the kidney. Journal of the American Society of
Nephrology, 17, 2390401.
2. Witzgall, R., Brown, D., Schwarz, C., & Bonventre, J. V. (1994).
Localization of proliferating cell nuclear antigen, vimentin, c-Fos,
and clusterin in the postischemic kidney. Evidence for a
heterogenous genetic response among nephron segments, and alarge pool of mitotically active and dedifferentiated cells. Journal
of Clinical Investigation, 93, 21752188.
3. Bonventre, J. V. (2003). Dedifferentiation and proliferation of
surviving epithelial cells in acute renal failure. Journal of the
American Society of Nephrology, suppl 1, S55S61.
4. Maeshima, A., Yamashita, S., & Nojima, Y. (2003). Identification
of renal progenitor-like tubular cells that participate in the
regeneration processes of the kidney. Journal of the American
Society of Nephrology, 14, 31383146.
5. Oliver, J. A., Maarouf, O., Cheema, F. H., Martens, T. P., & Al-
Awqati, Q. (2004). The renal papilla is a niche for adult kidney
stem cells. Journal of Clinical Investigation, 114, 795804.
6. Dekel, B., Zangi, L., Shezen, E., et al. (2006). Isolation and
characterization of non tubular sca-1 + lin- multipotent stem/
progenitor cells from adult mouse kidney. Journal of theAmerican Society of Nephrology, 17, 33003314.
7. Gupta, S., Verfaillie, C., Chmielewski, D., et al. (2006). Isolation
and characterization of kidney-derived stem cells. Journal of the
American Society of Nephrology, 17, 30283040.
8. Poulsom, R., Alison, M. R., Cook, T., et al. (2003). Bone marrow
stem cells contribute to healing of the kidney. Journal of the
American Society of Nephrology, suppl 1, S48S54.
9. McTaggart, S. J., & Atkinson, K. (2007). Mesenchymal stem
cells: immunobiology and therapeutic potential in kidney disease.
Nephrology, 12, 4452.
10. Little, M. H., & Bertram, J. F. (2009). Is there such a thing as a
renal stem cell? Journal of the American Society of Nephrology,
20, 21122117.
11. Hishikawa, K., Marumo, T., Miura, S., Nakanishi, A., Matsuzaki,
Y., & Shibata, K. (2005). Musculin/MyoR is expressed in kidneyside population cells and can regulate their function. The Journal
of Cell Biology, 169, 921928.
12. Challen, G. A., Bertoncello, I., Deane, J. A., Ricardo, S. D., &
Little, M. H. (2006). Kidney side population reveals multilineage
potential and renal functional capacity but also cellular heterogene-
ity. Journal of the American Society of Nephrology, 17, 18961912.
13. Lazzeri, E., Crescioli, C., Ronconi, E., et al. (2007). Regenerative
potential of embryonic renal multipotent progenitors in acute renal
failure.Journal of the American Society of Nephrology, 18, 3128
3138.
14. Sagrinati, C., Netti, G. S., Mazzinghi, B., et al. (2006). Isolation
and characterization of multipotent progenitor cells from the
Bowmans capsule of adult human kidneys. Journal of the
American Society of Nephrology, 17, 24432456.
15. Bruno, S., Bussolati, B., Grange, C., et al. (2009). Isolation and
characterization of resident mesenchymal stem cells in human
glomeruli.Stem Cells and Development, 18, 867880.
16. Bussolati, B., Bruno, S., Grange, C., et al. (2005). Isolation of
renal progenitor cells from adult human kidney. The American
Journal of Pathology, 166, 545555.
17. Kitamura, S., Yamasaki, Y., Kinomura, M., et al. (2005).
Establishment and characterization of renal progenitor like cells
from S3 segment of nephron in rat adult kidney. The FASEB
Journal, 2005(19), 17891797.
18. Yamashita, S., Maeshima, A., & Nojima, Y. (2005). Involvement
of renal progenitor tubular cells in epithelial-to-mesenchymal
transition in fibrotic rat kidneys. Journal of the American Society
of Nephrology, 16, 20442051.
19. Markovc-Lipkovsky, J., Muller, C. A., Klein, G., et al. (2007).
Neural cell adhesion molecule expression on renal interstitial
cells.Nephrology, Dialysis, Transplantation, 22, 15581566.
20. Lee, P. T., Lin, H. H., Jiang, S. T., et al. (2010). Mouse kidney
progenitor cells accelerate renal regeneration and prolong survival
after ischemic injury. Stem Cells, 28(3), 57384.
21. Ito, M., Liu, Y., Yang, Z., et al. (2005). Stem cells in the hair
follicle bulge contribute to wound repair but not to homeostasis ofthe epidermis. Natural Medicines, 2005(11), 13511354.
22. Crosby, H. A., & Strain, A. J. (2001). Adult liver stem cells: bone
marrow, blood, or liver derived? Gut, 48, 153154.
23. Vogetseder, A., Karadeniz, A., Kaissling, B., & Le Hir, M. (2005).
Tubular cell proliferation in the healthy rat kidney. Histochemistry
and Cell Biology, 124, 97104.
24. Vogetseder, A., Palan, T., Bacic, D., Kaissling, B., & Le Hir, M.
(2007). Proximal tubular epithelial cells are generated by division
of differentiated cells in the healthy kidney. American Journal of
Physiology. Cell Physiology, 292, C807C813.
25. Vogetseder, A., Picard, N., Gaspert, A., Walch, M., Kaissling, B.,
& Le Hir, M. (2008). The proliferation capacity of the renal
proximal tubule involves the bulk of differentiated epithelial cells.
American Journal of Physiology. Cell Physiology, 294, C22C28.
26. Humphreys, B. D., Valerius, M. T., Kobayashi, A., et al. (2008).
Intrinsic epithelial cells repair the kidney after injury. Cell Stem
Cell, 2, 284291.
27. Lin, F., Moran, A., & Igarashi, P. (2005). Intrarenal cells, not bone
marrow-derived cells, are the major source for regeneration in
postischemic kidney.Journal of Clinical Investigation, 115, 1756
1764.
28. Anglani, F., Ceol, M., Mezzabotta, F., et al. (2008). The renal stem
cell system kidney repair and regeneration. Frontiers in Biosci-
ence, 13, 63956405.
29. Zavadil, J., & Bttinger, E. P. (2005). TGF-beta and epithelial-to-
mesenchymal transitions. Oncogene, 24, 57645774.
30. Kalluri, R., & Weinberg, R. A. (2009). The basic of epithelial-
mesenchymal transition. Journal of Clinical Investigation, 119,
14201428.
31. Perez-Pomares, J. M., & Munoz-Chapuli, R. (2002). Epithelial-
mesenchymal transition: A mesodermal cell strategy for evolutive
innovation in metazoans. The Anatomical Record, 268, 343351.
32. Acloque, H., & Adams, M. S. (2009). Epithelial-mesenchymal
transition: the importance of changing cell state in development
and disease. Journal of Clinical Investigation, 119, 14381449.
33. Hay, E. D. (1968). Organization and fine structure of epithelium
and mesenchyme in the developing chick embryo. In R.
Fleischmajer & R. E. Billingham (Eds.), Epithelial-mesenchymal
interactions(pp. 3155). Baltimore: Williams and Wilkins.
34. Gilbert, S. F. (1995). Developmental biology (p. 894). Sunderland:
Sinauer Associates.
35. Mani, S. A., Guo, W., Liao, M. J., et al. (2008). The epithelial-
mesenchymal transition generates cells with properties of stem
cells. Cell, 133(4), 704
15.36. Swetha, G., Chandra, V., Phadnis, S., & Bhonde, R. (2009).
Glomerular parietal epithelial cells of adult murine kidney
undergo EMT to generate cells with traits of renal progenitors. J
Cell Mol Med. Oct 16 [Epub ahead of print]
37. Bianchi, G., Muraglia, A., Daga, A., Corte, G., Cancedda, R., &
Quarto, R. (2001). Microenvironment and stem properties of
bone-marrow derived mesenchymal cells. Wound Repair and
Regeneration, 9, 460466.
38. Oliver, J. A., Klinakis, A., Cheema, F. K., et al. (2009).
Proliferation and migration of label-retaining cells of the kidney
papilla. Journal of the American Society of Nephrology, 20(11),
23152327.
656 Stem Cell Rev and Rep (2010) 6:650657
-
7/26/2019 Anglani Et Al_2010
8/8
39. Scadden, D. T. (2006). The stem-cell niche as an entity of action.
Nature, 441, 10751079.
40. da Silva Meirelles, L., Chagastelles, P. C., & Nardi, N. B. (2006).
Mesenchymal stem cells in virtually all post-natal organs and
tissues.Journal of Cell Science, 119, 22042213.
41. Crisan, M., Yap, S., Casteilla, L. A., et al. (2008). A perivascular
origin for mesenchymal stem cells in multiple human organs. Cell
Stem Cell, 3, 301313.
42. Diaz-Flores, L., Gutirrez, R., Madrid, J. F., et al. (2009).
Pericytes. Morphofunction, interaction and pathology in aquiescent and activated mesenchymal cell niche. Histol Histo-
patol, 24, 909969.
43. Phinney, D. G., & Prockop, D. J. (2007). Concise review:
mesenchymal stem/multipotent stromal cells: the state of trans-
differentiation and modes of tissue repaircurrent views. Stem
Cells, 25, 28962902.
44. Johnson, R. C., Leopold, J. A., & Loscalzo, J. (2006). Vascular
calcification: pathobiological mechanisms and clinical implica-
tions.Circulation Research, 99, 10441059.
45. Covas, D. T., Panepucci, R. A., Fontes, A. M., et al. (2008).
Multipotent mesenchymal stromal cells obtained from diverse
human tissues share functional properties and geneexpression
profile with CD146+ perivascular cells and fibroblasts. Experi-
mental Hematology, 36, 642654.
46. Plotkin, M. D., & Goligorsky, M. S. (2006). Mesenchymal cells
from adult kidney support angiogenesis and differentiate into
multiple interstitial cell types including erytropoietin-producing
fibroblast. American Journal of Physiology-Renal Physiology,
291, F902F912.
47. Chen, J., Park, H. C., Addabbo, F., et al. (2008). Kidney-derived
mesenchymal stem cells contribute to vasculogenesis, angiogen-
esis and endothelial repair. Kidney International, 74, 879889.
48. Patschan, D., Michurina, T., Shi, H. K., et al. (2007). Normal
distribution and medullary-to-cortical shift of Nestinexpressing
cells acute renal ischemia. Kidney International, 71, 744754.
49. Huang, Y., Johnston, P., Zhang, B., et al. (2009). Kidney-derived
stromal cells modulate dendritic and T cell responses. Journal of
the American Society of Nephrology, 20, 831841.
50. Park, F., Mattson, D. L., Roberts, L. A., & JR, C. A. W. (1997).
Evidence for the presence of smooth muscle -actin within
pericytes of the renal medulla. Am J Physiol Regulatory
Integrative Comp Physiol, 273, 17421748.
51. Michos, O. (2009). Kidney development: from ureteric bud formation
to branching morphogenesis.Current Opin Genet Dev, 19, 484490.
52. Guillaume, R., Bressan, M., & Herzlinger, D. (2009). Paraxialmesoderm contributes stromal cells to the developing kidney.
Developmental Biology, 329, 169175.
53. Anglani, F., Forino, M., Del Prete, D., Tosetto, E., Torregrossa, R.,
& DAngelo, A. (2004). In search of adult renal stem cells.
Journal of Cellular and Molecular Medicine, 8, 474487.
54. Ekblon, P., & Weller, A. (1991). Ontogeny of tubular interstitial
cells. Kidney International, 39, 394400.
55. Al-Awati, Q., & Oliver, J. A. (2002). Stem cells in the kidney.
Kidney International, 61, 387397.
56. Dressler, R. D. (2009). Advances in early kidney specification,
development and patterning. Development, 136, 38633874.
57. Cullen-McEwen, L. A., Caruana, G., & Bertran, J. F. (2005). The
where, what and why of the developing renal stroma. Experimen-
tal Nephrology, 99, e1e8.
58. Vaughan, M. R., & Quaggin, S. E. (2008). How do mesangial and
endothelial cells form glomerular tuft. Journal of the American
Society of Nephrology, 19, 2433.
59. Tonlorenzi, R., Dellavalle, A., Schnapp, E., Cossu, G., &
Sampaolesi, M. (2007). Isolation and characterization of meso-
angioblasts from mouse, dog and human tissue. Curr Proc Stem
Biol, chapter 2:unit 2B.1.
60. Brunelli, S., Tagliafico, E., De Angelis, F. G., et al. (2004). Msx2
and necdin combined activities are required for smooth muscle
differentiation in mesoangioblast stem cells.Circulation Research,
94, 15711578.
Stem Cell Rev and Rep (2010) 6:650657 657