34 IM.&DI“ENTS ET ALIMEWTS L’APPROCHE …
9
34 IM.&DI“ENTS ET ALIMEWTS : L’APPROCHE ETHNOPHARMACOLDGIQUE TUSCHJNSKY Christine Institut für Ethnologie, Hamburg University Rothenbaumchaussee 64a, D-20148 Hamburg Germany RllSUïVÉ Les jumu (phytomkdicaments malais) sont populaires chez les Malais et sont connus depuis des siêcles. La conception pharmaceutique non occidentale du jamu a ses propres implications culturelles et sociales, en relation avec l‘humorisme, la philosophie et la religion des Malais. A Singapour,les jmnu connaissent une situation spkciale,entre une vision occidentale et Sud-Est asiatique du monde, entre les standards de la science occidentale et la tradition malaise. Les efforts pour << traduire >> le concept de jumu dans l’un de ceux de la pharmacie moderne sont vouks l’Cchec, car ces concepts ne sont pas compatibles. The following article on Malay phytopharmaceuticals (jawzu) is based on an anthropological field study conducted in the Malay community in Singapore in 1989/90 (TUSCHINSKY 1992), and a short follow-up in 1993. It does not examine pharnlaceuticalbut cultural and social aspects of janzu within the three spheres of production, trade and consumption, which are the constituting elements in the “biograpky of a drug” (v.d. GEEST 1988). THE VARIETY QF JAMU m SEVGAPQ~ Interest in non-Western pharmaceuticals has risen in the last decade, as has been the case with Southeast-Asian ‘L~CIIF~U’’. Jamu is the Imdonesian and Malay term for traditional phar- maceuticalsmade from fresh or dried medicinalplants. These remedies have existed for centuries, and are popular among the Malays’ throughout the Malayan Archipelago (Malay- sia, Singapore, Brunei Darussalam, Indonesia). This region is rich in medicinal plants, which are cultivated in gardens and plantations in addition to growing naturally alongside other indigenous vegetation. The flowers, leaves, fruits, bark, Wood and roots of these plants are prepared in different manners: Jamu can be an infusion of fresh or dried herbs, a mixture of dried pIants, or a combination of dried and pow- dered medicinal plants. Most recipes are compositions of up to 40 different elements. General folklore attributes the origins of jamu to Java’s prin- cipal courts, and today it continues to be primarily associated with Indonesia. In the traditional way, jarnu is produced at home to provide to friends and relatives. As a means of supple- menting family income, female family members often sel1 the surplus to neighbours or villagers; these ‘Ljmzu wornen” continue to be a familiar sight in Indonesian streets. Much like Street peddlers, jamu women wander through villages and cities, offering the contents of their jarnu gendong (jarnu car- ried on the back) to regular clientde. At the beginning of the 20th century, jarnu production un- derwent a significant transition. Innovative Indonesian entrepreneurs began producing home-made jamu for com- mercial sale, and the profits generated from this prosperous cottage industry initiated a series of events which led to today’s modern jamu industry. The pioneering businessmen transformed themselves and their heirs into what are today some of the world’s largestjumu producers, such as “Jamu Jago”, “Air Mancur” or “Nyonya Meneer”. These firms op- erate along modem management lines, and are oriented to Western pharmaceutical industry standards. Today, jamu is sold in various foms: ointments, oils, tonics or compresses are usually preferred for external use; powders, tablets, pills, tonics and capsules are used for more popular internal medi- cations, being considered as an important factor in every- day health care. More than 350 factories of varying sizes Actes du Colloque Europ&n d‘Ethnophammcologie et de la Ile ConErence internationale d’Ethnom&decine, Heidelberg, 24-27 mars 1993.
Transcript of 34 IM.&DI“ENTS ET ALIMEWTS L’APPROCHE …

34 IM.&DI“ENTS ET ALIMEWTS : L’APPROCHE ETHNOPHARMACOLDGIQUE
TUSCHJNSKY Christine Institut für Ethnologie, Hamburg University
Rothenbaumchaussee 64a, D-20148 Hamburg Germany
RllSUïVÉ Les jumu (phytomkdicaments malais) sont populaires chez les Malais et sont connus depuis des siêcles. La conception pharmaceutique non occidentale du jamu a ses propres implications culturelles et sociales, en relation avec l‘humorisme, la philosophie et la religion des Malais.
A Singapour, les jmnu connaissent une situation spkciale, entre une vision occidentale et Sud-Est asiatique du monde, entre les standards de la science occidentale et la tradition malaise. Les efforts pour << traduire >> le concept de jumu dans l’un de ceux de la pharmacie moderne sont vouks l’Cchec, car ces concepts ne sont pas compatibles.
The following article on Malay phytopharmaceuticals (jawzu) is based on an anthropological field study conducted in the Malay community in Singapore in 1989/90 (TUSCHINSKY 1992), and a short follow-up in 1993. It does not examine pharnlaceutical but cultural and social aspects of janzu within the three spheres of production, trade and consumption, which are the constituting elements in the “biograpky of a drug” (v.d. GEEST 1988).
THE VARIETY QF JAMU m S E V G A P Q ~ Interest in non-Western pharmaceuticals has risen in the last decade, as has been the case with Southeast-Asian ‘L~CIIF~U’’. Jamu is the Imdonesian and Malay term for traditional phar- maceuticals made from fresh or dried medicinal plants. These remedies have existed for centuries, and are popular among the Malays’ throughout the Malayan Archipelago (Malay- sia, Singapore, Brunei Darussalam, Indonesia). This region is rich in medicinal plants, which are cultivated in gardens and plantations in addition to growing naturally alongside other indigenous vegetation. The flowers, leaves, fruits, bark, Wood and roots of these plants are prepared in different manners: Jamu can be an infusion of fresh or dried herbs, a mixture of dried pIants, or a combination of dried and pow- dered medicinal plants. Most recipes are compositions of up to 40 different elements.
General folklore attributes the origins of jamu to Java’s prin- cipal courts, and today it continues to be primarily associated with Indonesia. In the traditional way, jarnu is produced at home to provide to friends and relatives. As a means of supple- menting family income, female family members often sel1 the surplus to neighbours or villagers; these ‘Ljmzu wornen” continue to be a familiar sight in Indonesian streets. Much like Street peddlers, jamu women wander through villages and cities, offering the contents of their jarnu gendong (jarnu car- ried on the back) to regular clientde. At the beginning of the 20th century, jarnu production un- derwent a significant transition. Innovative Indonesian entrepreneurs began producing home-made jamu for com- mercial sale, and the profits generated from this prosperous cottage industry initiated a series of events which led to today’s modern jamu industry. The pioneering businessmen transformed themselves and their heirs into what are today some of the world’s largestjumu producers, such as “Jamu Jago”, “Air Mancur” or “Nyonya Meneer”. These firms op- erate along modem management lines, and are oriented to Western pharmaceutical industry standards. Today, jamu is sold in various foms: ointments, oils, tonics or compresses are usually preferred for external use; powders, tablets, pills, tonics and capsules are used for more popular internal medi- cations, being considered as an important factor in every- day health care. More than 350 factories of varying sizes
Actes du Colloque Europ&n d‘Ethnophammcologie et de la Ile ConErence internationale d’Ethnom&decine, Heidelberg, 24-27 mars 1993.

MEDICAUENTS ET ALIMENTS :‘L’APPROCHE ETHNOPHARMACOLOGIQUE H 35
are registered in Indonesia, and their product is exported to several countries, the largest consumer market being in Malaysia and Singapore (AFDHALmLSCH 1988). Indonesia continues to be the trend-setter in jamu production, development and marketing. Jamu’s industrialisation has af- fected not only its outer appearance, but also the increasingly modern strategies used to sell it. This latter factor has played a significant role in changing jamu’s image from that of an old-fashioned medicinal plant treatment to a natural remedy with “ancestral heritage”, now also fitting into the Western back-to-nature trend. Janzu’s profit-generating potential be- came so significant that by the early 1980s, there was discus- sion in Indonesia about jamu becoming the most important non tnigas (non petrollnon gas) source of revenue for the coun- try (SIMANDJUNTAK 1984). Dreams of profitable export to the West have not yet been realised, however. In Singapore, the majority of all jarnu sold is imported from Indonesia, a minority is imported from Malaysia, and a very limited amount of jamu are produced in Singaporean home manufactures using little machinery and manually-intensive processes. When people in Singapore talk about jamu, they usually refer to the Indonesian products described above; but the term is often used to describe a macro-category, which includes many other varieties of Malay phytopharmaceuticals. Akar-akar kayu (literally: wooden roots; i.e. the cleaned and roughly chopped up raw ingredients used for infusions) is one example of jamu included in the macro-category, but perhaps the most important variety is rnajun (also majon, ma’jun, makjon), which is either imported from Malaysia or produced in Singapore. The original meaning of this Arabic term is “paste” or “cream”, but in general majun refers to a “com- pounded medicine” (WILKINSON 1959), “kneaded” and “of floury material” (WILKINSON 1985/1903). The main difference between jamu and majun is the form: janzu was originally sold in powder form, with pills, tablets and capsules being the result of modern development and commercialisation. Majun, in contrast, has the form of a large soft pill which is comparable in size and shape to a large black olive. In principle, the plant compositions are quite similar, but unlike jamu the powdered ingredients of majun are cooked, then kneaded with honey and beef fat and formed into the olive-like pills. Majun is rarely sold in singular form, and typi- cally ten to fifteen pills are packed in plastic containers. Re- cently, majun has also been produced in capsule form, containing the same powdered plant ingredients.
The term majun is known in Bahasa Indonesia as well and can even be found in Old-Javanese dictionaries (ZOET- MULDER 1982; MARDIWARSITO 1981). Yet nzajun is not known to come from Indonesia in pi11 form, where the term is only used to specify a certain kind of jamu, and thus describes the purpose rather than the form or shape. In Indonesia, jumu-
jamu majun are special medicines for the strengthening of male vitality (Air Mancur Catalogue). This purpose, however, is not contradictory with that of the Malaysian or Singaporean majun. Although it can also be taken by women, there is a clear delineation: majun is more for men, jumzc more for women. Only a few jamu come from Malaysia, whose products in- clude majun, akar-akar kayu, oils or ointments. According to the statement of a well-informed Singaporean jamu trader, the few attempts to develop an industry similar to Indonesia’s in Malaysia have been unsuccessful. In this article the term jamu is used as a super-category com- prising all varieties of Malay phytopharmaceuticals and will be specified only when necessary.
STRATEGIES IN SINGAPOREAN JAMU PRODUCTION AND TRADE A number of Malay people in Singapore are familiar with use and production of jarnu and are still knowledgeable about many medicinal plants (YUSOF 1987/88). Often they supply jarnu to relatives and friends, and sometimes they sell their products to small shops or market stalls. In spite of strict regu- lations in Singapore, jamu is often sold without any packag- ing descriptions whatsoever. The ingredients, producer, place of production, and sometimes even product name are often completely absent - they are simply known to all. In Singapore there exist only three producers which sell their products professionally either out of the home or through a shop or market stalls. Some businessmen specialise strictly in selling and are completely removed from the production process; three run specialised jamu shops, while others oper- ate strictly as agents. The 80- 100 small to moderate-sized jamu shops and stalls whose product range is not limited to Malay pharmaceuticals are supplied by three wholesalers.
Singapore’s production and marketing of jamu is compara- tively rudimentary. The professional jamzl business only started at the beginning of the 1980s, while Indonesian f i s have long been working with successful marketing strategies and continue to develop new ones. Singapore is exposed to the influences of neighbouring coun- tries, and a mixture of these features can be found in jamu marketing. Singapore jamu traders have, of course, al1 the marketing venues available of a modern City, and they make use of advertisements in newspapers and broadcast media. But these means are not as important as one would expect, and the informal word-of-mouth information provided by rela- tives, friends or jamu sellers is still an integral part of sale strategies. Some f m s have employed house-to-house sell- ers, Who serve as knowledgeable health care and cosmetic consultants - a role somewhere in between the traditional
Actes du 2e Colloque Européen d‘Ethnopharmacologie et de la 1 le Conférence internationale d‘Ethnomédecine, Heidelberg, 24-27 mars 1993.

36 I M~~DICAMENTS ET ALIMENTS : L’APPROCHE ETHiVOPHARA4ACOLOGlQVE
“janzu woman” and the counter salespeople in the European and American cosmetic industries. In 1992, the first small stall serving ready-to-drinkjanzu by a Malay lady was opened in “Geylang”, a Malay dominated quarter. Its design is a com- bination of store and ba - a lcind of “Jarnuteria”, which has been cornmonplace in many parts of Indonesia for several years. In spite of having alrnost no knowledge about their prod- ucts, al1 sales executives in Singaporean jamu outlets have a consulting role, too. Usually they need only read aloud the packaging inscriptions, but consumers expect some service from the selling individual.
The more important sale strategies and the creation and imple- mentation of product images become clexer on examination of the target consumer group. Jamu is popular among the Malays, who consider thesselves to be the true indigenous inhabitants of Singapore, in spite of the fact that the Malay population base has been steadily decreasing since the begin- ning of the 19th century (strict Singapore immigration laws instituted in 1965 stopped the immigrant influx). The ethnie breakdown of Singapore has changed only slightly over the last twenty years, and now stands at 76% Chinese, 15% Malays and 8% Indians. The 400,000 people Who make up the Malay community today have roots throughout the Malayan Archi- pelago (especially Bali, Java, Sulawesi, Bawean and Malay- sia), and they have maintained strong cultural and kinship links extending far beyond the state boundaries. The different Malay groups who emigrated to Singapore were ethnically
quite similar, and they intermingled quicldy with other Malays to form a distinct community with a high sense of community identification (BEDLINGTON 1974). Many have been living in Singapore for several generations, and the differences of geographic origin have seemingly lost any real signifieance. Malays often express the feeling of being an ethnie minority in their “own” country. in general they have a lower educa- tional and socio-economical status than the Chinese Major- ity, and almost no political influence: Malays are frequently labelled as “lagging behind” (BACH 1991). The Malay community defines itself with a common set of cultural val- ues and customs, its language (Malay), and by the same community-strenghtening religion (Islam).
In Singapore’s social and political context, this last criterion has turned out to be the most important defining element, and the influence of religion is prevalent at the retail level of Malay phannaceuticals. Jarnzr is only one segment of the goods of- fered at most of the 80-100 small and moderate-sized jamt shops and stalls; religious paraphernalia are also staple items, including praying carpets, a wide range of Islamic clothes and books, Islamic art, stickers with Koran verses and some- times hala1 food (prepared according to Islarnic rules). These shops are eoncentrated in predominantly Malay areas, but can also be found al1 over the City.
The religious embedding of jamu is also apparent in some of the corresponding product names. “Jamu Arab”, for instance,
Fig. P The term jarnu as both a self-reliant expression and a super-category
MASUN
I (IndonesiadMalay) (Arabie: paste) (IndonesiadMalay: originally from kneaded, compounded tree’s roots) dried fresh or dried medicine in form and roughly ehopped medicinal plants of big, soft, black medieinal plants
olive-like pills for infusions
since the beginning reeently also in of the 28th century form of eapsules in fortm of powder, nonpowdered pills, tonics, paste mixtures paste, capsules I
e.g. ubit periuk but alss some other
(trend to a uniform outer appearance of highly processed jamu products)
Actes du 2e Colloque Européen d’Ethnopharmacologie et de la 1 le Confc5rence internationale d‘Ethnomédecine. Heidelberg, 24-27 mars 1993.
MÉDICAMENTS ET ALIMENTS : L’APPROCHE ETHNOPHARMACOLOGIQUE m 37
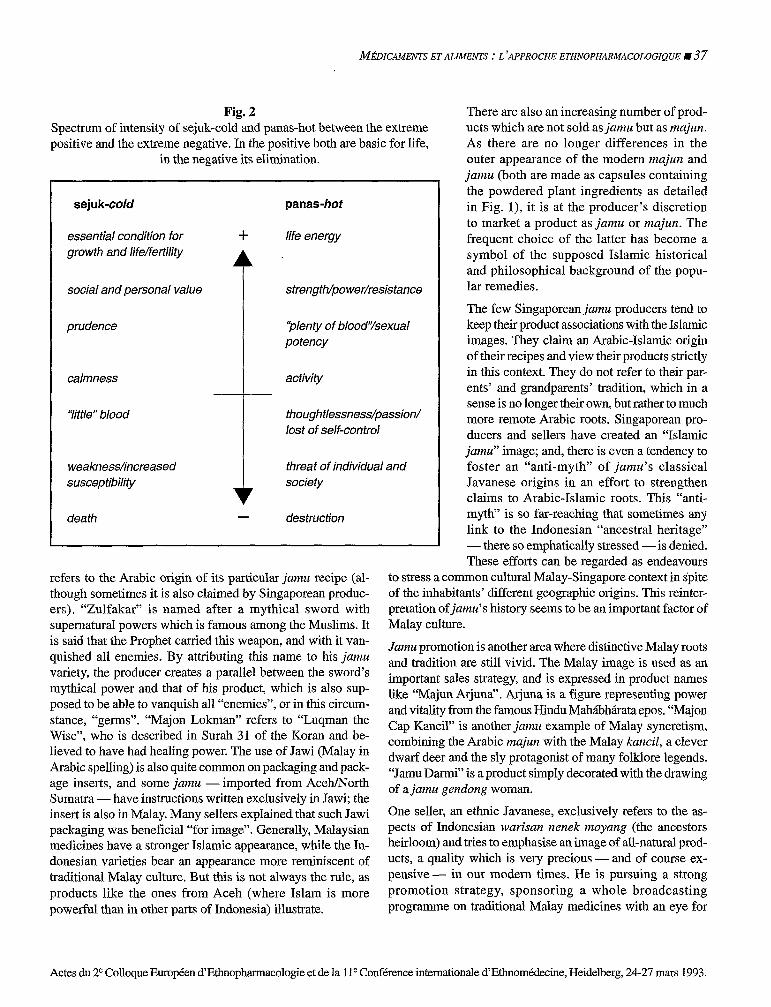
Fig. 2 Spectrum of intensity of sejuk-cold and panas-hot between the extreme positive and the extreme negative. In the positive both are basic for life,
in the negative its elimination.
sejuk-cold
essenfial condition for + growth and life/ferti/ity
social and persona1 value
prudence
calmness
Yitfle” blood
weaknesshncreased susceptibilify
death -
panas-hot
life energy
sfrengfh/power/resisfance
‘plenty of blood‘/sexual potency
activity
fhoughtlessness/passion/ lost of self-control
threat of individual and Society
destruction
refers to the Arabic origin of its particular jamu recipe (al- though sometimes it is also claimed by Singaporean produc- ers). “Zulfakar” is named after a mythical sword with supernatural powers which is famous among the Muslims. It is said that the Prophet carried this weapon, and with it van- quished al1 enemies. By attributing this name to his jamu variety, the producer creates a parallel between the sword’s mythical power and that of his product, which is also sup- posed to be able to vanquish al1 “enemies”, or in this circum- stance, “germs”. “Majon Lokman” refers to “Luqman the Wise”, Who is described in Surah 31 of the Koran and be- lieved to have had healing power. The use of Jawi (Malay in Arabic spelling) is also quite common on packaging and pack- age inserts, and some jamu - imported from Aceh/North Sumatra -have instructions written exclusively in Jawi; the insert is also in Malay. Many sellers explained that such Jawi packaging was beneficial “for image”. Generally, Malaysian medicines have a stronger Islamic appearance, while the In- donesian varieties bear an appearance more reminiscent of traditional Malay culture. But this is not always the rule, as products like the ones from Aceh (where Islam is more powerful than in other parts of Indonesia) illustrate.
There are also an increasing number of prod- ucts which are not sold as jamu but as maj~m. As there are no longer differences in the outer appearance of the modern majltn and jantu (both are made as capsules containing the powdered plant ingredients as detailed in Fig. l), it is at the producer’s discretion to market a product as jamu or majun. The frequent choice of the latter has become a symbol of the supposed Islamic historical and philosophical background of the popu- lar remedies.
The few Singaporean jamu producers tend to keep their product associations with the Islamic images. They claim an Arabic-Islamic origin of theù recipes and view their products strictly in this context. They do not refer to their par- ents’ and grandparents’ tradition, which in a sense is no longer their own, but rather to much more remote Arabic roots. Singaporean pro- ducers and sellers have created an “Islamic jamu” image; and, there is even a tendency to foster an “anti-myth” of jamu’s classical Javanese origins in an effort to strengthen claims to Arabic-Islamic roots. This “anti- myth” is so far-reaching that sometimes any link to the Indonesian “ancestral heritage” - there so emphatically stressed - is denied. These efforts can be regarded as endeavours
to stress a common cultural Malay-Singapore context in spite of the inhabitants’ different geographic origins. This reinter- pretation of jamu’s history seems to be an important factor of Malay culture.
Jamu promotion is another area where distinctive Malay roots and tradition are still vivid. The Malay image is used as an important sales strategy, and is expressed in product names like “Majun Arjuna”. Arjuna is a figure representing power and vitality fiom the famous Hindu Mahiibhkata epos. “Majon Cap Kancil” is another janm example of Malay syncretism, combining the Arabic rnajun with the Malay kaancil, a clever dwarf deer and the sly protagonist of many folklore legends. “Jamu Darmi” is a product simply decorated with the drawing of a jarnu gendong woman.
One seller, an ethnic Javanese, exclusively refers to the as- pects of Indonesian warisan nenek moyang (the ancestors heirloom) and tries to emphasise an image of dl-natural prod- ucts, a quality which is very precious - and of course ex- pensive- in Our modern times. He is pursuing a strong promotion strategy, sponsoring a whole broadcasting programme on traditional Malay medicines with an eye for
Actes du 2e Colloque Européen d’Ethnopharmacologie et de la 11“ Conférence internationale d’Ethnomédecine, Heidelberg, 24-27 mars 1993.

38 H MÉDICAMENTS ET ALIMENTS : L ?APPROCHE ETHNOPHARMACOLOGIQUE
eventually exporting to Japan. It is clear that an Islamic jamu image would not serve his purposes.
PRINCIPLES OF JAMU MEDICATIQN ANI9 THEIR SOCIAL I€WPLICATIONS Janzu is not a pharmaceutical in the Western sense: it is food supplement, prophylactic and curative remedy al1 in one. Jamu concentrates on certain aspects and interrelationships which Western medicine does not take as seriously: the notion of “care“ and “therapy”, for example, are not lcept as separate as they are in Western medicine. It is believed that keeping healthy also necessitates staying beautiful and attractive as long as possible - a perspective that might more generally be appreciated as the macrocosm reflecting the microcosm; the outer appearance reflecting or expressing the inner quali- ties. Cosmetics and the use of general tonics or aphrodisiacs are very popular, and have considerable stature in jamu medi- cine. It is not surprising that women represent the majority of jamu consumers and customers. since they have primarily responsibility for the health and well-being of their families in addition to being concerned about maintaining their appearance along the traditional norms of beauty. The qualities and effects of jamu are embedded in the widely discussed principles of the Malay humoral systern (HART
MAEaJ 1987; MANDERSON 1987; TUSCHINSICY 1992). balancing between the poles of hot (Mal. pa~tas) and cold (Mal. sejuk). In Malay humoral theory, both poles are essen- tials of a healthy and satisfactory life: neither of the poles is exclusively positive or negative, and the qualities of hot and cold are not just health indicators, they imply individual and social values.
Jmnu is used to treat usual bodily complaints and health dis- turbances indicating an imbalanced humoral condition, but the qualities and effects of the jamu variety is not as well distributed between hot and cold as one might expect. There are very few cooling jamu: so few, in fact, that the idea of a cooling jamu incited considerable amusement in Singapore’s Malay respondents. Months after the initial inquiries about cooling jamzt, many still asked laughing “Well, did you find your cooling jarnu?’, convinced such a search was futile. There are, however, a limited number of coolingjamu; sariawan is used for the treatment of “inner heat” and lip blisters, and somejamu exist to impiove the conditions for pregnancy, since coolness and humidity are seen as basic conditions for fertility and begetting.
Jamzt consumers and producers in Shgapore are more con- cerned about keeping heat in the body than suffering from too much heat. According to Malay healers, it is easy to cool somebody: “This is no problem, you just have to drink water
1969; LADEMAN 1981; MANDERSON 1981; LADER-
or eat papaya. But to “give heat” is very diffkult.” - “Ifsome- thing is cold, it is no medicine”, offered a Malay woman who produced j amt at home for her family. The cold threats are considered to come. from wind and rain, from constant work- ing in air-conditioned rooms, €rom energy-consuming activi- ties, but also from the process of ageing. Getting colder implicates a “loss of blood”, or by extension, of life energy. Jamu lcasih panas - jamu gives heat, if there is an increased need for it. But this particular jamu has other comnlon uses, since many consumers also believe it is a useful food supple- ment for people whose basic condition is ‘*hotter” than oth- ers. This is particularly true of men who are believed to be “hotter” than women. To keep their level of heat, they require a higher intake of hot jamu, and such beliefs are reflected in the existence of special product categories for men and women - an important part of the profitable jamu business. Women are supposed to avoid too much heat, and such jamu is forbidden for unmarried women; on the other hand, women must be “hot” enough - in any sense of the word - to be attractive. During pregnancy heat is considered to be danger- ous because it can induce an abortion, as the embryo needs coolness for growing. There is consequently also a waming on many jarnu packages: “Forbidden for pregnant women!” The hottest jamu are those used to increase male potency, often sold as majm. hfajurt is made of dried and powdered medicinal plants, which are roasted and nlixed with honey and beef oil. This procedure also increases the heat of the hot plants, and nzajttn is consequently a special product exclu- sively for men. Only old women who suffer from rheumatism are permitted to talce nmjzm, but in al1 other cases it is consid- ered too hot for them. “If women eat this, men will get prob- lems.. .”, jested a successful Singaporean jannt businessman. Heat is synonymous with life energy, potency, and power, and women should not have too rnuch of these qualities - or at least less than men. In this respect, the Malay humoral sys- tem and its hot-cold categorisation also serves as a stabilising factor for sexual hierarchy. This categorisation is meaningful not only in cornparisons between the sexes, but also between different ethnic groups. Singapore’s most dominant ethnic group is the Chinese, and as the biggest minority the Malays tallc frequently about the Chinese way of life and how it compares to their own. Bot11 share the principles of humoral medicine systems, albeit with some variations. Malay people, for instance, consider them- selves to be hotter than Chinese men and women, with al1 individual and social implications that the term “hot” entails. The Malay reasoning is as follows: they need more heat to maintain their hotter state, and consequently use more chili in their food, proving the hotter bodily state; for the same rea- son, they eat jarnu, since they have more temperament and passion and are more attractive. The Chinese medicines are
Actes du 2e Colloque Européen #Ethopharmacologie et de la I l e Confêrence internationale d’Ethnomêhcine, Heidelberg, 24-24 mars 1993.

MEDlCAMENTs ET ALIMENTS : L’APPROCHE ETHNOPHARMACOLOGIQUE I 39
also well-known among the Malays, but in general the Malays consider them too cold and therefore inappropriate. The op- posite is also supposed to be true of the Chinese, at least from the Malay perspective: Chinese people supposedly do not eat jamu, because it is too hot for them, such being the case be- cause they are colder people. Chinese women are in particu- lar said to be “colder” in al1 senses of the word, especially compared to the “hot-blooded” Malay women.
Malay men’s interest in increasing potency by using special jarnu seems to be surprisingly high. The topic arises in taks with jumu sellers and customers, in newspaper articles, and magazines. Many Young and healthy looking men enter the shops asking vendors for “special” products to strengthen male vitality. This initially seems to contradict the Malay male self- perception as strong and lively men (an opinion which is often expressed). But if one bears in mind that the necessary condi- tion for potency is heat, and that a high potency requires that a correspondingly high level of heat be maintained, the in- creased need for heat appears to be justified - particularly since sexual activity is heat-consuming.
When one considers al1 elements, the existence of a serious health - or potency - problem among Malay men seems to be very unlikely, despite conclusions one might draw from the high sales level of men’s jalnzd. The preoccupation with potency and the comparisons to the allegedly weaker Chi- nese men instead points to the social implications of heat: power and strength, which favour the Malays - perhaps not in the political context, but at least in an essentially personal and physical sense - and provides a feeling of strength and value. The humoral system fixes the limits of the ethnic group in positive categories, and not in stigmatising terms of weak- ness and inferiority as it is in the political context of Malay day-to-day experiences. In this respect, the hot-cold categorisation serves as a means of expressing power and in- dicating individual and social values.
PHARMACEUTICAL CONCEPTS IN THEJR CULTURAL CONTEXT In medical anthropology, a medical system is seen as part of the social, cultural andor cognitive system, including the ideas of health, illness and healing based on religion, philosophy and general world-views (WOODWARD 1985). There is con- sequently a clear connection between pharmaceuticals as an element of a medical system, and the cultural ideas behind the conception of the world. Western world-views can be very broadly characterised as individualistic; they are bound to the principles of linear thinking and the ideas of cause and effect, concentrating on the explanation of isolated phenomena at the micro level. By contrast, the Malay world-view, and in this generalisation the Southeast-Asian world-view, is sociocentric, embedded in the idea of microcosm in macro-
cosm, where every thing, plant, animal, human or spiritual being has its proper place; individual and social endeavours aim to maintain balance and harmony at al1 levels of exist- ence. In this philosophy,jamu plays its small part: It increases the amount of blood and of life energy, and keeps the blood flowing - a means of balancing the state of health between the poles of hot and cold.
The different concepts of medication reflect their different philosophical backgrounds. In general, Western pharmaceu- ticals are molecularly-defined active biological substances or mixtures of substances. The definition of phytopharmaceuti- cals has various levels: Ideally it is one molecularly-defined active substance of plant origin, which, once analysed, can also be synthetically produced. Many Western phytopharma- ceuticals made this way from complex to pure substances, and sometimes the origin falled into oblivion. Usually, these products are not regarded as phytopharmaceuticals any more.
Standardised phytopharmaceuticals represent the second im- portant category and are still considered to be “real” pharma- ceuticals: Lf scientists succeed in analysing the main active ingredient(s) of a plant, they are able to standardise the prod- uct, which means the amount of the active substance(s) is guar- anteed and always consistent. In nature, the amount differs in plants with regard to location, climate or way of cultivation. Entire plant extracts represent the third group of plant medi- cines, consisting both of complex compositions from several active substances and of elements which we cal1 “inactive” - meaning that the efficacy is not yet proven. Moreover, there are ingredients in many plants which are simply unknown. These products fall into a grey area of the Western concept of phar- maceuticals, since they do not fulfil all of its requirements. For example, unknown and “inactive” substances are avoided in Western pharmaceuticals, since they are considered superflu- ous or even dangerous. The basic principle is that one substance cures one symptom or symptom complex; the less ingredients, the less undesired effects, or so-called side-effects (ETKIN 1988). The single ingredients are chemically known, identifi- able and tested by repeated experimentation, with the idea of one cause and one effect being the underlying paradigm. Jamu represent a forth group of phytopharmaceuticals which - in this form - is not included in Western pharma- cology. These products are made of numerous medicinal plants, some recipes based on up to forty different varieties. Jurnu contain no extracts, but rather preparations of the entire plant, with al1 active, “inactive” and unknown substances including all fibrous material; this is true regardless of whether the jamu preparation is in the form of powder, pills, tablets or capsules. This fact explains the high amount ofjamu that has to be taken daily, i.e. 20-30 pills, and should not be mistaken as a high dosage.
Actes du 2e Colloque Européen d’Etlmopharmacologie et de la 1 le Confémce internationale d’Ethnomédecine, Heidelberg, 24-27 mars 1993.

40 IMÉDICAMENTS ET ALIMEIWS : L’APPROCHE ETHNOPHARM4COLOGIQUE
In this pharmaceutical concept of janzu, fiequently criticised as “old-fashioned and unscientific” from Western point of view, the correspondmg Malay world-view becomes clear: the most important “ingredient” is the abundance of medicial plants with al1 their constituting elements, and the complexity of the composition; each element has its proper place of fulfilment and acts only in coexistence with all its partners. There are central, stronger, and weaker, peripheral factors, being essential for the balance of the whole, and only this totality is a balanced energy potential. In other words, there is no hierarchy of “main”, “leading”, “active”, “inactive”, “unknown”, or “superfluous” substances, whose constituents can be singled out. Jarnu is a whole “cosmos of medicine”, amicrocosm within a macrocosm, a body within another bigger one, like every spiritual, social, human, animal-like or plant body.
In 1948, the famous scholar Sastroamidjojo, author of the Indonesian essential book on jamu, expressed these basic ideas of Indonesian and Malay thiiking his way: “In other words, Our slrin does not really border Our bodies from the outside world. Our bodies have an interrelation- ship with the cosmos, much like the cells constituting Our body, and the atoms which malce up each of those cells. Unity/oneness, in this case constituted by Our bodies’ cells, forms a part of the cosmos that cannot be separated from the big universe, which is infinite. This unity, microcosm and macrocosm together, is always in a state of balance. In na- ture there really are no sharp and straight borderslboundary lines, Jzaturu non facitsaltzw.” (SASTWOAMIDJOJO 19881 1948; translation by G.T.) In general there are two ways in Western phytopharmaceu- tical research In the first, phytopharmaceuticals have mo- lecularly definable, active ingredients and tl~eir efficacy is seen as their sum total; any function of urknown, less active or “inactive” substances is denied. Or, as a more recent de- velopment, scientists try to concentrate on the total compo- sition, which can be investigated only as a total extract or preparation and places less emphasis on the search for “main” or “leading” active substances; qualitative interrelations are considered more important than materiaUquantitative ones. But this latter field of science still laclts Western scientific methods, for what scientific processes can be used to ex- periment with or investigate total extracts? How would pri- mary and secondary effects be elucidated? What can be said about the characteristics of a pure and absolute substance in comparison to a total extract or an entire plant preparation? How can synergism and risk reduction be psoved? Both of the above ways are discussed with considerable controversy and emotion, and each raises questions beyond pharmacol- ogy and natural science. They are based on different para- digm and world-views which, as cultural constructs, have considerable influence on scientific work.
This very discussion of synergism and risk reduction was started by the Indonesian natural scientist Sutrisno in 1976, but clearly laclcing the “correct” scientific means. He formu- lated a SEES (Side effect eliminating substance/Secondary effectiveness enhancing substance) theory, postulating fewer side effects and a well-balanced total efficacy of entire plant extracts. In the West, the SEES-theory was not accepted (REHM 1985) due to the lack of an experimentd basis and “sufficient“ scientific proof. Western scientists, working on the explanation of isoldted phenomena at a micro-level, look for analysis and experimental proof of single constituents. Sutrisno’s attempt to develop m underlying theory has a clear relation to his world-view: if every level of existence is mod- elled on “the whole” - in the last consequence on the divine power - why shouldn’t a scientist work on a theory using “the whole”? It might add new aspects to the appraisal of this theory, or any scientific theory for that matter, to bear in mind different world-views - and their existence is a cultural con- stant - behind opposing scientific statements.
TWO WBRLDS - JAMU IN SINGAPBRE Singapore is a Southeast-Asian melting pot for different, and sometimes, contradicting traditions and world-views: on the one hand it is strongly oriented towards Western standards of scie.nce, business and faskion; and on the other, Southeast Asian’s social, cultural and philosophicai val- ues do not always parallel this Western orientation. In the janttc products, the two world-views and theis resulting scientific approaches meet.
The different concepts of medication cause problems for a state so oriented to Western standards of science, business and fashion. Singaporean health authorities would like to treat the jamu products in the same manner as Western phar- maceuticals, i.e. to analyse al1 ingredients, standardise them, and describe their components and functions exactly. In 1989 there was a plan to investigate al1 non-Western pharmaceuticals, includingjnmu, after completing the reg- istration of Western drugs in 1991; this would have pro- vided one legal category of medicines with one set of laws and rules (Singaporean Ministry of Health Official; per- sonal communication 1989).
This corresponded to Western scientific t W n g : Much as Western pharmaceuticals move along a scale from the com- plex to the pure substances, scientists try to develop the phytopharmaceuticals of the aforementioned group three and four into those of group two. Much research has been done in Western and Southeast-Asian laboratories to screen and malyse al1 jarnu ingredients in order to be able to standardise them and to test the products for security and effkacy. In tlpis process, empirical knowledge does not count, yet. Standardisation is
Actes du 2e Colloque EuropCen d’Ethnopharmacologie et de la 1 le Conférence internationale d‘Ethnom6decine, Heidelberg, 24-27 mars 1993.

MI~DICAMENTS ET ALIMENTS : L’APPROCHE ETHNOPHARMACOLOGIQUE I 41
the “magic word” for scientists and producers; if they succeed in this endeavour, jamu would be able to compete with other pharmaceuticals and could be exported to the West. But the analysis of all jamu ingredients soon reaches methodological limits, and can only be completed for a few of the substances of some medicinal plants. Until now, it has been impossible to completely analyse a plant’s entire preparation - and the task is made that much more difficult in compositions of dozens of plants as are found in many jamu.
Industrial producers would also like to fulfil the demands of Western science and technology standards, but these standards are not their own and sometimes hard to understand or fulfil. If producers could satisfy the West’s criteria, they could ex- port to Western countries and receive international recogni- tion. On the other hand, they want to continue producing medicines according to non-Western traditions andknow-how.
Singaporean (and Indonesian) producers, sellers and authori- ties know about Western standards in spite of being unable to adapt jamu to them. But the pressure to make accommoda- tions to this ideal is high, coming also from better educated urban customers. In Singapore, this has led to what is some- times a very odd mixture of old fashioned jamu promotion with modern medical accessories. On registered (or tested) products, one finds the registration number (for products from Indonesia) or a supplement to the same effect indicating test- ing by the Ministry of Health. For consumers, this creates the notion that the ingredients have been comprehensively tested for their efficacy, when in fact it means little more than “tested for toxic substances”, which cannot exceed certain limits. In Singapore, the substances are mercury (limit: 0.5 ppm), lead (20 ppm), copper (150 ppm) and arsenic (5 ppm) (Ministry of Health Official; personal communication 1993).
Occasionally products are also screened for mixing with reg- istered, i.e. prescription drugs; sometimes producers are tempted to “improve” the efficacy of their jamu by adultera- tion with painkillers or even hormones. In 1985, a popular imitation jamu for rheumatic disorders with the brand name “Air Pancur” (a derision of the Indonesian jamu factor’s name “Air Mancur”) had to be recalled from market shelves; it was found to contain Diazepam, Indomethacin and Phenylbuta- zone, although this example is nothing extraordinary com- pared to medicine scandals that have occurred elsewhere in the world. According to Singaporean health authorities, there are not many cases of adulteration or contamination. At any rate, unsafe medicines are only brought to the attention of authorities if there are incriminations. “But Malays seldom complain. They are not the people to complain.. .” (Ministry of Health Official; personal communication 1993). The market is big enough to support fakes and imitations, too, terms which are etic ones in this context: Consumers usu- ally are indifferent about brands and labels unless their atten-
tion is drawn to it. The impostor products can be sold in many different ways: many products are sold with no label at all, since they are well known to consumers; alternatively, they are sold under an original or very similar brand name; there are also “Indonesian” jamu packaged and sometimes also pro- duced in Singapore or Malaysia, although only the raw ingre- dients are imported from Indonesia. The existence of the warning Awas barang tiruan! (Beware of fakes!) is helping to create consciousness of brand names.
But Singaporean consumers are often too aware of the outer indicators of “progress”, and attach great importance to them even if the indicators do not tell them anything. Occasionally, imitations or fakes of janzu brands carry imitated registration numbers which, for example, read: “doctor number A71 47721” - enough to satisfy the customer’s expectations of a modem, “tested” jamu product.
It is difficult to monitor situations such as those described above as they relate to “traditional modern” jamu in Singapore, but “developing” jamu into standardised phytopharma- ceuticals would not make the task any easier. First, because of the technical impracticability of this undertaking; even if were possible, it would consume the energy of generations of scientists. Second, and more importantly, jamu cannot be trans- lated into a Western scientific system. Tt would of course be possible to produce standardised phytophmaceuticals with one or two active ingredients, but these would not be jamu. And third: Why should a phytopharmaceutical like jamu be forced to conform to Western standards?
In the face of these problems, Singaporean health authorities did not proceed with the plan to register non-Western pharma- ceuticals in the same way as Western ones. They merely main- tained common regulations for “traditional medicines”, which do not require registration or licensing as long as the packages show a product composition written in English on the label; any adulteration is prohibited. Furthermore, producers are pro- hibited from promoting their products for any of the following nineteen specified diseases and conditions: blindness, cancer, cataracts, drug addiction, deafness, diabetes, epilepsy or fits, hypertension, insanity, kidney diseases, leprosy, menstrual dis- orders, paralysis, tuberculosis, sexual function, infertility, im- potency, frigidity, conception and pregnancy (Mmstry of Health Official; personal communication 1993).
In fact, the majority of the popular jamu are indeed used for the treatment of some of the listed diseases or conditions. Produc- ers and sellers try to skirt the prohibition by using linguistic tricks and sometimes by just crossing out the incriminated terms on the original packaging. In this manner, the jamu products are allowed to continue their century-old career in Singapore. So far, this has been the only way to handle the “modern tradi- tional” jamu, since a general ban would be unjustified and cre- ate significant social and political awkwardness.
Actes du 2e Colloque Européen d‘Ethnopharmacologie et de la Ile Conférence internationale d‘Ethnomédecine, Heidelberg, 24-27 mars 1993.

42 BMÉDICAMENIS ET ALIMENT5 : L’APPROCHE ETHNOPHARMACOLOGIQVE
Actes du 2e Colloque Européen d’Ethnopharmacologie et de la lle Conférence internationale d‘Etlmom&lecine, Heidelberg, 24-27 mars 1993.
The shifting of the discussion between tradition and moder- nity, between Indonesia, Malaysia and Singapore blurs an- other aspect of jumu trade which often escapes the public’s notice: the very “modern” profit. Singaporean jamu selIers take advantage of low prices and production costs in Indone- sia and Malaysia, and use the manifold marketing possibili- ties offered by their metropolitan City state. Some jurnu businessmen are registered only as “general importers and exporters”: they buy the raw ingredients frorn Indonesia, mail them to Singapore, export them to Malaysia where they own factories, and re-import the ready-made product to Singapore. One doesn’t even need an office in Singapore for this job, an adequate representative car is enough. If one considers only the difference in sale prices between Indonesia and Singapore (and of course wholesalers do not buy at retail prices, although they may have other cost factors), the profit is between 200-500% - and there is no tax or customs on the import of Indonesian goods. The businessmau who disclosed confiden- tially: “The profit is really very, very gooc’ was surely not telling lies. And certainly this factor is another strong argu- ment for Singaporean health authorities to laeep jamu alive.
NOTE 1. “Malay” is an ethnic category and refers to the ethnic Malay peo- ple and their language. Malay people live in varying proportions in the states of the whole Malay Archipelago.
REFEPXENCEO: AFDHAL A.F., WELSCH R.L., 1988, The Rise of the Modern Jamu Industry in Indonesia, in S.V.D. GEEST, S . REYNOLDS (Eds.), The Context of Medicines in Developing Countrim, Dordrecht. Air Mancur, Buku Daftar Jamu, Solo n. d. BACH G., 199 1, Zwischen Staatsideologie und Islam: Malaiische Ilfedizin in Singapore, Hamburg. BEDLIPIJGTOW S.S., 1914, The Siqppore MaIay Commurrity: The Poli- tics of State Integration, Corne11 University. ETKIN N., 1988, Cultural Construction of Efficacy, in S.V.D. GEEST, S. REYNOLDS WHYTE? (Éd.), The Conte.ut ofhfedicines in Developing Cozcntries, Dordrecht. GEEST S., v.d. 1988, Phmaceutical Anfhropology, Perspectives for Researcl~ and Application, in S.V.D. GEEST, S . REYNOLDS WHYTE (Éd.), The Conte.Tt of Medicines i n Developing Cozn1tries. Dordrecht. HART D., 1969, Bisayan Filipbzo arzd Ilfalayan Humoral Pathologies: Folk Medicine and Ethnohistory in Southeast Asia, New York. LADERMAN C., 198 1, Symbolic and Empirical Reality: A New Ap- proach ta the Analysis of Food Avoidances, Americm Ethnolo,qist, 9(3),
LADERMAN C., 1981, Destructive Heat and Cooling Prayer: Malay Humoralism in Pregnancy, Child-birth and the Post-Partum Period, Soc.Sci.& Med,. 25(4), 351-365. MANDERSON L., 198 1, Traditional Food Classifications and Humoral Theory in Peninsular Malaysia, Ecol.Food & Nufrition, 11,81-93. MANDERSON L., 1987, Hot-Cold Food and Medical Theories: Over- view and Introduction, Soc. Sci. & Med., 25(4), 329-330. PdARDIWARSITO L., 198 1, Kamus Jawa Kuna (Kawi)-IndonesiaEnde, Flores. “Only spot checks for traditional medicines now”. October 8, 1989, The Sunday Times. REHM K.D., 1985, Jamu - die traditionellen Arzneimittel Indonesiens, in SCHRODER E. @id.), Ethnobotanik - Ethnnbotccny, Curare-Sonder- band, 3,403-410, Braunschweigtwiesbaden. SA’ ADAH binteYusof, 1981/88, Cultural Appraisal of Flora: Malay Folk- Medicine in Singapore, Unpublished Academic Ecercise, Dep. of Geog- raphy, National University of Singapore. SASTROAMIDJOJO S . , 1988/1948, Obat Asli Indonesia Jakarta. §IMAWDJUWTAKE.S., 1984, Meningkatan Pemasaran Jamu, Menjual Gairah Seks, Prisma, 2,74-84. TUSCHINSKY C., 1992, Produktion, Handel und Konsumtion nicht- Mtestlicher Medihnzente in Siidost-Asien: Malaiische jamu iu Singapore. Hamburg. WILKINSON R.J., 1959, A Malay-English Dictionary (Romanised), London. WJ.LICIN§ON R.J., 1985/1903, I<amus Jawi-Melayu-Inggeris, (AClas- sic Jawi-Malay-English Dictionary), Melaka. WOODWARD M., 1985, Healing and Morality: A Javanese Example. Soc.Sci.& Med., 21/9, 1007-1021. ZOETMULDER P.J., 198 1, Old Javanese-English Dictionary 1, S’Gravenhage 1982.
Publication with the same title: TUSCHINSKY C., 1995, Soc. Sci. Med. Vol. 41, No. 11, 1587-1595.
468-493.