3. The Antitussive Action Codeine- Mechanism, Methodologyand
30
Bull. Org. mond. Sat 1969, 40, 425-454 Bull. Wid Hithi Org.f Codeine and its Alternates for Pain and Cough Relief* 3. The Antitussive Action of Codeine- Mechanism, Methodology and Evaluation NATHAN B. EDDY, M.D.,1 HANS FRIEBEL, Dr. med.,2 KLAUS-JORGEN HAHN, Dr. med.8 & HANS HALBACH, Dr. med. Dr.-Ing.4 This report-the third of a series on codeine and its alternates for pain and cough relief-presents a detailed review of the physiology and pathophysiology of cough, the methods for the experimental and clinical measurement of the antitussive action of drugs, possible mechanisms of action of antitussive agents, and includes a compilation of experi- mental results and clinical experience with codeine as an antitussive. CONTENTS INTRODUCTION .... . . . . . . . . 425 MECHANISM AND SIGNIFICANCE OF COUGH . . 426 METHODS FOR THE STUDY OF ANTITUSSIVE ACTION ..... . . . . . . . . . . 428 PHARMACOLOGICAL COMPONENTS OF THE ANTITUSSIVE EFFECT . . . . . . . . . . . 434 ANTITUSSIVE ACTION OF CODEINE . . . . . . 441 RESUMt . . . . . . . . . . . . . . . . 451 REFERENCES . ......... . 452 INTRODUCTION Codeine was first used as a therapeutic antitussive agent soon after its separation as an alkaloidal entity (Martin, 1834) and some of the earliest accounts of dosage and of the circumstances of its use are sum- marized by Krueger, Eddy & Sumwalt (1943). Codeine has indeed dominated the picture with * This review of the analgesic and antitussive effects of codeine and its alternates is being published in the Bulletin of the World Health Organization in five instal- ments. The first, devoted to an assessment of codeine as a pain reliever, was published in Bull. WId Hlth Org., 1968, 38, 673-741. The second instalment, on alternates to codeine as an analgesic, was published in Bull. WId Hlth Org., 1969, 40, 1-53. The third presented here is devoted to the evaluation of codeine as an antitussive agent. The fourth instalment will deal with potential alternates for cough relief. The final instalment will con- sist of a discussion and summary of the preceding reviews. 1 Consultant, National Institutes of Health, Bethesda, Md., USA. 'Professor of Pharmacology and Toxicology, Univer- sity of Heidelberg, Germany. Present address: Chief, Drug Safety, World Health Organization, Geneva. ' Department of Medicine, University of Heidelberg, Germany. 'Director, Division of Pharmacology and Toxicology, World Health Organization, Geneva, Switzerland. respect to the symptomatic management of cough, with only minor variations, and this situation has been influenced little by the introduction of sub- stances claimed to be superior in effectiveness and safety (Domenjoz, 1952; Winter & Flataker, 1954; Pellmont & Biichtold, 1954).5 The number of compounds alleged to possess anti- tussive action comparable with, or superior to, that of codeine has increased greatly in recent years (see Part 4) but the popularity of codeine continues and its annual consumption remains at a high level, paral- leling the high frequency of need for relief of cough as a symptom, especially chronic cough. Bickerman (1960) estimated, not so long ago, that 13% of the population of the United States of America was more than 65 years old and that there were not less than 1 300 000 chronic coughers. Watt (1958) estimated that in the United Kingdom of Great Britain and Northern Ireland 10% of all prescriptions were for cough relief. The need for antitussive preparations 6 Heroin was introduced 50 years earlier as a superior antitussive but obviously proved itself to be less safe and, in spite of persistent claims as to its specificity, it has been banned from therapeutics in most countries. No further reference to it will be made. 2312 -425
Transcript of 3. The Antitussive Action Codeine- Mechanism, Methodologyand
Bull. Org. mond. Sat 1969, 40, 425-454Bull. Wid Hithi Org.f
Codeine and its Alternates for Painand Cough Relief*
3. The Antitussive Action of Codeine- Mechanism, Methodology and Evaluation
NATHAN B. EDDY, M.D.,1 HANS FRIEBEL, Dr. med.,2 KLAUS-JORGEN HAHN, Dr. med.8& HANS HALBACH, Dr. med. Dr.-Ing.4
This report-the third of a series on codeine and its alternates for pain and coughrelief-presents a detailed review of the physiology and pathophysiology of cough, themethods for the experimental and clinical measurement of the antitussive action of drugs,possible mechanisms of action of antitussive agents, and includes a compilation of experi-mental results and clinical experience with codeine as an antitussive.
CONTENTS
INTRODUCTION .... . . . . . . . . 425
MECHANISM AND SIGNIFICANCE OF COUGH . . 426
METHODS FOR THE STUDY OF ANTITUSSIVE
ACTION ..... . . . . . . . . . . 428
PHARMACOLOGICAL COMPONENTS OF THEANTITUSSIVE EFFECT . . . . . . . . . . . 434
ANTITUSSIVE ACTION OF CODEINE . . . . . . 441RESUMt . . . . . . . . . . . . . . . . 451REFERENCES . .......... 452
INTRODUCTION
Codeine was first used as a therapeutic antitussiveagent soon after its separation as an alkaloidal entity(Martin, 1834) and some of the earliest accounts ofdosage and of the circumstances of its use are sum-marized by Krueger, Eddy & Sumwalt (1943).Codeine has indeed dominated the picture with
* This review of the analgesic and antitussive effectsof codeine and its alternates is being published in theBulletin of the World Health Organization in five instal-ments. The first, devoted to an assessment of codeine asa pain reliever, was published in Bull. WId Hlth Org.,1968, 38, 673-741. The second instalment, on alternatesto codeine as an analgesic, was published in Bull. WIdHlth Org., 1969, 40, 1-53. The third presented here isdevoted to the evaluation of codeine as an antitussiveagent. The fourth instalment will deal with potentialalternates for cough relief. The final instalment will con-sist of a discussion and summary of the preceding reviews.
1 Consultant, National Institutes of Health, Bethesda,Md., USA.
'Professor of Pharmacology and Toxicology, Univer-sity of Heidelberg, Germany. Present address: Chief, DrugSafety, World Health Organization, Geneva.
' Department of Medicine, University of Heidelberg,Germany.
'Director, Division of Pharmacology and Toxicology,World Health Organization, Geneva, Switzerland.
respect to the symptomatic management of cough,with only minor variations, and this situation hasbeen influenced little by the introduction of sub-stances claimed to be superior in effectiveness andsafety (Domenjoz, 1952; Winter & Flataker, 1954;Pellmont & Biichtold, 1954).5The number of compounds alleged to possess anti-
tussive action comparable with, or superior to, thatof codeine has increased greatly in recent years (seePart 4) but the popularity of codeine continues andits annual consumption remains at a high level, paral-leling the high frequency of need for relief of coughas a symptom, especially chronic cough. Bickerman(1960) estimated, not so long ago, that 13% of thepopulation of the United States ofAmerica was morethan 65 years old and that there were not less than1 300 000 chronic coughers. Watt (1958) estimatedthat in the United Kingdom of Great Britain andNorthern Ireland 10% of all prescriptions were forcough relief. The need for antitussive preparations
6 Heroin was introduced 50 years earlier as a superiorantitussive but obviously proved itself to be less safe and,in spite of persistent claims as to its specificity, it has beenbanned from therapeutics in most countries. No furtherreference to it will be made.
2312 -425
N. B. EDDY AND OTHERS
is clear and codeine is our standard of reference.However, two facts have given impetus to the searchfor an adequate substitute-substances without anal-gesic action can exhibit antitussive potency and suchsubstances may be entirely devoid of morphine-likedependence-producing properties (Isbell & Fraser,1953).
In recent years much attention has been directedto the mechanism of cough and its relief and toadequate methodology for the measurement of thelatter. This work will be discussed first and will befollowed by details of the antitussive action ofcodeine and later (in Part 4) by a discussion of thepotential alternates.
MECHANISM AND SIGNIFICANCE OF COUGH
Reviews of this topic have been prepared by Bucher(1958), Bickerman (1960), Friebel (1963) andWiddicombe (1964). Cough is a protective reflex,the purpose of which is to remove irritating materialsor sensations from the respiratory tract, and as suchits pathways include sensitive receptors, afferent nervefibres, central connexions with a " relay station inthe arc for cough reflex" (May & Widdicombe,1954), and efferent nerves. Experiments of Larsell& Burget (1924) and Widdicombe (1954) demonstra-ted two types of receptors: one in the trachea, sensi-tive to mechanical stimuli, the other throughout thetracheobronchial tree, responding chiefly to irritatingchemical stimuli. The afferent nerve fibres, whichconduct the action potentials arising in these recep-tors, pass along the superior laryngeal nerve and thevagus, entering the medulla with the vagus root.Section of the vagus below the point at which it isjoined by the superior laryngeal nerve does not sub-stantially affect the cough threshold of anaesthetizedcats (Sell, Lindner & Jahn, 1958), indicating probablythat the stretch receptors in the lung (Bucher & Jacot,1951) take little part in the cough reflex. Cough-exciting impulses from the pharynx are carried inthe glossopharyngeal nerve.The existence of a specific cough centre located
in the dorsolateral region of the medulla close tothe respiratory centre was suggested by Borison(1948) and by Chakravarty et al. (1956). This sug-gestion was confirmed by Engelhorn & Weller (1961,1965), who localized a central mechanism for theadaptation of the activity of the respiratory system toacute changes in its environment in the lower ponsand medulla. Its nervous components, E, neurones,were localized in the caudal end of the nucleus am-
biguus. The authors assumed connexions betweenthese neurones and the receptors characterized byWiddicombe (1954). Under normal breathing condi-tions these neurones are silent but become activatedby noxious stimulation and may play an importantrole in the central processing of cough-evoking stim-uli (Engelhorn & Weller, 1965).The existence of other connexions of the cough
centre must be assumed and has been partially de-monstrated. Section in the forward part of the pons,for example, weakens the cough response in the cat.Spread of excitation of the cough centre to the vomit-ing centre is well known, connexions with the respi-ratory centre must exist, and considerable voluntarycontrol, even suppression of cough is possible (Kuhn& Friebel, 1960a, 1960b; Engelhorn & Weller, 1961;Friebel & Hahn, 1966; Hahn & Friebel, 1966).
Efferent impulses from the cough centre, co-ordi-nating movements of the glottis, the diaphragm andthe abdominal and intercostal muscles in the act ofcoughing, pass over the recurrent, the phrenic, theintercostal and other nerves.Cough is understood as an explosive expulsion of
air resulting in the " generation of a high-linear-velo-city air stream with high kinetic energy available forthe acceleration and displacement of an object in theairway" (Ross, Gramiak & Rahn, 1955). Theseauthors assume the explosive expulsion of air to bethe product of substantial elevation of intrapleuralpressure and sudden opening of the glottis. Equali-zation of pressure in the trachea with the outside aircreates a pressure differential along the bronchialtree and the bronchi narrow passively. This allocatesa key position in the expulsion of air to the move-ments of the glottis. These movements, at least theinitial closure of the glottis, are centrally controlledindependently of intrathoracic pressure and are car-ried out even if no air-flow occurs. The other factorto bring about the air expulsion is the force of themuscular contractions. Even if the movements ofthe glottis are inhibited, or the expired air goes outthrough a tracheal fistula, remarkable blasts of aircan be produced (Floersheim, 1959).The act of coughing is often, but not necessarily,
initiated by an inspiration (Staehelin, 1914; Trende-lenburg, 1950; Widdicombe, 1954, 1961; Kuhn &Friebel, 1960a,- 1960b; Friebel & Hahn, 1966; Hahn& Friebel, 1966). This is not consistent with a veryclose correlation between the central portion of thecough reflex arc and the respiratory centre. Engel-horn & Weller (1965) suggested that the EQ neuronesbelonged to an independent sensitive mechanism for
426
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
the protection of the lung against noxious stimula-tion. Friebel & Kuhn (1962) in this connexion show-ed that the cough and respiratory centres reacted dif-ferently to drugs. They demonstrated that 2-amino-indane stimulated respiration in conscious andnarcotized guinea-pigs but depressed the cough reflexmechanism. In fact the cough reflex mechanism con-tains peculiarities in its function and organizationwhich seem to exclude a close association with the res-piratory mechanism. Its functions can be looked uponas summing the cough-inducing stimuli, co-ordina-ting the respiratory musculature to initiate the coughreaction and interrupting the respiratory rhythm infavour of the cough reaction (Kuhn & Friebel,1960b).Summation of afferent impulses towards the pro-
duction of cough was suggested by Stefko & Bensofn(1953) and Bucher (1958). Experiments of Friebel &Hahn (1966) in conscious guinea-pigs gave evidenceof a remarkable ability of the cough centre to storethe afferent impulses. The animals reacted with anexplosive expulsion of air, on the average 2.8 secondsafter an appropriate electrical stimulation of thetracheal mucosa was initiated. A response couldstill occur with weaker stimulation up to a latency of16 seconds. If the stimulation was too weak to evokea cough reaction in 16 seconds, it did not producecough at all. The authors concluded that the sum-mation of cough-inducing impulses served two pur-poses. It intensified the protective function of thecough reflex and prevented unlimited activity of thecough reflex mechanism. Variability in the latencywas the only specific modification of the intensity andcharacteristics of the single cough response producedby variation in the intensity, duration and frequencyof stimulation. Obviously, the central part of thecough reflex arc was able to collect variable afferentimpulses and transform these into efferent reactionsof relative uniformity (Friebel & Hahn, 1966).The efferent impulses of the cough reflex activated
the respiratory muscles which normally carry out themovements of breathing, so that the normal respira-tory rhythm was interrupted or postponed (Kuhn &Friebel, 1960b). The moment of interruption varied.In 85 of 100 cough reactions recorded from electri-cally stimulated conscious guinea-pigs, the explosiveblast began at the height of inspiration, in 12 it beganduring expiration and in three at the moment ofcomplete expiration. An interruption of inspirationshas never been observed (Hahn & Friebel, 1966).Rarely, an acceleration of the normal expiration,leading to a typical cough reaction, has been
recorded. Engelhorn & Weller (1965) observed inanaesthetized cats an inhibition of the activity ofexpiratory neurones (Ea) on account of the activityof cough-specific E, neurones.The newer information on the organization and
function of the cough reflex mechanism, therefore,supports the hypothesis of its independence, in themain, of the respiratory mechanism, in respect tocough-provoking stimulation, summation of afferenttussive impulses and transformation of these im-pulses for co-ordination of the respiratory muscu-lature to produce the explosive cough response.The functions of the cough reflex as a protective
device are:
(1) warning against noxious irritation and damagein the airways from inhaled chemicals or foreignbodies; and
(2) clearing the airways by removal of the offend-ing irritant.
Cough is a symptom in a wide variety of diseases.Inflammation of the respiratory tract can be accom-panied by increased irritability of the sensory recep-tors and intrapulmonary tumours can evoke coughby pressure on or involvement of sensitive receptorsand nerve fibres. The cough response via the auricu-lar branch of the vagus on account of inflammation,etc., of the external auditory meatus is well known.Cough may be an allergic response, a consequenceof circulatory disturbances or it may be psychogenic.Cough arises most commonly from a stimulus withinthe respiratory tract, from infections or mechanicalirritation within the lumen (Bickerman, 1960b) orfrom inhalation of polluted air or tobacco smoke(Phillips, Phillips & Thompson, 1956; Herzog, 1967).From the clinical standpoint, cough is probably themost important mechanism of bronchial catharsis(Bickerman, 1960b). If cough is present for a consid-erable time, adaptation may occur and the patientmay become almost unaware of its occurrence; or,the apprehensive person may exaggerate its intensity.When the cough is incapable of, or ineffective in,
removing the provoking stimulus, tussive insuffi-ciency results. In many suppurative diseases of thelung, cough is unable to remove the thick, tenacious,mucopurulent secretions which form constantly inresponse to the infection. The dry, hacking, irritativecough of some acute infections of the respiratorytract, such as laryngitis, tracheobronchitis and per-tussis, may by itself become a major factor in retard-ing recovery by causing loss of sleep, inadequate foodintake, nausea and emesis. In obstructive disease of
427
N. B. EDDY AND OTHERS
the tracheobronchial tree, such as tumours, foreignbodies and chronic asthma, the cough reflex maybecome self-perpetuating and the resultant severeparoxysms of unproductive coughing may causeserious debilitation of the chronically ill patient(Bickerman, 1960b; Banyai & Johannides, 1956).Other consequences of severe protracted coughing arepulmonary emphysema, fractures of ribs, cough syn-cope, urinary incontinence, post-operative disruptionof abdominal incisions and spontaneous pneumo-thorax. The necessity of cough-depressing therapyfor unproductive cough is acknowledged (Friebel,1963).
METHODS FOR THE STUDY OF ANTITUSSIVE ACTION
Measurement of antitussive potency in animal experi-ments
There are many reports of attempts to assess anti-tussive potency in animals; 70 reports in respect ofcodeine, arranged according to animal and method,have been summarized in Table 27, yielding a widerange of effective doses, from 0.3 to 100 mg per kg.The variation is related mainly to the method, butthis has varied in detail, even when it was said to bethe same, in respect of the stimulus used to evokecough, and analysis of the data has varied with theinvestigator. Generally, however, one can assumethat the method and analysis were the same whencomparison was made in a particular case betweena new agent (or agents) and codeine. It is worthwhile, we believe, to discuss the methods, at leastin principle, the conditions of their application, andtheir significance, reliability and interpretation asmeans of measurement.
Intrapleural injection. Systematic exploration ofcough-depressing activity began with Ernst (1938),who reported cough thresholds in cats with artificialchronic pleuritis. The inflammation was producedby intrapleural injection of iodine (Lugol's solution),after which percussion of the chest wall produced acough reaction. Though Ernst (1939) claimed theresults were reproducible, the method has been usedonly infrequently with no effort towards its refine-ment.
Irritating chemicals. Eichler & Smiatek (1940)were the first to use irritating chemicals to stimulatecoughing. Their basic procedure has been variouslymodified. Usually the animals have been exposed tothe mixture of irritating gas, vapour or aerosol withair, in a chamber suitable for one animal and for
visual or acoustical observation or instrumentalrecording of cough reactions. Winter & Flataker(1954) used ammonia vapour and sulfuric acid aero-sol; Friebel, Reichle & von Graevenitz (1955) intro-duced the inhalation of sulfur dioxide mixtures;G6sswald (1958) used citric acid; Silvestrini & Maffii(1959) employed acrolein vapour; and Kroepfli (1950)blew soap powder against the tracheal mucosa. Eachof these agents elicits cough by stimulation of chemo-receptors and each has its advantages and limitations.
Receptors sensitive to cough-provoking irritantsare spread throughout the trachea and bronchi(Larsell & Burget, 1924; Widdicombe, 1954). Thusthe inhalation of gases, vapours and aerosols caninfluence many of them, whereas the introduction ofsolid material such as soap powder will reach onlya few in the trachea. But vapours, etc., inhaled viathe nose and pharynx will also stimulate receptorstherein, perhaps eliciting sneezing as well as coughingand making discrimination difficult if the response isrecorded instrumentally, as it was by Winter & Fla-taker (1954). Rosiere, Winder & Wax (1956) andLaBarre & Plisnier (1959) therefore directed theair-flow through an opening in the trachea and hadto use anaesthetized animals or others with a chronictracheal fistula.
Irritants like citric acid, acetic acid, ether, acrolein,ammonia, sulfuric acid or sulfur dioxide have differ-ent cough-eliciting potency and the concentration forcough threshold varies widely from less than 1.0%(sulfur dioxide) to 20.0% (citric acid) (Friebel,Reichle & von Graevenitz, 1955; G6sswald, 1958).The duration of their action is also different anddepression of cough evoked by inhalation of sulfurdioxide requires a larger dose of codeine than coughinduced by ammonia if the guinea-pig is the test ani-mal (Friebel, Reichle & von Graevenitz, 1954; Winter& Flataker, 1954). On the other hand, dogs showless difference according to the chemical irritant used.It would be worth while to know to what extent theeffective dose of codeine for a particular speciesdepends upon the physiological characteristics of thespecies or upon the stimulus and the details of themethod.Not only does the irritant potency of the chemical
stimulant vary but also its effectiveness varies accord-ing to the concentration and absolute amount at thesite of stimulation. Amdur (1957), for example,showed that the effect of sulfuric acid aerosols onbronchial receptors more nearly approached that ofsulfur dioxide gas the smaller the droplets of theaerosol. Also the smaller the droplets the more tran-
428
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
sient the effect and the faster the recovery. This isimportant for the stability of the cough threshold,since the usual procedure is to determine the thresh-old before and at intervals after drug administration.A change in normal sensitivity of the receptor withtime would influence the accuracy of the judgementof the drug's effect. Therefore, limited stimulationwith adequate intervals for recovery have to be takeninto account, as they have been by some authors.Friebel, Reichle & von Graevenitz (1955) recordedin 3.8% of guinea-pigs a decrease in sensitivitybetween two applications of sulfur dioxide 30 minutesapart. If soap powder is blown into the trachea aconsiderable adaptation of the receptors has to betaken into account (Kroepfli, 1950) because the solidirritant is scarcely removed from the site of applica-tion.One advantage of a chemical irritant as the cough
stimulus is that it permits the use of many animalsin a single experiment, facilitating statistical analysisof the results. This no doubt explains the frequencywith which such stimuli have been employed.
Mechanical stimulation. Kase (1952) was the firstto describe a method for the production of cough bymechanical stimulation of the tracheal mucosa suit-able for the measurement of antitussive action. Themost sensitive area for such stitnulation is at thebifurcation of the trachea. It may be reached throughthe fenestrated wall of the trachea by various devices,bristles, catheters, etc., but these must be appliedcautiously to avoid damaging the mucosa andcausing a change in sensitivity and adaptation to thestimulation (Larsell &I Burget, 1924; Widdicombe,1954). The strength of the stimulus cannot be con-trolled as accurately as with chemical or electricalstimulation and the animal must be prepared opera-tively. If mechanical stimulation is attempted imme-diately after operation, sensitivity may be impairedby the anaesthetic and later pulmonary infection mayensue. The chief advantage of mechanical stimula-tion is its simplicity and some of its drawbacks areavoided by the technique of Tedeschi et al. (1959).These authors implanted an iron slug within the tra-chea of a dog which could be made to vibrate againstthe tracheal mucosa by bringing a strong electromag-net against the outside of the throat, thus eliciting acough response. After some time, chronic inflamma-tion with epithelial desquamation and loss of sensitiv-ity resulted.
Electrical stimulation. This method was introducedby Schroeder (1951). Electrodes were attached to a
vagal loop and through these, stimuli were appliedin the unanaesthetized animal (dog). The method ofelectrical stimulation which is most often employedwas devised by Domenjoz (1952). The superiorlaryngeal nerve was isolated in the anaesthetized catand stimulated briefly; the number and duration ofstimuli required adjustment in the particular animalto elicit cough reliably. The technique of electricalstimulation with modifications has been employedin anaesthetized guinea-pigs (Krause, 1958), inunanaesthetized guinea-pigs (Kuhn & Friebel, 1960a,1960b) and in unanaesthetized dogs (Stefko &Benson; 1953). The latter authors implanted elec-trodes in the tracheal wall, eliciting cough by stimula-tion of adjacent nerve fibres and receptors, andChakravarty et al. (1956) provoked cough by meansof electrodes placed stereotactically in the medullaof the decerebrate cat.
Various forms of electrical current have been used,with changes in the shape of the single impulse (spike,square or undulatory), and with variations in voltage,current, frequency and duration. There have beenexplorations, too, of interrelationships between volt-age and frequency of stimulation for producing coughmost effectively (Schroeder, 1951; Stefko & Benson,1953) and most recently of the interrelationshipbetween intensity, duration and frequency of thresh-old stimuli by Friebel & Hahn (1966). Variation inthese parameters within described limits had noappreciable effect on the intensity or characteristicsof the cough response, but the latent period betweenthe beginning of stimulation and the occurrence ofthe cough could be decreased (Friebel & Hahn, 1966).
Electrical stimulation to produce cough has nophysiological equivalent; it also requires operativepreparation of the animal and testing immediatelyafter the operation can be influenced by the anaes-thetic. Nevertheless the method has been used bymany and has the advantage of exact measurementof stimulus strength and quality.Avoidance of anaesthesia in antitussive testing was
one of the conditions stressed by Schroeder (1951).A cough-depressing action of some of the anaestheticagents used in animals has been observed or referredto by Schroeder (1951), Domenjoz (1952), Tedeschiet al. (1959), Friebel & Kuhn (1962), Hahn & Friebel(1966) and others. One might expect the effectivedose of the antitussive, codeine for example, to besmaller in experiments performed under anaesthesia,but the data of Table 27 do not give such an indica-tion.Some of the methods for antitussive experiments
429
N. B. EDDY AND OTHERS
require the preparation of a tracheal fistula andthis causes the air passages to be exposed to drylaboratory air instead of air highly humidified bypassage through the nose and throat of the animal.Under this unnatural physiological condition there isevaporation and thickening of the bronchial secre-tion, impaired activity of the ciliated epithelium andpoorer transport of secretions (Perry & Boyd, 1941;Dalhamn, 1960). Even if the inspired air is humidifiedto 30%, ciliary movement stops within 3-5 minutesof opening the trachea. The impairment of mucustransport favours the formation of an immovablelayer of secretion and a change in sensitivity to cough-provoking stimuli (Gordonoff, 1938). If the trachealfistula is maintained chronically, as proposed by Kase(1952, 1954, 1955) there is liability to respiratoryinfections (Rosiere, Winder & Wax, 1956), againinfluencing the threshold for cough stimulation.Similar considerations must be borne in mind in con-nexion with other operative procedures, implantationof electrodes, exposure of the laryngeal nerve, etc.The catalogue of factors which may influence coughthreshold before and after drug administration islong, varying with the working procedure, and theyplay a significant role in the variations in resultsshown in Table 27.
There are also qualitative differences in the animalspecies used in the experiments. Guinea-pigs, catsand dogs are to be preferred. Mice are too small fordiscrimination between sneezing and coughing. Ratsrespond readily to sulfur dioxide inhalation by bothsneezing and coughing and, when tested repeatedlyover a three-month period, showed decreasing sensi-tivity. Guinea-pigs, on the other hand, maintained aconstant sensitivity throughout 48 weeks (Friebel &Kuhn, 1964). In general, the smaller species requirehigher doses per kg of codeine than do the largerspecies to produce the same effect; cough elicitedin guinea-pigs by ammonia is an exception to thisrule. On account of their size, cats and dogs areamenable to all methods for antitussive testing andto all routes of drug administration, but unanaesthe-tized cats and dogs quickly learn to control partiallytheir breathing, restricting the inhalation of irritatingchemicals, so that they have to be checked carefullyto determine whether under undrugged conditions thecough response remains the same. A further draw-back to the use of dogs is their ability to be trainedto the experimental procedure, and to develop avoluntary cough response; the better the relationbetween handler and animal the more ready the res-ponse (Schlez, 1965).
In most experiments with rats and guinea-pigs,drugs have been given subcutaneously; in cats intra-venous injection has been usual, whilst in dogs, allroutes have been used. Intravenous injection has theadvantage of requiring small doses and usually hasa transitory effect, permitting comparison of repeateddoses; if several injections are given the possibilityof summation of subliminal stimuli or of tachyphy-laxis cannot be disregarded. The mode ofadministra-tion takes on added importance when the resultsare considered in relation to man. In antitussivetherapy in man, the oral route is usual, whilst inexperiments in animals it is the exception. Therefore,if antitussive effect is shown in the latter, one alsoneeds to know something of absorption and meta-bolism after oral administration, factors whichhave been largely disregarded in predicting clinicaleffectiveness.
Measurement of antitussive potency in experimentallyinduced cough in man
Cough may be induced experimentally in man byinhalation of an aerosol containing acetylcholine,ammonia or citric acid, or by intravenous injectionof lobeline or paraldehyde.Hdglund & Michaelsson (1950) published the first
report on experimental cough provoked in healthyvolunteers by inhalation of an irritating chemicalcompound. The subjects respired through tubes fit-ted with valves to prevent expiration into the system.Ammonia vapour (2%) in the desired quantity wasadded to the inspired air by means of a syringe. Themomentary closure of the glottis in response wasrecorded by a pneumograph around the subject'schest. The method of Hoglund & Michaelsson, moreor less modified, has been used by Trendelenburg(1950), Blix (personal communication, 1952), Hahn& Willbrand (1952) and Gravenstein, Devloo &Beecher (1954), with all except the latter showingelevation of the cough threshold by codeine. Tren-delenburg and some others relied on subjective obser-vation of apparent closure of the glottis, believingthat this was always in accord with mechanicalrecording. Closure of the glottis was taken as thethreshold response whether or not an explosive actof coughing followed and, according to Trendelen-burg, the amount of ammonia causing this responsewas the indication of threshold. When this had beendetermined test substances were administered andmeasurements of threshold continued every fiveminuttes until the threshold quantity of ammoniahad returned to the original amount required.
430
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
Gravenstein, Devloo & Beecher (1954) could notbe certain why they failed to confirm the results ofthe others. They called attention to two points,firstly that Hoglund & Michaelsson and the othershad not used a placebo as control or used double-blind conditions, and secondly they found that theammonia-mixture container lost ammonia readily.A lower concentration ofammonia would be less irri-tating and if it were used in later trials after an anti-tussive agent it would make the latter appear effective.This would not allow the threshold to return to itsoriginal value.There are also other points at issue in the method.
While closure of the glottis (sudden pause in breath-ing) was chosen as the indication of response, itremains to be proven that this can be accepted as anadequate indication for a cough reaction and whe-ther that reflex is influenced by the same drugs andby the same doses as the cough reflex. Trendelenburg(1950), as well as Hahn & Wilbrand (1952), ob-served wide variations in threshold values dependingupon weather conditions and psychological factors.Trendelenburg, however, did not think initial thres-hold values influenced drug effects. Gravenstein,Devloo & Beecher (1954) found the threshold moreconstant and reproducible, but observed no signifi-cant change after medication.A method closely related in principle to that of
ammonia inhalation was introduced by Bickerman& Barach (1954) and by Bickerman et al. (1956).Cough was induced by'a 25% solution of citric aciddeeply inhaled from a nebulizer through a tight-fittingface mask and a constant oxygen flow of five litresper minute. They recorded the number of coughselicited and the expiratory air flow. The subjecttook three inhalations, resting two or three minutesbetween each. In drug potency tests the response wasrecorded at zero time and hourly to four hours aftermedication. Bickerman et al. (1957) later spoke of" trained " subjects, who worked with the methodthrough many months and showed a reasonabledegree of adaptation (" learning " factor) to the pro-cedure. This group worked under double-blind con-ditions and was challenged with concentrations ofcitric acid from 1.25-25.0% to determine a thresholdstimulus, arbitrarily set as that concentration of citricacid which evoked a total of not less than four coughswhen inhaled five times. Since this threshold levelvaried from subject to subject and sometimes in thesame subject from day to day, it was redeterminedfor each subject at the beginning of each test run.Under these conditions Bickerman et al. (1957)
observed a decrease in frequency of the citric-acid-induced cough of 22.4% at the second and fourthhours after 5 mg of codeine phosphate orally, adecrease of 22.4-32.5% at the first second and thirdhours after 15 mg, and of 22.4-43.1 % at each hourlyobservation after 30 mg of codeine. Changes inexpiratory airflow differed occasionally from differ-ences in cough frequency, and the latter yielded thebetter dose-response curves.The method of Bickerman and his associates has
been employed by Rasch (1957), Archibald, Slipp &Shane (1959), Morris & Shane (1960), Groszman,Birker & Casimir (1961), Calesnick, Christensen &Munch (1961), Tannenbaum (1965) and Silson (1965),who demonstrated a reduction in coughing after drugadministration, and by Gravenstein, Devloo &Beecher (1954) and Sevelius, Lester & Colmore(1965) who did not. Gravenstein, Devloo & Beechersaid that the Bickerman technique did not distin-guish between a noisy, explosive cough and one oflittle intensity, that the quantity of aerosol reachingthe lungs could not be accurately controlled or deter-mined, and that double-blind conditions were diffi-cult to maintain because of recognition by the sub-jects of other effects (sedative action, etc.). Sevelius,Lester & Colmore nebulized different strengths ofcitric acid solution, 5.0-25 %, to determine the con-centration which consistently produced maximumcough response, a different threshold from that usedby Bickerman. In spite of emphasis on selection andtraining of normal volunteers, in all of their sixsubjects the cough response to the same dose ofirritant changed from hour to hour by as much as50%. The subjects also definitely became adaptedto the citric acid irritation and coughed progressivelyless frequently on repeated exposures. Withoutproper placebo control data a " false positive " drugeffect could be ascribed to what was only adaptation.These authors were unable to distinguish between15 and 30 mg of codeine and placebo. This statementconcerning adaptation to the stimulus is at variancewith Bickerman's experience, but Sevelius, Lester &Colmore required stronger citric acid concentrationsand it is not clear whether or not residues of citricacid on the tongue and in the throat were removedby rinsing as they were by Bickerman. Seveliusand his associates maintained that Bickerman'sprocedure was considerably more complicatedthan theirs since he examined 153 " normal "subjects to obtain 21 presenting relatively constantreactivity to the cough-provoking aerosol. Suchselection not only reduces variation in the sen-
431
N. B. EDDY AND OTHERS
sitivity of the cough reflex mechanism related tosmoking, chronic respiratory infections, etc., but willalso reduce the influence of another factor, voluntaryor subjective control over the response, which mayplay a role in all experimentation on humans. Thecough response can be voluntarily suppressed andinitiated.
Results obtained with the Bickerman method havenot always correlated well with clinical effectivenessof the agents tested, in the treatment of pathologicalcough. Bickerman & Itkin (1960) failed to demon-strate a cough-depressing effect with normethadone,though such an effect has been well established inanimal experiments and clinical experience. On theother hand, Woolf& Rosenberg (1964), using a tape-recorder system as an objective measure of coughing,found laevopropoxyphene inactive clinically, whileBickerman et al. (1957) and Calesnick, Christensen& Munch (1961) found it effective against artificiallyproduced coughing.
Recently Calesnick & Christensen (1967) have usedthe citric-acid-aerosol method with a different end-point, the latent period from beginning of inhalationunder pressure through a tight face mask to coughresponse and regarded a lengthening of this periodas indicative of cough suppression. They used onlymales because females were too sensitive to reflexclosure of the glottis which would prevent inhalationof a sufficient amount of the aerosol (25 % citric acid).They also excluded persons who did not give a goodcough response before drugging or who failed toshow an antitussive effect with an exploratory doseof 40 mg of codeine orally. Graded doses were givenwith citric acid challenge hourly throughout fourhours. A good dose-response curve was obtainedwith 5.0-40.0 mg of codeine.
Prime (1961), looking for a controllable agent forartificial cough production, developed an observationof Tiffeneau (1955). The inhalation of a nebulizedsolution of acetylcholine regularly induced more orless coughing in certain persons. Prime also triedether and sulfur dioxide; both were effective, but thetaste and smell were objectionable and the latter asused was so powerful that none wanted to repeat theexperience. In non-smokers, and persons withoutrespiratory infection under 30 years of age, Primefound acetylcholine even at 1.0% completely ineffec-tive, confirming the observations of Tiffenau (1955)and Halsreiter (1959). However, in patients withchronic bronchitis, emphysema, asthma, fibroustuberculosis, pulmonary sclerosis, or acute respira-tory inflammation acetylcholine was 80-90% effec-
tive. Haslreiter's experience was similar, a posi-tive cough response to acetylcholine in mostpatients with chronic bronchitis, etc., and a nega-tive response in all healthy persons. Both Prime(1961) and Sevelius, Lester & Colmore (1965) foundthat cigarette smokers, admitting to only a littlehabitual coughing, responded positively to acetyl-choline.
Haslreiter (1959) and Prime (1961) used acetylcho-line to attempt evaluation of cough depressants. Thesubject breathed his individual concentration (Hasl-reiter, 1959) or 1.0% (Prime, 1961) acetylcholineaerosol until coughing began or at most for 11/2 min-utes and the number of coughs ensuing during thenext 20 minutes was counted. The subject then tookan inert tablet or one containing the cough depres-sant and 20 minutes later the test was repeated. Theactive and inactive tablets were administered in ran-dom order to each subject. Prime compared thecough rates before and after medication with positiveresults; Haslreiter determined the number of patientswho did not coug4 after the test drug. Their resultsdid not correspond. Sevelius, Lester & Colmore(1965) could not confirm Prime's results either. Innine subjects they were unable to distinguish between30 mg of codeine phosphate and placebo, adminis-tered double-blind in random order with 60 or120 minutes allowed for absorption. Prime admittedto them that his later experience was in accord withtheirs. It should also be mentioned that acetylcholineantagonists (hexamethonium, for example), not other-wise antitussive, abolish the cough response to acetyl-choline (Tiffeneau, 1955).As indicated earlier, cough can be provoked in man
by intravenous injection of paraldehyde or lobeline.Gravenstein, Devloo & Beecher (1954) found thatthe usual dose required to produce a satisfactorycough response varied from 0.25 to 0.5 ml in differentsubjects (Konar (1959) used 1.0 ml). The paraldehydewas injected into a vein of the forearm through acontinuous 5.0% dextrose solution drip. The resultwas a feeling of constriction of the chest and anexplosive cough which relieved the feeling. Thecoughing bout lasted 30-60 seconds and might befollowed by an afterburst of coughing. When theeffective dose had been determined and repeated at30 minutes, the antitussive was administered andthe paraldehyde repeated at half-hour intervals for2 or 21/2 hours. Gravenstein, Devloo & Beecherinvestigated the effect of drugs on the response toparaldehyde, and showed a difference between heroin,2.5 mg subcutaneously, and placebo, where the sub-
432
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
jects were used as their own control, but not withcodeine, 10 mg orally or 30 mg intravenously, ormorphine, 5 mg subcutaneously, when the subjectswere not their own controls. Konar (1959) also failedto obtain a positive effect on the response to paral-dehyde with codeine or morphine. Gravenstein andhis associates deemed it unwise to continue with theparaldehyde test because of pain at the site of injec-tion and phlebitis, fear on the part of the subject ofthe feeling of chest constriction, and variability inthe response.
Lobeline administered intravenously excitescough, presumably because of a direct effect on thecough centre (Chabrier, Giudicelli & Thuillier, 1950).The effective dose was 3.0-10.0 mg, and this dosecaused a cough reaction of 10-20 seconds durationfollowed by about 60 seconds of polypnoea. Theauthors found that 80-100 mg of pholcodinedecreased the response to lobeline. They said,however, that lobeline had to be used cautiouslybecause of possible toxic reactions. Hillis & Kelly(1951) were unsuccessful in attempts to suppress thecough response to 5.0 mg of a-lobeline, intravenouslyin normal subjcts, with codeine, morphine or heroin.The cough response was blocked by hexamethoniumiodine.Bickerman & Barach (1954) said that artificial
cough production should meet the following condi-tions: uniform and consistent response of the sub-ject to the same threshold stimulus; the eliciting agentshould be non-toxic and relatively simple in its appli-cation so that observations may be made on manysubjects; and the results should be reproducible.None of the methods described meets these condi-tions completely. The reviewers believe the citric-acid-aerosol technique to be the most promising,best developed, and least disturbing to the subject,but further efforts to develop methods for antitussiveevaluation should be encouraged. Artificially pro-duced cough, in volunteer subjects, is not the sameas cough of pathological origin at least in strength,timing and persistence of cough induction, and onecannot always expect to obtain the same drug res-ponse in both situations. Nevertheless, the experi-ments with artificial cough are worth while for deter-mination of carry-over of effectiveness in this andother respects from laboratory animals to man, butshould be accompanied by studies of absorption,distribution and disposition for further informationon species parallelism. Then one has the backgroundfor interpretation of laboratory results and for clin-ical application.
Evaluation ofantitussive action against cough ofpatho-logical origin
The crucial test for an antitussive is the study ofits effect in patients with spontaneously occurringcough of various origin. Most of the reports in thisconnexion are based on clinical experience ratherthan controlled clinical trial. Reliable, unbiasedevaluation and comparison should come from thelatter, but the former is supplementary and essential.Covering a larger number of patients of more hetero-geneous character, the general clinical observationcontributes to the knowledge of side-effects, unusualadverse reactions and useful indications of applica-tion and contraindication.
Here, as elsewhere, the clinical trial must fulfil somebasic requirements of clinical pharmacology, double-blind procedure to avoid error by suggestion, inclu-sion of placebo or standard drug of established effi-cacy for comparison, and randomization of drugadministration to facilitate statistical analysis. Thisis not the place to discuss the design of specific clini-cal trials but certain features of the procedure, asapplied to the evaluation of antitussives, must beconsidered for better judgement of the significanceof the data to be presented in respect to specificagents. In the main, two approaches to evaluationof efficacy, etc., have been developed-analysis of thesubjective judgement of effect by patient and/orobserver, and objective measurement of changes innumber, severity, etc., of bouts of coughing duringspecific periods of time with and without drug orplacebo-and variations in each approach haveappeared almost from investigation to investi-gation.As much as 31 years ago, Davenport (1938) admin-
istered codeine and closely related substances double-blind to coughing tuberculous patients and concludedthat the optimal oral dose of codeine was only 10 mg,and Himmelsbach et al. (1940) using placebo forcomparison, demonstrated worsening of the coughwhen the change was to the placebo from morphineor codeine. It has been in the past 15 years, however,since the discovery of the antitussive property ofdextromethorphan, that particular attention has beendirected to quantification in evaluative efforts.
Assessment of efficacy is of necessity a comparisonbetween groups, as comparable as possible in sizeand composition, receiving different agents or in theindividual receiving two or more agents. He may beasked to compare his condition at administrationwith that at fixed time intervals thereafter, or his
433
N. B. EDDY AND OTHERS
condition during one period of medication, a day ora week or longer, with that during another equalperiod. He may be asked simply to judge improve-ment, no change or worsening, to express his prefer-ence for the agent used at one time over another, orto judge the severity of the symptoms (number orseverity of coughs, etc.) or of the change in the symp-toms, whether slight, moderate, great or none. Ineither of the latter judgements, numerical scales maybe employed where the highest number means theleast effect, if the symptom is assessed directly, or thegreatest effect ifchange is beingjudged. Alternativelyresults have also been expressed as a percentage ofthe group of patients reporting, according to thecriterion employed. All of these methods have beenused in the evaluation of antitussives and areprobably best illustrated with specific results in theevaluation of codeine (see below).Davenport (1938) mentioned the unsatisfactory use
of kymographic recording of chest movements fordetermination of the frequency of coughing. Graven-stein, Devloo & Beecher (1954) introduced a soundrecorder, connected to a microphone, from whichnumbers of bouts or numbers of individual coughscould be counted. The sound-induced electrical im-pulses were registered kymographically. This auto-matic record correlated well with that of a personmonitoring the cough by direct count. With minorvariations the method has been employed by Krug(1964), Kleibel (1964), Kleibel, Steinhoff & Wild(1965), Sevelius & Colmore (1967), and others.Woolf & Rosenberg (1964) used a tape-recorder toregister the actual sound of the cough, and this hadthe advantage for recording over prolonged periodsthat the on-off switch was automatically operated bythe sound. Others have overcome the prolongedobservation difficulty by restricting the record to aspecified period, uniform from day to day and basedupon survey of the coughing pattern throughout the24 hours.The subjective and objective approaches to evalu-
ation of antitussive action have been compared withdifferent results. Gravenstein, Devloo & Beecher(1954) could not detect changes in cough counts toback up judgement of an antitussive effect of codeinecompared with placebo. Nicolis & Pasquariello(1962a, 1962b) recorded a significant reduction in thenumber of coughs by codeine versus placebo whenthe patients' judgement of effect, based on a four-point scale, showed no difference. In another study,however, Pasquariello & Nicolis (1962) showed goodcorrelation between patients' drug preference and
reduction in bouts of coughing. Woolf& Rosenberg(1964) also compared their patients' judgement ofchange in coughing with the results recorded auto-matically. An actual reduction in the number ofcoughs by 50% was recognized in only 36 of 90 cases.The authors concluded that the majority of thepatients did not appreciate the extent to which theircough varied from day to day and were frequentlyunaware of the effect of antitussive preparations.Gravenstein, Devloo & Beecher (1954) reached theopposite conclusion, that their patients felt better andthought they coughed less.
Various methods of statistical analysis of results,whether subjective or objective, have been used. Itmay be of interest to mention Armitage's sequentialanalysis, since its applicability was first demonstratedin an antitussive study (Snell & Armitage, 1957). Ithas the advantage of making evaluation possiblewhile the trial proceeds, avoiding undue continuationor premature termination. No doubt conflictingresults in clinical trials are influenced by using toofew patients. Improper dosage selection can alsobias the results by destroying the double-blind featurethrough the appearance of recognizable effects unre-lated to the one under examination.
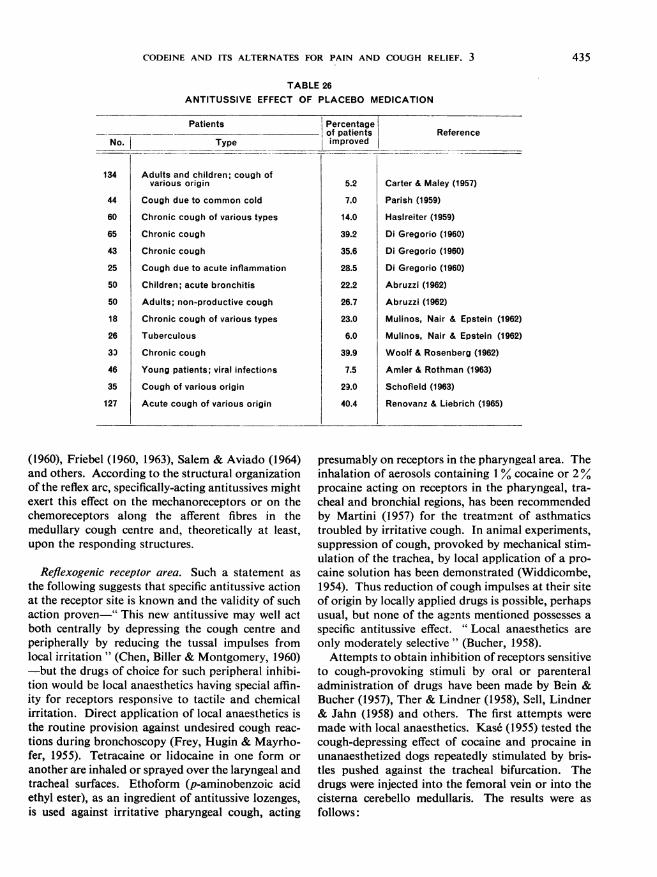
Finally, it is of interest to review the role of theplacebo and the degree ofeffect which it has producedin antitussive testing. Table 26 summarizes someplacebo results, and is restricted to those reportswhich could be interpreted in terms of the percentageof the group of patients who improved. From thesedata an average analgesic effect of placebo of 22.8%may be calculated-somewhat less than the averagefigure (35.2%) calculated by Beecher (1955) as theaverage percentage analgesic effect of placebo. Oneother point was brought out by Renovanz & Liebrich(1965). On the basis of the patients' judgement ofimprovement in frequency and intensity of coughing,placebo was less effective when compared withcodeine, 29.0% and 32.3 % reductions in number andintensity of cough, respectively, than when comparedwith no medication, 40.4% and 60.9% reductions innumber and intensity.
PHARMACOLOGICAL COMPONENTS OF THE ANTITUSSIVEEFFECT
Specific cough-depressant actions
The mechanisms of antitussive action have beendiscussed extensively by Bucher (1958), Bickerman
434
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
TABLE 26ANTITUSSIVE EFFECT OF PLACEBO MEDICATION
Patients IPercentageof patients
Type improved
Adults and children; cough ofvarious origin
Cough due to common cold
Chronic cough of various types
Chronic cough
Chronic cough
Cough due to acute inflammation
Children; acute bronchitis
Adults; non-productive cough
Chronic cough of various types
Tuberculous
Chronic cough
Young patients; viral infections
Cough of various origin
Acute cough of various origin
5.2
7.0
14.0
39.2
35.6
28.5
22.2
26.7
23.0
6.0
39.9
7.5
29.0
40.4
Reference
Carter & Maley (1957)
Parish (1959)
Haslreiter (1959)
Di Gregorio (1960)
Di Gregorio (1960)
Di Gregorio (1960)
Abruzzi (1962)
Abruzzi (1962)
Mulinos, Nair & Epstein (1962)
Mulinos, Nair & Epstein (1962)
Woolf & Rosenberg (1962)
Amler & Rothman (1963)
Schofield (1963)
Renovanz & Liebrich (1965)
(1960), Friebel (1960, 1963), Salem & Aviado (1964)and others. According to the structural organizationof the reflex arc, specifically-acting antitussives mightexert this effect on the mechanoreceptors or on thechemoreceptors along the afferent fibres in themedullary cough centre and, theoretically at least,upon the responding structures.
Reflexogenic receptor area. Such a statement as
the following suggests that specific antitussive actionat the receptor site is known and the validity of suchaction proven-" This new antitussive may well actboth centrally by depressing the cough centre andperipherally by reducing the tussal impulses fromlocal irritation " (Chen, Biller & Montgomery, 1960)-but the drugs of choice for such peripheral inhibi-tion would be local anaesthetics having special affin-ity for receptors responsive to tactile and chemicalirritation. Direct application of local anaesthetics isthe routine provision against undesired cough reac-
tions during bronchoscopy (Frey, Hugin & Mayrho-fer, 1955). Tetracaine or lidocaine in one form or
another are inhaled or sprayed over the laryngeal andtracheal surfaces. Ethoform (p-aminobenzoic acidethyl ester), as an ingredient of antitussive lozenges,is used against irritative pharyngeal cough, acting
presumably on receptors in the pharyngeal area. Theinhalation of aerosols containing 1 % cocaine or 2%procaine acting on receptors in the pharyngeal, tra-cheal and bronchial regions, has been recommendedby Martini (1957) for the treatment of asthmaticstroubled by irritative cough. In animal experiments,suppression of cough, provoked by mechanical stim-ulation of the trachea, by local application of a pro-caine solution has been demonstrated (Widdicombe,1954). Thus reduction of cough impulses at their siteof origin by locally applied drugs is possible, perhapsusual, but none of the agents mentioned possesses a
specific antitussive effect. " Local anaesthetics are
only moderately selective" (Bucher, 1958).Attempts to obtain inhibition of receptors sensitive
to cough-provoking stimuli by oral or parenteraladministration of drugs have been made by Bein &Bucher (1957), Ther & Lindner (1958), Sell, Lindner& Jahn (1958) and others. The first attempts were
made with local anaesthetics. Kase (1955) tested thecough-depressing effect of cocaine and procaine inunanaesthetized dogs repeatedly stimulated by bris-tles pushed against the tracheal bifurcation. Thedrugs were injected into the femoral vein or into thecistema cerebello medullaris. The results were as
follows:
No.
134
44
60
65
43
25
50
50
18
26
30
46
35
127
435
N. B. EDDY AND OTHERS
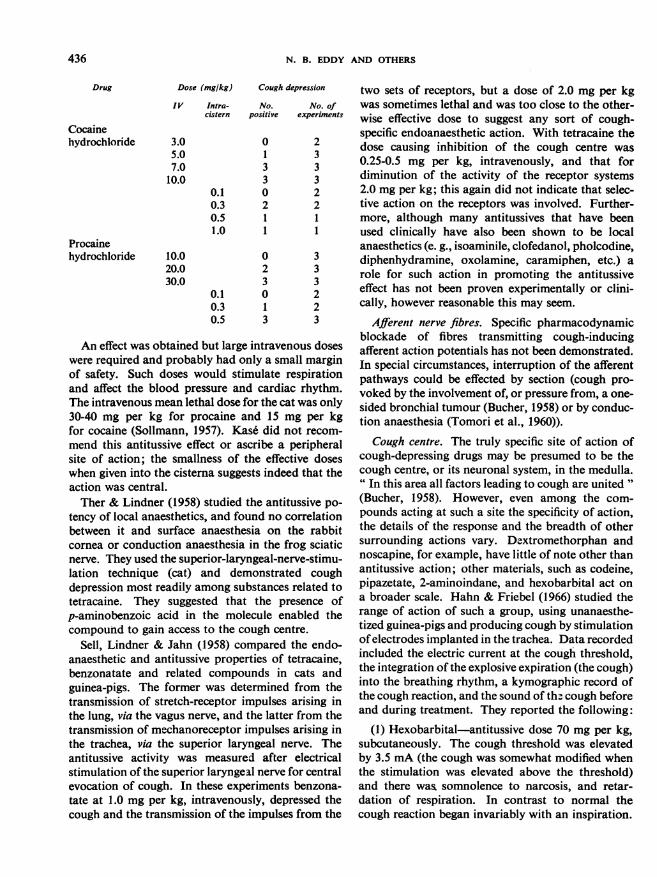
Dose (mg/kg) Cough depression two sets of receptors, but a dose of 2.0 mg per kgIV Intra- No. No. of was sometimes lethal and was too close to the other-
cistern positive experiments wise effective dose to suggest any sort of cough-specific endoanaesthetic action. With tetracaine the
3.0 0 2 dose causing inhibition of the cough centre was
7.0 3 3 0.25-0.5 mg per kg, intravenously, and that for0.0 3 3 diminution of the activity of the receptor systems
0.1 0 2 2.0 mg per kg; this again did not indicate that selec-0.3 2 2 tive action on the receptors was involved. Further-0.5 1 1 more, although many antitussives that have been1.0 1 1 used clinically have also been shown to be local
anaesthetics (e. g., isoaminile, clofedanol, pholcodine,0.0 0 3 diphenhydramine, oxolamine, caramiphen, etc.) a0.0 2 3 role for such action in promoting the antitussive
0.1 0 2 effect has not been proven experimentally or clini-0.3 1 2 cally, however reasonable this may seem.0.5 3 3 Afferent nerve fibres. Specific pharmacodynamic
blockade of fibres transmitting cough-inducingafferent action potentials has not been demonstrated.In special circumstances, interruption of the afferentpathways could be effected by section (cough pro-
voked by the involvement of, or pressure from, a one-sided bronchial tumour (Bucher, 1958) or by conduc-tion anaesthesia (Tomori et al., 1960)).
Cough centre. The truly specific site of action ofcough-depressing drugs may be presumed to be thecough centre, or its neuronal system, in the medulla." In this area all factors leading to cough are united "(Bucher, 1958). However, even among the com-
pounds acting at such a site the specificity of action,the details of the response and the breadth of othersurrounding actions vary. Dextromethorphan andnoscapine, for example, have little of note other thanantitussive action; other materials, such as codeine,pipazetate, 2-aminoindane, and hexobarbital act on
a broader scale. Hahn & Friebel (1966) studied therange of action of such a group, using unanaesthe-tized guinea-pigs and producing cough by stimulationofelectrodes implanted in the trachea. Data recordedincluded the electric current at the cough threshold,the integration of the explosive expiration (the cough)into the breathing rhythm, a kymographic record ofthe cough reaction, and the sound of the cough beforeand during treatment. They reported the following:
(1) Hexobarbital-antitussive dose 70 mg per kg,subcutaneously. The cough threshold was elevatedby 3.5 mA (the cough was somewhat modified whenthe stimulation was elevated above the threshold)and there was somnolence to narcosis, and retar-dation of respiration. In contrast to normal thecough reaction began invariably with an inspiration.
An effect was obtained but large intravenous doseswere required and probably had only a small marginof safety. Such doses would stimulate respirationand affect the blood pressure and cardiac rhythm.The intravenous mean lethal dose for the cat was only30-40 mg per kg for procaine and 15 mg per kgfor cocaine (Sollmann, 1957). Kas6 did not recom-
mend this antitussive effect or ascribe a peripheralsite of action; the smallness of the effective doseswhen given into the cisterna suggests indeed that theaction was central.Ther & Lindner (1958) studied the antitussive po-
tency of local anaesthetics, and found no correlationbetween it and surface anaesthesia on the rabbitcornea or conduction anaesthesia in the frog sciaticnerve. They used the superior-laryngeal-nerve-stimu-lation technique (cat) and demonstrated coughdepression most readily among substances related totetracaine. They suggested that the presence ofp-aminobenzoic acid in the molecule enabled thecompound to gain access to the cough centre.
Sell, Lindner & Jahn (1958) compared the endo-anaesthetic and antitussive properties of tetracaine,benzonatate and related compounds in cats andguinea-pigs. The former was determined from thetransmission of stretch-receptor impulses arising inthe lung, via the vagus nerve, and the latter from thetransmission of mechanoreceptor impulses arising inthe trachea, via the superior laryngeal nerve. Theantitussive activity was measured after electricalstimulation of the superior laryngeal nerve for centralevocation of cough. In these experiments benzona-tate at 1.0 mg per kg, intravenously, depressed thecough and the transmission of the impulses from the
Drug
Cocainehydrochloride
Procainehydrochloride
1
123'
436
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
The subsequent reduction in the cough response wasslowed; in some cases animals coughed for threeseconds after interruption of the cough-provokingcurrent. A broadening of the kymographic V-recordof the cough further illustrated the retardation ofthe response. Signs of closure of the glottis as apart of the event disappeared and the sound of thecough was weakened.
(2) Aminoindane-antitussive dose 14.5 mg per kg,subcutaneously. The cough threshold rose quicklyby 1.5 mA and showed no tendency to recover duringthe next three hours. Respiratory frequency wasincreased and there was motor excitement, piloerec-tion, secretion of tears and saliva. The explosiveexpiration began during the expiratory phase of thebreathing cycle more frequently than is normal; itwas never integrated into the breathing cycle assometimes occurred before drugging. The sound ofthe cough increased and the kymographic recordbecame irregular and broader in form.
(3) Codeine phosphate-antitussive dose 15.4 mgper kg, subcutaneously. The cough threshold waselevated by 0.5 mA for about three hours (a largerdose of 30.8 mg per kg elevated the threshold by0.9 mA). The noise of the cough was weakened andits kymographic record was simplified but not broad-ened.
(4) Pipazetate-antitussive dose 14.5 mg per kg,subcutaneously. The cough threshold was elevatedby about 1.6 mA, and was still above normal afterthree hours. The noise of the cough was decreased;the record was irregular and sometimes broader.
(5) Dextromethorphan-antitussive dose 26.0 mgper kg, subcutaneously. The cough threshold wasraised by 0.4 mA for three hours. Respiration wasunchanged. The explosive expiration began morefrequently (18%) than is normal in the expiratoryphase of the breathing cycle, and in 14% of cases atthe very end of expiration. The record showednumerous irregularities and broadening. The noiseof the cough was decreased only during the first20 minutes.
Thus these compounds produced several differenteffects, only one common to them all, an elevationof the cough threshold, which could be overcome byincreasing the strength of the stimulation. The sen-sitivity of the centre is decreased but it is not para-lysed. Based upon their experimental results Friebel& Hahn (1966) and Hahn & Friebel (1966) concludedthat the centre temporarily loses the ability to sum-
mate the incoming stimuli and that this failure ofsummation is the principal effect of the antitussivecompound, though it may also sometimes changethe character or form of the response.Some compounds affect the correlation between
the respiratory cycle and cough. With hexobarbital,as was noted, the cough was initiated with an inspira-tion; the same was true in barbiturate-treated cats(Kroepfli, 1950). In untreated cats, 16% of electric-ally-provoked cough reactions began without theintroductory inspiration.
If the central action of antitussives were directedprimarily against the stimulus-summating functionof the centre, this would explain the equal therapeuticeffectiveness of these drugs against most forms ofirritating cough. Codeine, dextromethorphan, pipa-zetate, and benzonatate seem to be equally satisfac-tory whether the cough arises from acute or chronicbronchitis, tuberculosis, emphysematous bronchitis,asthmatic bronchitis or bronchial carcinoma; thedoses necessary for diminution of the cough areabout equal, and this is understandable only if theyare acting uniformly on a central mechanism acti-vated by all kinds of cough. The clinical significanceof the other cough modifications described by Hahn& Friebel (1966) has not been clarified.
Efferent activating structures. Inhibition of coughthrough an effect on responding structures has beenclaimed for oxolamine (Silvestrini & Pozzatti, 1960)and sodium dibunate (DeVleeschhouwer, 1954) as apart of peripheral antitussive action. However, therespiratory centre is also in control of these structuresand differentiation is not possible.
Effects other than specific cough-depressant action
Cough-depressing substances, of course, exhibitother pharmacodynamic effects, which may be detect-able at the antitussive dosage level and which maypromote or even interfere with antitussive usefulness.
Respiratory effects, other than antitussive effects.B-nzonatate, tetracaine and related substances, ifinjected intravenously, diminish the spontaneousactivity of the pulmonary stretch receptors, thoughthe margin between effective and toxic doses is small(receptor-depressing doses in cats are between 0.5 and2.0 mg per kg whilst depression of blood pressure,temporary arrest of respiration, and ozcasional deathoccurs with doses of 2.0 or 3.0 mg per kg). Depres-sion of the pulmonary stretch receptors is probablynot significant in antitussive action. Cutting off im-pulses from these receptors from the vagus, below
437
438 N. B. EDDY AND OTHERS
the entrance of the superior laryngeal nerve, did notaffect the cough response to electrical stimulation ofthat nerve (Widdicombe, 1954; Sell, Lindner & Jahn,1958). Pholcodine enhanced the Hering-Brauer pul-monary-inflation reflex, which May & Widdicombe(1954) thought was secondary to bronchoconstrictionand indicated increased activity of the pulmonarystretch receptors, yet pholcodine was equivalent tocodeine as an antitussive.Many antitussives affect central regulation of res-
piration. Friebel & Kuhn (1962) and Hahn & Friebel(1966) demonstrated that hexobarbital decreasedrespiratory volume and frequency at doses belowthose which affected the cough reflex mechanism.Pentoxyverine 1 citrate, pipazetate and the piperidinederivative, L 2909, depressed the cough reflex at adose level which did not seem to affect respiration,but pipazetate would increase the respiratory depres-sant effect of hexobarbital. 2-Aminoindane stimula-ted respiration even when the respiratory centre wasdepressed by previous administration of hexobarbitaland its antitussive effectiveness equalled that ofcodeine (Friebel & Kuhn, 1962; Kuhn & Friebel,1960a, 1960b). Again these results support the sug-gestion that the respiratory centre, in its reactivity todrugs, is to a considerable extent independent of thecough centre, that depression or stimulation of res-piration may be independent of antitussive effective-ness (Eichler & Smiatek, 1940; Haas, 1955; LaBarre & Plisnier, 1959), and that the degree ofrespira-tory depression produced by many antitussives doesnot impair their antitussive usefulness at usual thera-neutic doses.
Analgesic effect. The virtually exclusive use of theopiates, or of analgesics related to morphine, forantitussive effect was interrupted by the observationsof Pellmont & Bachtold (1954) and Winter & Flata-ker (1954), which demonstrated, on the one hand,that the structurally related dextromethorphan, and,on the other hand, that the unrelated noscapine bothdepressed experimentally produced cough, althoughboth lacked analgesic action.Cough and pain are nociceptive warning signals
which can evoke reflex protective responses and whichare perceived as discomforts of greater or less degree.Antitussives and analgesics suppress the responseunder experimental conditions and make the per-son feel better by decreasing his awareness of thediscomfort, apart from the suppression of the res-ponse. This would seem to bring into play a similar
I Also known as carbetapentane.
mechanism for both types of relief, but antitussiveaction without analgesia implies a fundamental dif-ference in the mechanisms involved.
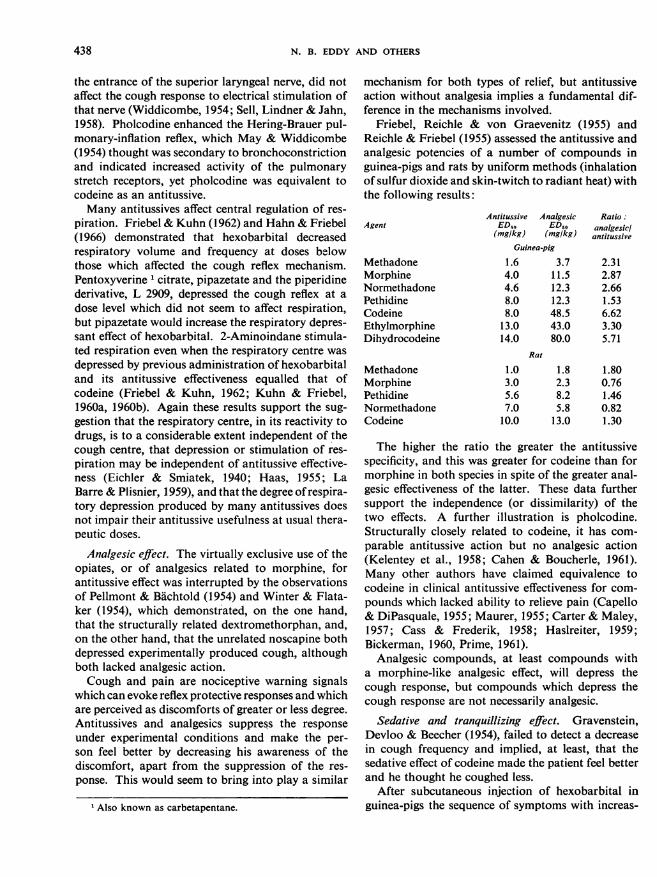
Friebel, Reichle & von Graevenitz (1955) andReichle & Friebel (1955) assessed the antitussive andanalgesic potencies of a number of compounds inguinea-pigs and rats by uniform methods (inhalationof sulfur dioxide and skin-twitch to radiant heat) withthe following results:
Antitussive Analgesic Ratio:Agent EDro ED,, analgesicl
(mg/kg) (mg/kg) antitussiveGuinea-pig
Methadone 1.6 3.7 2.31Morphine 4.0 11.5 2.87Normethadone 4.6 12.3 2.66Pethidine 8.0 12.3 1.53Codeine 8.0 48.5 6.62Ethylmorphine 13.0 43.0 3.30Dihydrocodeine 14.0 80.0 5.71
Rat
Methadone 1.0 1.8 1.80Morphine 3.0 2.3 0.76Pethidine 5.6 8.2 1.46Normethadone 7.0 5.8 0.82Codeine 10.0 13.0 1.30
The higher the ratio the greater the antitussivespecificity, and this was greater for codeine than formorphine in both species in spite of the greater anal-gesic effectiveness of the latter. These data furthersupport the independence (or dissimilarity) of thetwo effects. A further illustration is pholcodine.Structurally closely related to codeine, it has com-parable antitussive action but no analgesic action(Kelentey et al., 1958; Cahen & Boucherle, 1961).Many other authors have claimed equivalence tocodeine in clinical antitussive effectiveness for com-pounds which lacked ability to relieve pain (Capello& DiPasquale, 1955; Maurer, 1955; Carter & Maley,1957; Cass & Frederik, 1958; Haslreiter, 1959;Bickerman, 1960, Prime, 1961).
Analgesic compounds, at least compounds witha morphine-like analgesic effect, will depress thecough response, but compounds which depress thecough response are not necessarily analgesic.
Sedative and tranquillizing effect. Gravenstein,Devloo & Beecher (1954), failed to detect a decreasein cough frequency and implied, at least, that thesedative effect of codeine made the patient feel betterand he thought he coughed less.
After subcutaneous injection of hexobarbital inguinea-pigs the sequence of symptoms with increas-
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
ing dosage was sedation at 50 mg per kg (to anaesthe-sia), depression of respiration and depression ofcough at 77 mg per kg (Friebel & Kuhn, 1962). Isthe depression of cough in hexobarbital-treatedanimals a specific antitussive action or a part of thegeneral depression of reflexes? Hahn & Friebel(1966) observed, in guinea-pigs in which cough waselicited by electrical stimulation, that hexobarbitalat 70 mg per kg, subcutaneously, first caused sedation(sometimes with delirium) followed by decrease inrespiratory frequency and later, while in an anaesthe-tized, condition by a retardation and decrease in thecough response which, as anaesthesia declined, out-lasted the respiratory depression. Throughout theperiod under hexobarbital the cough was alwaysinitiated by inspiration, which was not the case inuntreated animals.
Tedeschi et al. (1959) found an ED50 of 13.7 mgper kg for pentobarbital sodium in unanaesthetizeddogs, for depression of cough due to mechanicalstimulation. However, the barbiturate was effectiveonly in doses which produced signs of neurologicaldeficit, marked ataxia and/or unconsciousness indi-cating that " pentobarbital acts as a non-selectiveantitussive agent ". The cough response of decere-brate cats to electrical stimulation has been abolishedby thiopental, 4-12 mg per kg, intravenously (Matal-lana & Borison, 1955).
Methaqualone, similar in its sedative effect to thebarbiturates, diminished by 50% the cough responseto electrical stimulation in narcotized cats at a doseof 4 mg per kg, intramuscularly (Boissier & Pagny,1960a, 1960b). Up to 40 mg per kg, it also had anantitussive effect in unanaesthetized guinea-pigs ex-posed to sulfur dioxide, without producing sedation.Certain hypnotics then may cause specific antitus-sive effects. A broader examination of the antitussivepotency of sedatives (hypnotics) is desirable to deli-neate better the relation between sedation and coughrelief.
Lorenz (1962) studied the sedative and antitussiveeffects of dipropylbarbituric acid, codeine, and a mix-ture of the two in guinea-pigs and cats. In anaesthe-tized cats, stimulated electrically, the antitussive effectof intravenous codeine was not increased by the addi-tion of the barbiturate. In unanaesthetized guinea-pigs, however, the cough reflex was depressed bysmaller doses of codeine in the mixture than whenit was given alone, subcutaneously or orally; thesedative effect of the barbiturate in the mixture wasalso enhanced. Whether this was potentiation of anti-tussive action or of sedation was not clarified.
In man, as in laboratory animals, narcosis abo-lishes the cough reflex; in deep narcosis the mecha-nism is paralysed. Barbiturates and other sedatives,in sleep-inducing doses, are not expected to act ascough depressants, though the sedation may be asuseful an adjunct to cough therapy in some circum-stances as simultaneous analgesia may be in others.
Neuroleptic effect. Chlorpromazine, a standardsubstance among neuroleptic compounds, and thio-ridazine act similarly, protecting against vomiting,having moderate anticholinergic, adrenolytic andantihistaminic properties, and are both credited withstrengthening the pharmacodynamic effects of opi-ates, barbiturates and other sedatives and anaesthe-tics. Both substances, according to Boissier & Pagny(1960a, 1960b), showed a good antitussive effect inguinea-pigs subjected to sulfuric acid aerosol. Pro-methazine, which is weaker in its neuroleptic potency,also depressed the cough reflex at higher doses. Theauthors believed that non-specific central depressantproperties were mainly responsible for the cough-depressing effect. Kase & Yuizono (1959) testedsome compounds structurally related to chlorproma-zine and found chlorpromazine in dogs, at 20 mg perkg intravenously, sometimes slightly effective, per-phenazine, prochlorperazine and other phenothia-zines more definitely effective against cough at equalor smaller doses. Thus powerful neuroleptics affectthe cough-reflex mechanism and act in this respectlike the opiate analgesics; absence of neurolepticaction in substances related to chlorpromazine doesnot exclude antitussive effectiveness.Tomori et al. (1960) studied the effect of neurolep-
tics on tracheal and bronchial reflexes in man. Tenpatients under (1) ether-oxygen anaesthesia, (2)autonomic blockade with the " lytic cocktail " or (3)blockade plus hypothermia, were stimulated mechan-ically in the lower trachea. Signs of positive reflexactivity were coughing and apnoea. A positive res-ponse failed to occur in 12% in (1), 26.5% in (2) and46.9% in (3). The mechanism of the cough de-pressing effect is a matter for speculation, since thecomposition of the " lytic cocktail " was not dis-closed but may have contained chlorpromazine orpethidine or both. There may have been a deepeningof the ether narcosis or strengthening of the antitus-sive action of pethidine.
Ganglionic blockade. Three observations may jus-tify a consideration of whether ganglionic blockadecan influence the cough reaction. Tiffeneau (1955)found that inhalation of hexamethonium instantly
8
439
440 N. B. EDDY AND OTHERS
stopped the excessive cough reactions producedin man by inhalation of acetylcholine aerosol. Hillis& Kelly (1951) suppressed the cough, produced inhuman volunteers by intravenous injection of lobe-line, also by using hexamethonium. Korpas, Tomori& Ivanca (1957) studied the cough-depressing effectof pentamethonium in cats. Doses, which were undersome experimental conditions slightly effectiveagainst cough reactions, were considerably higherthan those which paralyse the cervical ganglion.Tests with quatemary salts of antitussive agents gaveno convincing evidence that ganglionic blocking con-tributes to the cough-depressing effect.
Local anaesthetic effect. The role of local anaesthe-sia in antitussive action has been discussed (see above,Part 3, section headed " Reflexogenic receptor area ").
Spasmolytic and spasmogenic effects. The evidencein this connexion may be summarized briefly.Some antihistamines depress experimental cough
in laboratory animals and in man (see Part 4). How-ever, Boissier & Pagny (1960a, 1960b) concluded thatantihistamines were not antitussives per se. Theycould not demonstrate a parallelism of antihistaminicand antitussive potencies.
Atropine was tested in unanaesthetized dogs byKase (1955). It had no cough-depressing action indoses of 0.1-5.0 mg per kg, intravenously. Silvestrini& Maffii (1959) observed no significant effect ofatropine on the acrolein-induced cough in guinea-pigs; the doses used were 1.0-5.0 mg per kg, sub-cutaneously. Bobb & Ellis (1951) treated with atro-pine and curare unanaesthetized dogs, in which thevagus loop was electrically stimulated: both wereineffective.Domenjoz (1952), Kase (1955) and Hara & Yanau-
ra (1959) showed no definitive effect of papaverinein dogs and cats, though the doses were high in com-parison with that of codeine. This is discussed morefully in Part 4.
Isoaminile relaxes other smooth muscle, isolatedrabbit uterus and intestine, and inhibits the peristal-tic reflex (Krause, 1958; Graham, 1962). Clofedanoland nicodicodine relaxed the rabbit duodenum andrelieved spasms induced by barium chloride or acetyl-choline (Cahen& Boucherle, 1964, 1965). Oxolaminewas about as active as papaverine in its inhibitoryeffect on the tracheal chain preparation (Silvestrini& Pozzatti, 1960; Balea & Buret, 1964). Caramiphenprevented or retarded bronchoconstriction provokedin guinea-pigs by injection or inhalation of acetyl-choline or histamine (Plisnier, 1957). Pentoxyverine
showed similar properties. Oxeladin exerted papa-verine-like spasmolytic action on the isolated ileum(David, Leith-Ross & Vallance, 1957) and on thetracheal chain preparation (Ozawa et al., 1962). Thethiambutene derivative, AT-327, had little spasmo-lytic effect (Kase et al., 1959).
Epinephrine caused no depression of the coughreflex, mechanically stimulated in unanaesthetizeddogs (Kase, 1955), but ephedrine, less effective as abronchodilator, depressed the cough in 6 out of 12dogs, at a dose of 5.0 mg per kg, intravenously.Increasing the dose to 10-20 mg per kg did not pro-duce an effect in the dogs which did not respond.Methamphetamine' was more centrally exciting thanephedrine, and had antitussive (Kase, 1955) andanalgesic (Suter, 1951) properties.
Codeine, as well as morphine, causes slight bron-choconstriction (Krueger, Eddy & Sumwalt, 1943;Konzett, 1955; La Barre & Plisnier, 1959) and thecodeine bronchospasm can be relieved partly byisoprenaline (Friebel & Kuhn, 1962). Pholcodinealso has a bronchoconstrictor effect comparable tothat of codeine (Plisnier, 1960). Antitussive potencywould not appear to be impaired, though warningswith respect to impairment of respiratory functionhave been expressed, especially if a bronchospasticcondition already exists.
All of this does not suggest any significant relation-ship of spasmolytic or spasmogenic effects to anti-tussive action, though under some circumstances apotent bronchodilator may help in the relief of anassociated condition.
Augmentation and reduction of bronchial secretion.Noscapine, 1.0-2.0 mg per kg, intravenously, in-creased bronchial secretion in anaesthetized rabbits(Konzett & Rothlin, 1954; La Barre & Plisnier, 1959;Plisnier & Hernalsteen, 1959). The dose was sufficientto depress the cough. Caramiphen ethane disulfonatealso increased bronchial secretion in the same type ofexperiment at 6.0 mg per kg, intravenously (Plisnier,1957). Silomat, 40 mg per kg intravenously, increasedbronchial secretion in rabbits by 20-45% for 2-6hours (Engelhorn, 1960).
Pholcodine, orally or subcutaneously in doses of0.1-50 mg per kg, did not cause a significant changein output of respiratory-tract fluid; nor did diphen-hydramine (Bidwell & Boyd, 1952).
Bedell & Seebohm (1959) warned against the useof codeine in patients with emphysema because ofits drying effect. Boyd & Trainer (quoted by Boyd,
1 Also known as methylpropamine.
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
1954) recorded a decrease in bronchial secretion afterdextromethorphan. Clofedanol (Boyd & Boyd, 1960)and pentoxyverine (Levis et al., 1955) decreased thesecretion of saliva and presumably of bronchial fluid.There is no clinical evidence that antitussive ther-
apy is significantly affected by the changes in secre-tion described.
ANTITUSSIVE ACTION OF CODEINE
Animal experimentsMany reports of attempts to evaluate the antitus-
sive effectiveness of codeine in animals are summa-rized in Table 27. These have been arranged byspecies and by the method of cough production,though the latter has not been uniform in detail,even when the cough-provoking stimulus was said tobe the same. Some of these variations have beendiscussed previously (see Part 3, section headed" Measurement of antitussive potency in animalexperiments "). Also the effective doses for the mostpart are indicative only of reduction or depression ofthe cough of varying degree, an ED50 having beencalculated only in rare instances (those doses aremarked in Table 27). Consequently, doses rangewidely, even for similar methods and species, from10 to 26 mg, subcutaneously or intraperitoneally, inmice, rats and guinea-pigs with irritant vapourinhalation, but calculated ED50s vary widely also,10 mg per kg and 13.5 mg per kg, subcutaneously, inrats, 25 mg per kg by the same route in guinea-pigswith sulfur dioxide inhalation. If ammonia vapourwas used in guinea-pigs the effective dose was only0.3 mg per kg, subcutaneously. Even so the dose hadto be increased remarkably, to 12 mg per kg, if thedrug was given orally. In rabbits also, with cough pro-duced by mechanical stimulation, there was a consid-erable ratio between oral and parenteral effectivedoses. In cats there was very wide variation ineffective dosage. Electrical stimulation and intra-venous administration were commonly used in thisspecies but mostly in anaesthetized animals. Theanaesthetic, usually a barbiturate, possessing in itselfsome cough-depressing action (see above, Part 3, sec-tion headed " Sedative and tranquillizing effect ")might be in part responsible for these variations,because of differences in depth of anaesthesia, butthere are many other variables in these experiments.The sensitivity of dogs to the cough-depressing actionof codeine appears to be high and more uniform,with a dose range of only 0.5-7.5 mg per kg forvarious procedures and routes of administration.
Perhaps with greater significance for the therapeu-tic use of codeine in man, it would be interesting toknow if codeine could depress or abolish cough, inanimals, which occurred spontaneously in bronchitis,for example. Stefko, Denzel & Hickey (1961) report-ed suppression of cough due to upper respiratoryinfection, in a dog for 30 minutes with 1.0 mg per kgand for 38 minutes with 2.0 mg per kg, orally. Exper-imentally produced cough in dogs has been abolishedby codeine, if the conditions were adequate, for 40minutes with 4.0 mg per kg, orally, for example,when the cough was elicited by electrical stimulationof the trachea. Chen, Biller & Montgomery (1960)have reported complete suppression of cough pro-duced in dogs by chemical stimulation.
Other authors who have attempted to establishdose-effect relationships have not been successful inobtaining 100% suppression of experimentally in-duced cough (Kdllquist & Melander, 1957; Silves-trini & Maffii, 1959; Engelhorn, 1960). The explana-tion may lie in the experiments of Rosiere, Winder& Wax (1956) which showed that complete inhibitionof cough could be overcome by intensifying thecough-provoking stimulation, but that stronger stim-ulation could be overcome only to a certain extentby increasing the dose of codeine.
Onset and duration of action of codeine in relationto experimentally induced cough in animals havebeen studied by Winter & Flataker (1954), Kas6(1955), Chen, Biller & Montgomery (1959), Engel-horn (1960), Stefko, Denzel & Hickey (1961), Kraus-haar, Schunk & Thym (1964), Hahn & Friebel (1966),and others. In conscious dogs, for example, somecough-depressing action has been observed 15 min-utes after oral administration, peaks of action at45-60 minutes after ingestion (Chen, Biller & Mont-gomery, 1959; Stefko, Denzel & Hickey, 1961) anda duration of action mainly dependent upon the doseof codeine but usually not exceeding three hours.
Repetition of codeine doses at short intervals wasfollowed by tolerance to antitussive action (Kase,1955; Friebel & Kuhn, 1964). In the experiments ofKase, dogs were injected intravenously daily. Theinitial dose of 10 mg per kg depressed coughing for20-30 minutes on the first day; the same dose wasineffective on the 14th day of administration. Thecough-depressing effect, which reappeared when thedose was increased to 15 and 20 mg per kg, wasreduced again in 4-10 days. Friebel & Kuhn treatedguinea-pigs and rats with codeine, subcutaneously,three times a day for six to seven weeks. The dailydose was increased from 20 to 110 mg per kg and
441
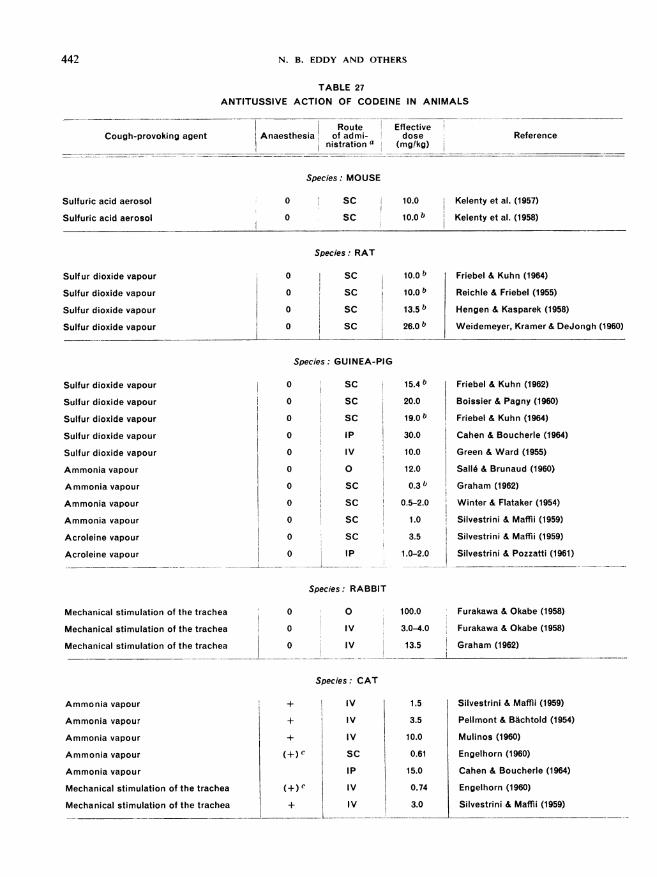
442 N. B. EDDY AND OTHERS
TABLE 27
ANTITUSSIVE ACTION OF CODEINE IN ANIMALS
Cough-provoking agentRoute Effective
Anaesthesia of admi- dosenistration a (mg/kg)
Species: MOUSE
Sulfuric acid aerosol
Sulfuric acid aerosol
0
0
SC
SC
10.0 Kelenty et al. (1957)
1 Kelenty et al. (1958)
Species: RAT
Sulf ur dioxide vapour
Sulfur dioxide vapour
Sulfur dioxide vapour
Sulfur dioxide vapour
Friebel & Kuhn (1964)
Reichle & Friebel (1955)
Hengen & Kasparek (1958)
Weidemeyer, Kramer & DeJongh (1960)
Sulfur dioxide vapour
Sulfur dioxide vapour
Sulfur dioxide vapour
Sulfur dioxide vapour
Sulfur dioxide vapour
Ammonia vapour
Ammonia vapour
Ammonia vapour
Ammonia vapour
Acroleine vapour
Acroleine vapour
Species: GUINEA-PIG
0 SC 15.4 b
0 SC 20.0
0 SC 19.0 b
0 IP 30.0
0 IV 10.0
0 0 12.0
0 SC 0.3 b
0 SC 0.5-2.0
0 SC 1.0
0 SC 3.5
0 IP 1.0-2.0
Friebel & Kuhn (1962)
Boissier & Pagny (1960)
Friebel & Kuhn (1964)
Cahen & Boucherle (1964)
Green & Ward (1955)
Salle & Brunaud (1960)
Graham (1962)
Winter & Flataker (1954)
Silvestrini & Maffii (1959)
Silvestrini & Maffli (1959)
Silvestrini & Pozzatti (1961)
Species: RABBIT
Mechanical stimulation of the trachea
Mechanical stimulation of the trachea
Mechanical stimulation of the trachea
0 0
0 IV
0 IV
100.0 Furakawa & Okabe (1958)
3.0-4.0 Furakawa & Okabe (1958)
13.5 Graham (1962)-~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Species: CAT
Ammonia vapour
Ammonia vapour
Ammonia vapour
Ammonia vapour
Ammonia vapour
Mechanical stimulation of the trachea
Mechanical stimulation of the trachea
+) c
+) c
IV
IV
IV
SC
IP
IV
IV
1.5
3.5
10.0
0.61
15.0
0.74
3.0
Silvestrini & Maffli (1959)
Pellmont & Bachtold (1954)
Mulinos (1960)
Engelhorn (1960)
Cahen & Boucherle (1964)
Engelhorn (1960)
Silvestrini & Maffli (1959)
Reference
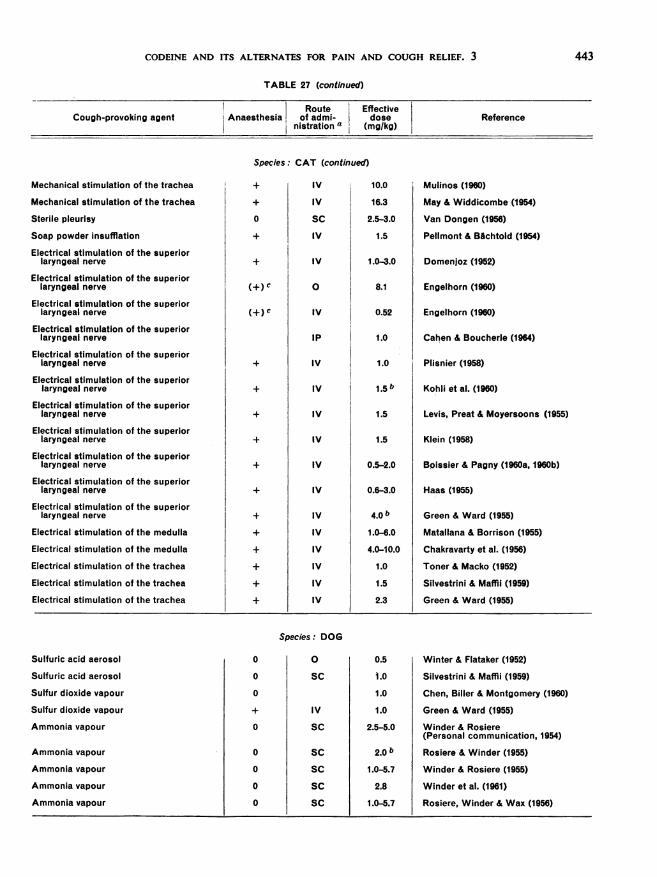
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
TABLE 27 (continued)
Route EffectiveCough-provoking agent Anaesthesia of admi- dose ReferenceI nistration a (mg/kg)
Species: CAT (continued)
Mechanical stimulation of the trachea
Mechanical stimulation of the trachea
Sterile pleurisy
Soap powder insufflation
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the superiorlaryngeal nerve
Electrical stimulation of the medulla
Electrical stimulation of the medulla
Electrical stimulation of the trachea
Electrical stimulation of the trachea
Electrical stimulation of the trachea
+
(+)c
+
+
IV
IV
SC
IV
IV
0
IV
IP
IV
IV
IV
IV
IV
IV
IV
IV
IV
IV
IV
IV
10.0
16.3
2.5-3.0
1.5
1.0-3.0
8.1
0.52
1.0
1.0
1.5 b
1.5
1.5
0.5-2.0
0.6-3.0
4.0 b
1.0-6.0
4.0-10.0
1.0
1.5
2.3
Mulinos (1960)
May & Widdicombe (1954)
Van Dongen (1956)
Pellmont & BAchtold (1954)
Domenjoz (1952)
Engelhorn (1960)
Engelhorn (1960)
Cahen & Boucherle (1964)
Plisnier (1958)
Kohli et al. (1960)
Levis, Preat & Moyersoons (1955)
Klein (1958)
Boissier & Pagny (1960a, 1960b)
Haas (1955)
Green & Ward (1955)
Matallana & Borrison (1955)
Chakravarty et al. (1956)
Toner & Macko (1952)
Silvestrini & Maffli (1959)
Green & Ward (1955)
Species: DOG
Sulfuric acid aerosol
Sulfuric acid aerosol
Sulfur dioxide vapour
Sulfur dioxide vapour
Ammonia vapour
Ammonia vapour
Ammonia vapour
Ammonia vapour
Ammonia vapour
0
0
0
0
0
0
0
0
0
SC
IV
SC
SC
SC
SC
SC
0.5
i.0
1.0
1.0
2.5-5.0
2.0 b
1.0-5.7
2.8
1.0-5.7
Winter & Flataker (1952)
Silvestrini & Maffli (1959)
Chen, Biller & Montgomery (1960)
Green & Ward (1955)
Winder & Rosiere(Personal communication, 1954)
Rosiere & Winder (1955)
Winder & Rosiere (1955)
Winder et al. (1961)
Rosiere, Winder & Wax (1956)
443
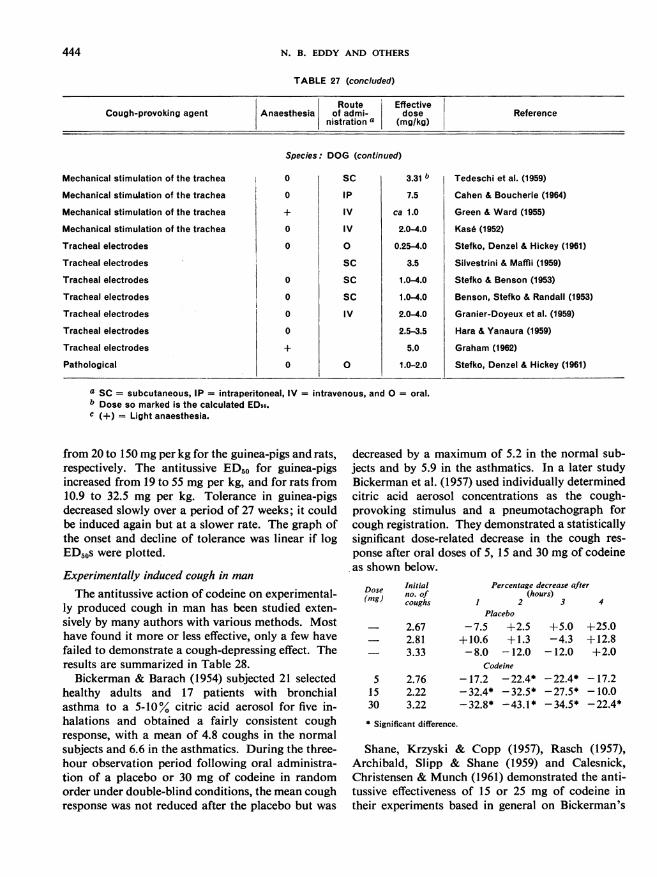
N. B. EDDY AND OTHERS
TABLE 27 (concluded)
Route EffectiveCough-provoking agent Anaesthesia of admi- dose Reference
nistration a (mg/kg)
Species: DOG (continued)
Mechanical stimulation of the trachea 0 SC 3.31 b Tedeschi et al. (1959)
Mechanical stimulation of the trachea 0 IP 7.5 Cahen & Boucherle (1964)
Mechanical stimulation of the trachea + IV ca 1.0 Green & Ward (1955)
Mechanical stimulation of the trachea 0 IV 2.0-4.0 Kas6 (1952)
Tracheal electrodes 0 0 0.25-4.0 Stefko, Denzel & Hickey (1961)
Tracheal electrodes SC 3.5 Silvestrini & Maffii (1959)
Tracheal electrodes 0 SC 1.0-4.0 Stefko & Benson (1953)
Tracheal electrodes 0 SC 1.04.0 Benson, Stefko & Randall (1953)
Tracheal electrodes 0 IV 2.04.0 Granier-Doyeux et al. (1959)
Tracheal electrodes 0 2.5-3.5 Hara & Yanaura (1959)
Tracheal electrodes + 5.0 Graham (1962)
Pathological 0 0 1.0-2.0 Stefko, Denzel & Hickey (1961)
a SC = subcutaneous, IP = intraperitoneal, IV = intravenous, and 0 = oral.b Dose so marked is the calculated EDso.c (+) = Light anaesthesia.
from 20 to 150 mg per kg for the guinea-pigs and rats,respectively. The antitussive ED50 for guinea-pigsincreased from 19 to 55 mg per kg, and for rats from10.9 to 32.5 mg per kg. Tolerance in guinea-pigsdecreased slowly over a period of 27 weeks; it couldbe induced again but at a slower rate. The graph ofthe onset and decline of tolerance was linear if logED50s were plotted.
Experimentally induced cough in manThe antitussive action of codeine on experimental-
ly produced cough in man has been studied exten-sively by many authors with various methods. Mosthave found it more or less effective, only a few havefailed to demonstrate a cough-depressing effect. Theresults are summarized in Table 28.Bickerman & Barach (1954) subjected 21 selected
healthy adults and 17 patients with bronchialasthma to a 5-10% citric acid aerosol for five in-halations and obtained a fairly consistent coughresponse, with a mean of 4.8 coughs in the normalsubjects and 6.6 in the asthmatics. During the three-hour observation period following oral administra-tion of a placebo or 30 mg of codeine in randomorder under double-blind conditions, the mean coughresponse was not reduced after the placebo but was
decreased by a maximum of 5.2 in the normal sub-jects and by 5.9 in the asthmatics. In a later studyBickerman et al. (1957) used individually determinedcitric acid aerosol concentrations as the cough-provoking stimulus and a pneumotachograph forcough registration. They demonstrated a statisticallysignificant dose-related decrease in the cough res-ponse after oral doses of 5, 15 and 30 mg of codeineas shown below.
Dose Initial(mg) no. of(m) coughs
51530
Percentage decrease aft(hours)
1 2 3Placebo
2.67 - 7.5 +2.52.81 +10.6 +1.33.33 - 8.0 -12.0
Codeine
2.76 - 17.2 - 22.4*2.22 - 32.4* - 32.5*3.22 -32.8* -43.1*
+5.0-4.3-12.0
-22.4*- 27.5*-34.5*
er
4
+25.0+12.8+2.0
-17.2-10.0-22.4*
* Significant difference.
Shane, Krzyski & Copp (1957), Rasch (1957),Archibald, Slipp & Shane (1959) and Calesnick,Christensen & Munch (1961) demonstrated the anti-tussive effectiveness of 15 or 25 mg of codeine intheir experiments based in general on Bickerman's
444
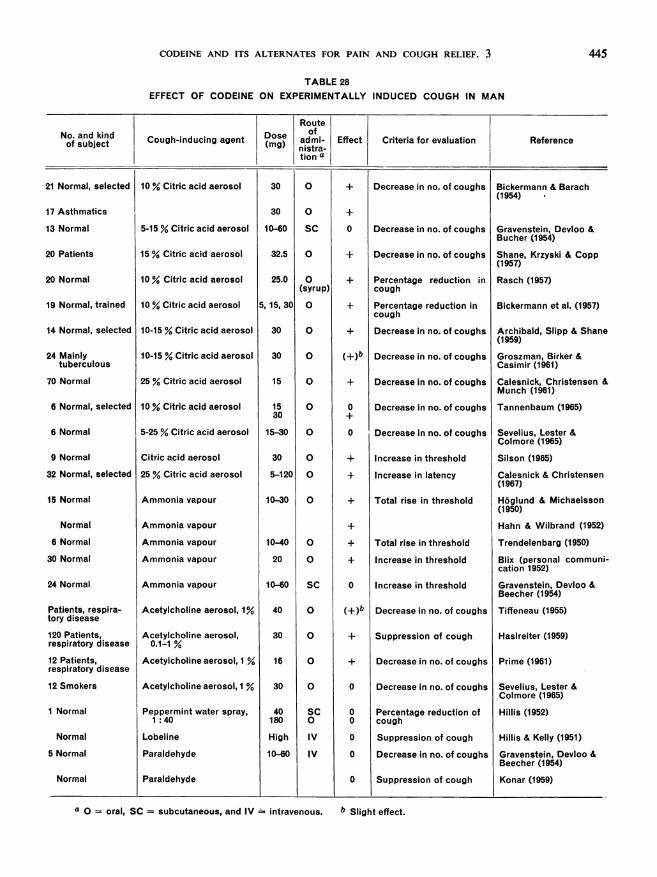
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
TABLE 28EFFECT OF CODEINE ON EXPERIMENTALLY INDUCED COUGH IN MAN
RouteNo. and kind Dose IofCough-inducing agent (m)Iadmi- Effect Criteria for evaluation Referenceof subject (mg nistra-
tion a
21 Normal, selected
17 Asthmatics
13 Normal
20 Patients
20 Normal
19 Normal, trained
14 Normal, selected
24 Mainlytuberculous
70 Normal
6 Normal, selected
6 Normal
9 Normal
32 Normal, selected
15 Normal
Normal
6 Normal
30 Normal
24 Normal
Patients, respira-tory disease
120 Patients,respiratory disease
12 Patients,respiratory disease
12 Smokers
1 Normal
Normal
5 Normal
Normal
10 % Citric acid aerosol
5-15 % Citric acid aerosol
15 % Citric acid aerosol
10 % Citric acid aerosol
10 % Citric acid aerosol
10-15 % Citric acid aerosol
10-15 % Citric acid aerosol
25 % Citric acid aerosol
10 % Citric acid aerosol
5-25 % Citric acid aerosol
Citric acid aerosol
25 % Citric acid aerosol
Ammonia vapour
Ammonia vapour
Ammonia vapour
Ammonia vapour
Ammonia vapour
Acetylcholine aerosol, 1%
Acetylcholine aerosol,0.1-1 %
Acetylcholine aerosol, I %
Acetylcholine aerosol, 1 %
Peppermint water spray,1 :40
Lobeline
Paraldehyde
Paraldehyde
30
30
10-60
32.5
25.0
5, 15, 30
30
30
15
1530
15-30
30
5-120
10-30
10-40
20
10-60
40
30
16
30
40180
High
10-60
0
0
SC
0
0(syrup)
0
0
0
0
0
0
0
0
0
0
0
SC
0
0
0
0
SC0
IV
IV
++
+b+
+
+
+
0
+
0
+
+
0
(+)b
+
+
0
00
0
Decrease in no. of coughs Bickermann & Barach(1954)
Decrease in no. of coughs
Decrease in no. of coughs
Percentage reduction incough
Percentage reduction incough
Decrease in no. of coughs
Decrease in no. of coughs
Decrease in no. of coughs
Decrease in no. of coughs
Decrease in no. of coughs
Increase in threshold
Increase in latency
Total rise in threshold
Total rise in threshold
Increase in threshold
Increase in threshold
Decrease in no. of coughs
Suppression of cough
Decrease in no. of coughs
Decrease in no. of coughs
Percentage reduction ofcough
Suppression of cough
Decrease in no. of coughs
Suppression of cough
Gravenstein, Devloo &Bucher (1954)
Shane, Krzyski & Copp(1957)
Rasch (1957)
Bickermann et al. (1957)
Archibald, Slipp & Shane(1959)Groszman, Birker &Casimir (1961)
Calesnick, Christensen &Munch (1961)
Tannenbaum (1965)
Sevelius, Lester &Colmore (1965)
Silson (1965)
Calesnick & Christensen(1967)
Hoglund & Michaelsson(1950)
Hahn & Wilbrand (1952)
Trendelenbarg (1950)
Blix (personal communi-cation 1952)
Gravenstein, Devloo &Beecher (1954)Tiffeneau (1955)
Hasireiter (1959)
Prime (1961)
Sevelius, Lester &Colmore (1965)Hillis (1952)
Hillis & Kelly (1951)
Gravenstein, Devloo &Beecher (1954)
Konar (1959)
a 0 = oral, SC = subcutaneous, and IV - intravenous.
445
b Slight effect.
N. B. EDDY AND OTHERS
method. Tannenbaum (1965) obtained results whichwere not significant for a 15-mg dose of codeine butwhich showed significant cough suppression with30 mg compared with a placebo. Groszman, Birker& Casimir (1961) found a moderate antitussive effectwith 30 mg of codeine, orally, which was greater inthose tuberculous patients who responded only mod-erately to a citric acid aerosol.
Silson (1965) made his subjects inhale a fixed con-centration of citric acid aerosol continuously until acough response occurred. From the time for this tooccur and the concentration of the aerosol, a citricacid threshold stimulus was calculated and effect wasexpressed as percentage increase of this threshold.An oral dose of 30 mg of codeine raised the thresholdin the nine subjects tested.
Calesnick & Christensen (1967) considered thelatency of response (time elapsing between beginningof inhalation of a constant citric acid concentrationand occurrence of cough response) to be a purelyobjective index useful for measuring antitussive po-tency. By this parameter a single oral dose of 5 mgof codeine exerted a measurable antitussive effect,differing with statistical significance from the res-ponse to a placebo. A dose-response curve wasplotted for doses of 5-120 mg with the maximumeffect at 40 mg of codeine. These authors also stud-ied the influence of the citric acid concentration inthe aerosol on the cough-suppressant effect of aconstant dose of40 mg of codeine. When the amountof citric acid provided supramaximal stimulation, agradual reduction in the antitussive effectiveness ofcodeine occurred until a cough-suppressing actioncould not be distinguished from the response toplacebo.
Gravenstein, Devloo & Beecher (1954) were unableto detect a cough-suppressing effect of oral dosesof 30 mg of codeine, whether citric acid aerosols,ammonia inhalations or intravenous paraldehydeinjections were used as stimuli, because of the greatvariability in the reactions of the subjects. Otherantitussives used for comparison also failed todemonstrate effectiveness, except for heroin afterparaldehyde injection.
Sevelius, Lester & Colmore (1965) said that theirsubjects became adapted to the citric acid aerosoland consequently an antitussive effect of 30 mg ofcodeine was not demonstrated. Using an acetyl-choline aerosol to induce cough, the effect of 30 mgof codeine was no greater than that of a placebo whe-ther the post-drug test was made at 60 or 120 minutes.Other authors have regarded the ammonia and
acetylcholine inhalation methods feasible for anti-tussive testing.Hoglund & Michaelsson (1950), who were the
first to develop a method for induction of cough, orits equivalent, experimentally in man, added amountsof ammonia to the inspired air with human volun-teers. The closure of the glottis and the momentarypause in respiration which followed was considereda substitute for a cough response and the antitussiveeffectiveness of codeine was calculated from theamount of codeine required to raise the threshold.A dose-response curve was established for 10, 15, 20and 30 mg of codeine. Trendelenburg (1950) used thesame method and criteria and found a good dose-response relationship for 10-40 mg of codeine, orally,as shown below.
Codeinedose(mg)
10203040
No.of trials
31553
Maximumthresholdelevation
(%)6211991137
Duration Total effectof elevation (o% x time)
(min)
607210080
2 310469547805 950
In nearly all cases the threshold returned to theinitial value within the 3-4 hour observation period.Hahn & Wilbrand (1952) and Blix (personal com-munication, 1952) also reported a depressing actionof codeine on ammonia-induced cough.
Tiffeneau (1955), who initiated the use ofan acetyl-choline aerosol for cough production, saw only avery moderate effect on the cough frequency by anoral dose of 40 mg of codeine. Haslreiter (1959)conducted a double-blind trial on 120 patients withrespiratory disease, who coughed in response to indi-vidually determined concentrations of acetylcholineaerosol. After 30 mg of codeine, orally, coughingbouts could not be induced with the same concentra-tion of acetylcholine in 58% of the patients; coughingbouts could not be induced in 6% of the patientsafter a placebo. Prime (1961) using a 1% acetyl-choline aerosol demonstrated a significant decreasein the number of coughs in 12 patients, 20 minutesafter an oral dose of 20 mg of codeine. Comparisonwas with a placebo in random order under double-blind conditions.Other attempts to demonstrate an antitussive effect
of codeine on cough induced by other procedureshave failed. Hillis (1952) used a peppermint: waterspray (1: 40). Codeine, 60 mg subcutaneously, or180 mg orally, did not reduce the number of coughsbut morphine did. Hillis & Kelly (1951) injectedlobeline intravenously. A substantial dose of mor-
446
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
phine or codeine did not block the resulting coughbut hexamethonium was effective. According toGravenstein, Devloo & Beecher (1954) and Konar(1959) the cough following intravenous injection ofparaldehyde could not be influenced by codeine.
Clinical trials and experience (Table 29)
The first report on a clinical trial of codeine as anantitussive which might meet today's standards wasby Davenport (1938). He compared, double-blind,oral doses four times a day of dihydroisocodeine andcodeine in tuberculous patients. Evaluation was bysubjective effect following medication and the twodrugs were judged equally effective. There was nocomparison with placebo. The antitussive effective-ness of codeine was accepted without question at thattime, though it had not been established for patholo-gical cough in man by placebo comparison. Him-melsbach et al. (1940) added placebo to a double-blind comparison of morphine and codeine asantitussives. The cough of the majority of thepatients worsened when codeine was replaced byplacebo and improved when the switch was to mor-phine. No change occurred when a 2-mg dose ofmorphine was replaced by 10 mg of codeine. Theseauthors believed 10 mg of codeine to be an optimaldose and 30 mg unnecessarily large.
Cass & Frederik (1953) compared 17 mg ofcodeine4 times a day with 4 mg of dextromethorphan anda placebo in 65 patients with chronic cough underdouble-blind conditions, and clearly established theantitussive effect of codeine. Their patients identifiedtwo of the three coded placebo medications correctlyas least effective and the three coded codeine prepa-rations as most effective. The authors transformedsubjective assessment of cough severity into an aver-age cough-intensity score for each treatment. Inanother trial Cass, Frederik & Andosca (1954)demonstrated the ability of their patients to discerncorrectly differences in the antitussive effectivenessof three different doses of dextromethorphan. Theplacebo medication was least effective and the cough-intensity score of 15 mg of codeine lay between thoseof 12 and 18 mg of dextromethorphan.Abelmann, Gaensler & Badger (1954) found
16.2 mg of codeine three times a day more effectivethan placebo, measured by days in which cough wasimproved. Haslreiter (1959) assessed the effect of30 mg of codeine three times a day against placeboin a double-blind trial on 60 patients during a testof pipazetate. Of the patients receiving codeine,
87% experienced relief while only 14% of those onplacebo registered improvement. Di Gregorio (1960)demonstrated a good antitussive effect of 30 mg ofcodeine, given three times a day, on acute as well ason chronic cough.
Gravenstein, Devloo & Beecher (1954) and Gra-venstein & Beecher (1955) devised an objective meth-od of cough counting by means of a sound recorderand compared the results of therapy obtained bysubjective assessment of coughing with the actualcough counts. While a difference of statistical sig-nificance in the patients' judgement of antitussiveeffectiveness of codeine and heroin against placebowas found, at least in one of the two groups ofpatients, the cough counts did not show a corre-sponding difference. From this the authors suggestedthat the activity of antitussives, especially of codeine,consisted essentially in a modification of psycho-logical factors so that patients felt better and thoughtthey coughed less when changes in the cough fre-quency did not occur.Proof to the contrary was obtained subsequently
by Cavalieri et al. (1960), Nicolis & Pasquariello(1962a, 1962b) and Pasquariello & Nicolis (1962).They counted the number of coughs for a three-hourperiod following the oral administration of 60 mg ofcodeine or placebo and demonstrated a significantdifference. The same patients were evaluated fortheir subjective response. They preferred codeine,15 patients to 5, but scores based on patients'judgement of cough intensity showed no markeddifference between codeine and placebo.Woolf& Rosenberg (1962) compared, in a double-
blind trial, codeine in syrup, 32.4 mg five times daily,with the syrup alone and found a definite antitussiveeffect of codeine by a preference-ranking scheme. Ina subsequent study (Woolf & Rosenberg 1964), inwhich cough was sound-recorded over a 24-hourperiod, the syrup with codeine, 32.4 mg five times aday, was significantly more effective compared witha control period and to a period of administrationof syrup alone. Thus they showed antitussive poten-cy for codeine by both subjective and objectivemethods of evaluation.
Sevelius & Colmore (1967) also found 15 mg ofcodeine, three times a day, more effective thanplacebo by subjective and objective methods. In12 male hospitalized patients with chronic cough,the coughing pattern was determined for two days.If the counts agreed within 20% the experiment wascontinued with alternative administration of drugand placebo. The reduction in the number of coughs
447
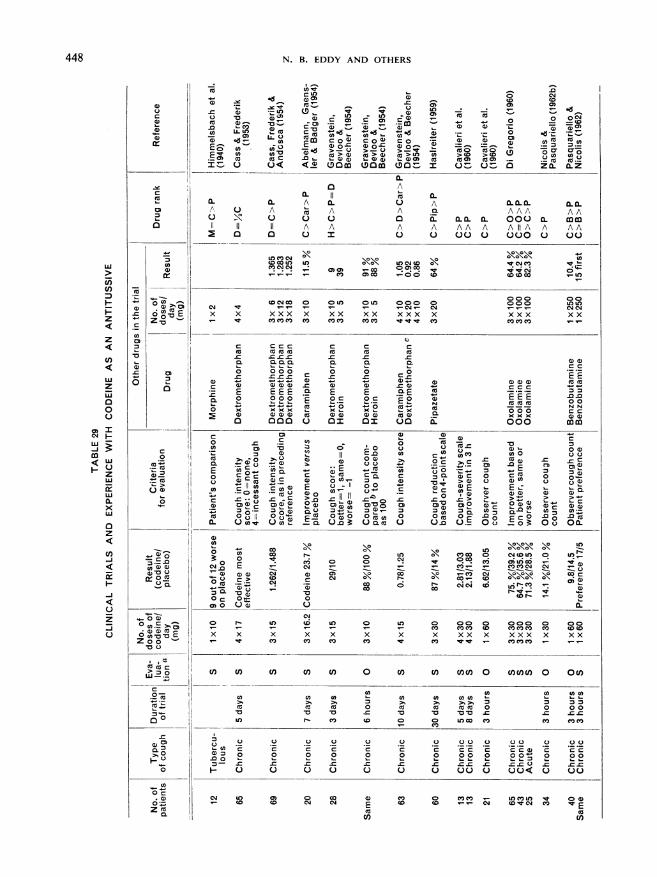
4) ._
U _r_ )
C: 11 'a
0) (c (
0 VdC-C
I
-c
(L
2 0) -~
m
:1
0
-4O cm6 0-a E
c
0
(U
(U
(U
0
a)n0
~0(U
0 (c. >,
z 0
Oc
x x
N. B. EDDY AND OTHERS
-LO0
C] A~~~~~~~~~~~~~~~C
(Uto U QQrAnLo (U 0AQO .c 0C) 0)Q U) 1L Q CO4c'0 ~~~~~~.. - ~~~~~~ 0 ~~~~~g,t
U. U c(U (~\co o c 0 *
>30c 0- (U- -0 \- - o
Ct C> >Q a) c) >LO _ >W>, Us a) CD c
(Uc n.. -((w ..(U(U C.(U0( (U (U0( (UO) *U (U .2
0<NO O. (OCO (OCO 000C I 0000 Z0 CL
0 ~~~A0. (U 0.
0. A 0.) A 0..00L.0.LA A A _ A A A AA0X0 0 0XI (L0X0 00 00.X cocIIte XA A A A AA A AIIA A AA
lo (0)01(0U UU L UU') CIO 004
.4 4 0))'n-00 0Ra R - ico O)(co -00 (0 co0o(o0(U'
( 04 co 0 0(00o0 000DO 0 000 LO to
xxx x xx xx xxx x xxx xxcoC3COCO CO co CO COCOco lt11, CO) COCOCO
C ccc c cs c(U (Uc( (U (U (U
o 000 0 0 0
s E EEE *EEE 2 *E E E0 X,.-(U (U(U(U (U (U(U (U(U (U*c x x x (Umo DOD 0 DIs D 000o. 000 mm
0 0
Q >° >(U 0° >
= (UAs Q (UmB
0 (U- oCQ .-
-Q aE)_ ~0@(C 0
~~~~~~o C a()
O > U) eDU:> O U:
CMc 00 0 c
0(
X cXo X X XC C
I-
0n clncn u o Cn-aco~~~~~~~~~~~a
> ~>~ >, nU U U U
L CLO
O c, c) c.c_ c. c
H0 0 0 0 0 0
N1 0 00CO cotD N E CD
cn
~~~ 0 ~~~0 Uco coO 0 0
cm (U CDs
cz 'C *.-E -4 E, <, ,cQc O.E Eg-
0c > > > >
s1. 0°° av) a) - : '
cmw (U IL- U (
_ cr). a O : C4. cn :3 U):
0 M O 0 E\ \0 00n
On 0. Oos Oo00.*0 00 0 0010 0 0fL
L-OOl
Xl tt co O CO CD LtO OLO
(0'ut - ( 0 0 o
X CO 0 0 0 00
CO 7OCOC CD COOC CO 0
C 4 C C CO cO
O) OCDO0 U)o 0 0
(UUC) O (U (U(
(U COUn 0 UE 0 00O0 u~~~co co co~~~ CDoCD
o o 0 0 0 0 00
2 cc. c2 .2E2 2 .22.c ca .c .)c ~ccO
00 0 00<l" 0 00
UU0 CIOCID m CY) LO ~~~~~~C,)(
448
(U._..
0)
a
-a
CD
w
FnU,)
H
z
z
U)
wzw00U
0) 1
CO4
w
E
<w0
z
-
-LJ
0.Z0
ca
ll,i
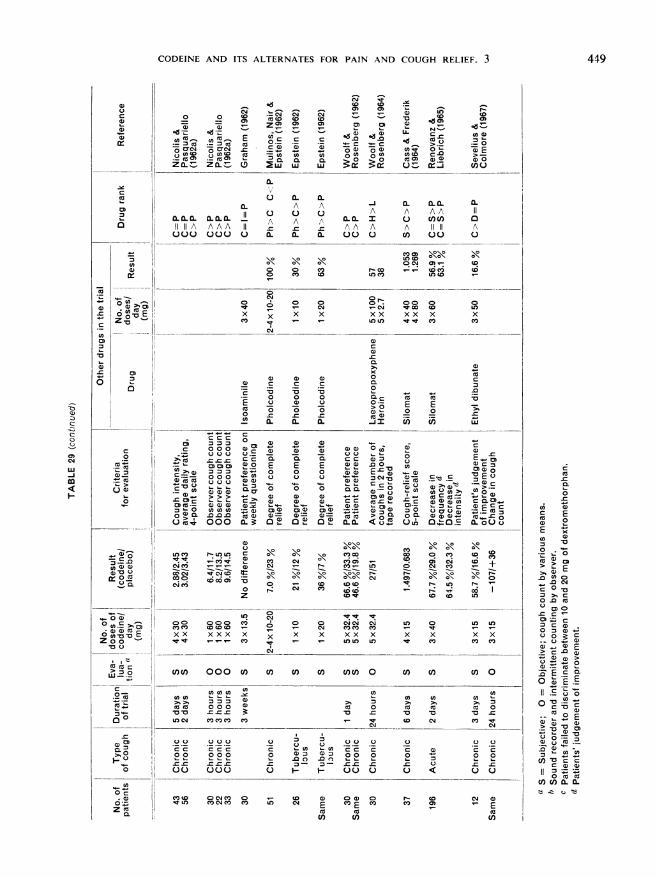
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
-Q U)Q Z0, 0 0 0) cm°
L~~~~~~~~~~~~~~LO a)O ' 7cO C O 5 U) D wz Z .2in n -w w - U)0
a. a.a a
a. 0A 0 A A A Aa. a ca. A A A 0.0a. I 0 co()0IIIA AAA 11 A A fA A A liii A0000000) a. 0. a. 000) c/) 00 0
0
0
C')
0x
M ');
0 C
0 0
x x
co cb \\IXuf) CD00C4 0! -:
o r-oCD 00 0_Cli cOD cox x x x xXL IV
X
CDco
0
xC.
. a~~~~~~~~~~~~~~~~~~~~~)C
c ~~~~~CL
0 CU~~~~~~~~~~~U O 0 C° Ouq~~~~~U C
2co0S E t)4~0) °* E -
I ~ ~~~~~~O o o a) 0)°-c -c
Ia. a. ..Xi u3 cw
C 000 a) 0U)c-a) ) CD cD
°° OC c L
E E E 0U
0 0iE0 0 a Du - _ E
nC oU 000c, DUa)OOa, *_*_ a}0° U*-co W0U M(Dn) aU) D D
ME C 0c a)00) CB CD,
000 a.~3- -o a~ -a~.c a. ou0
CO _ a
C9^ --:!-zzc0CQ t C-cOcoC') CO04m~~
D 0oCO _xx xxx x
c/)C) 000 C/
cncn
U U)OOcu c
o o oo o
Vt C
csc cs c
co o) COCl
ItLO) COC) C4c co
C')
04
0
x
C')
C CRfC.f- '- LO
soso
o CDCDC) CXO C(
0~ 0 04~01C.Cl' COC CO-
x x x x x
COCO LO
\1 \1CO3CD 0 CO
0- C) CO
C)
t 1- LO
r-D
I
(e ctoCD +
r -
ooUl)
LO In UC
x x x x
"W
cn un cn un un O cn cn u oO
CU 0 CU 0
C VS_ D C') CO t
C_ ~ C_ C_ .C
0 I- - 000 0 S 0 0
U)co) N UDLO c4 E <tE<taE
CU CU CUcn) C)
C
E0
-ECl) U°
> E
0 2a
E x
0 c
.0CD0
.0 C'o
u 0
W >) CQ. CU
0 0
0*.C C
U).~ ° E.? C a. a
tQ _c- a) lr
c CO ' ~ E
II ._
o n : H
Ua) Q CU,
(I) V C C
(1 Cl) 0. 0
0
U)
U)
U)
449
cu
0
L-
0
00
U0 _
Z cm
076(D
s:~r-
2,tq)
c-JQa
m)
750Ca
-c
0 CD
° t 1
CD):C.) -
Zo
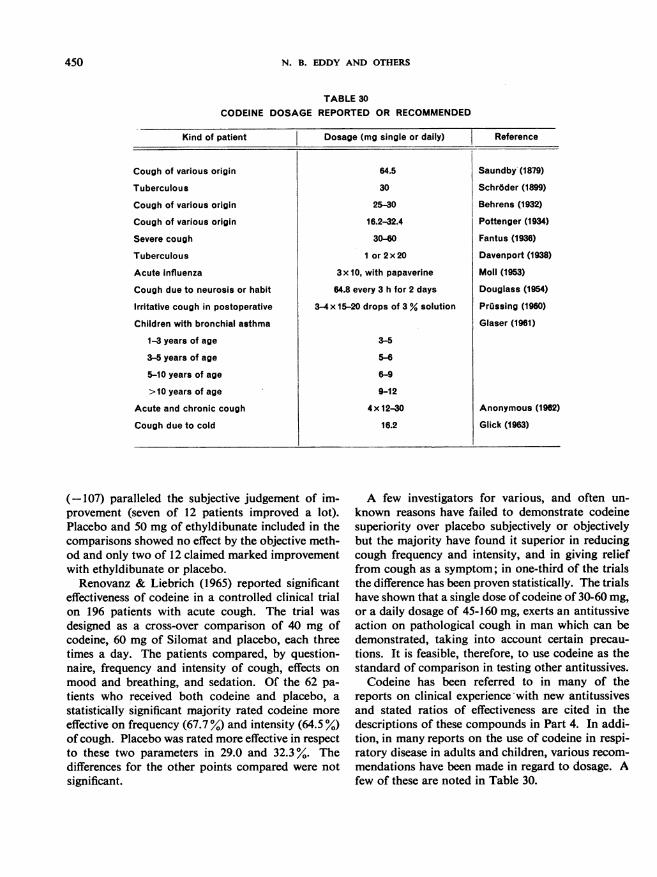
N. B. EDDY AND OTHERS
TABLE 30CODEINE DOSAGE REPORTED OR RECOMMENDED
Kind of patient
Cough of various origin
Tuberculous
Cough of various origin
Cough of various origin
Severe cough
Tuberculous
Acute influenza
Cough due to neurosis or habit
Irritative cough in postoperative
Children with bronchial asthma
1-3 years of age
3-5 years of age
5-10 years of age
>10 years of age
Acute and chronic cough
Cough due to cold
Dosage (mg single or daily)
64.5
30
25-30
16.2-32.4
30-GOI or2x20
3x 10, with papaverine
64.8 every 3 h for 2 days
3-4x 15-20 drops of 3 % solution
3-5
5-6
6-9
9-12
4 x 12-30
16.2
Reference
Saundby (1879)
Schr6der (1899)
Behrens (1932)
Pottenger (1934)
Fantus (1936)
Davenport (1938)
Moll (1953)
Douglass (1954)
Prussing (1960)
Glaser (1961)
Anonymous (1962)
Glick (1963)
(-107) paralleled the subjective judgement of im-provement (seven of 12 patients improved a lot).Placebo and 50 mg of ethyldibunate included in thecomparisons showed no effect by the objective meth-od and only two of 12 claimed marked improvementwith ethyldibunate or placebo.Renovanz & Liebrich (1965) reported significant
effectiveness of codeine in a controlled clinical trialon 196 patients with acute cough. The trial wasdesigned as a cross-over comparison of 40 mg ofcodeine, 60 mg of Silomat and placebo, each threetimes a day. The patients compared, by question-naire, frequency and intensity of cough, effects onmood and breathing, and sedation. Of the 62 pa-tients who received both codeine and placebo, astatistically significant majority rated codeine moreeffective on frequency (67.7 %) and intensity (64.5 %)of cough. Placebo was rated more effective in respectto these two parameters in 29.0 and 32.3%. Thedifferences for the other points compared were notsignificant.
A few investigators for various, and often un-known reasons have failed to demonstrate codeinesuperiority over placebo subjectively or objectivelybut the majority have found it superior in reducingcough frequency and intensity, and in giving relieffrom cough as a symptom; in one-third of the trialsthe difference has been proven statistically. The trialshave shown that a single dose of codeine of 30-60 mg,or a daily dosage of 45-160 mg, exerts an antitussiveaction on pathological cough in man which can bedemonstrated, taking into account certain precau-tions. It is feasible, therefore, to use codeine as thestandard of comparison in testing other antitussives.Codeine has been referred to in many of the
reports on clinical experience with new antitussivesand stated ratios of effectiveness are cited in thedescriptions of these compounds in Part 4. In addi-tion, in many reports on the use of codeine in respi-ratory disease in adults and children, various recom-mendations have been made in regard to dosage. Afew of these are noted in Table 30.
450
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3
RESUME
LA CODEINE ET SES SUCCEDANES SEDATIFS DE LA DOULEUR ET DE LA TOUX:3. LA SEDATION DE LA TOUX PAR LA CODIINE - MECANISME METHODOLOGIE ET
EVALUATION
Cette troisieme partie du rapport d'ensemble consacreaux propriet6s sedatives de la codeine et de ses succedanesexpose en detail les donnees experimentales relatives auxvoies qu'emprunte le r6flexe de la toux et au mecanismede ce moyen de protection contre les irritations nociveset les lesions des voies aeriennes par des agents m6ca-niques ou chimiques. Les etudes les plus r6centes de sanature et de son fonctionnement supportent l'hypotheseselon laquelle le reflexe est en grande partie ind6pendantdu mecanisme de la respiration. La toux est un symptomeque l'on observe dans un tres grand nombre de maladies(inflammatoires, infectieuses, allergiques, circulatoires,psychiques).On a mis au point toute une serie de methodes en vue
d'evaluer chez l'animal les effets s6datifs sur la toux dela codeine ou d'autres drogues. On peut recourir pourprovoquer la toux a des stimuli chimiques, mecaniquesou 6lectriques. Ces divers procedes font l'objet d'unedescription minutieuse et leurs avantages et desavantagesrespectifs sont examines.Pour juger de la valeur therapeutique d'une drogue, il
est particulierement utile d'apprecier son action sedativesur la toux directement chez l'homme. A cet effet, latoux peut etre provoqu6e experimentalement au moyend'inhalations d'aerosols contenant de l'acetylcholine, del'ammoniac ou de l'acide citrique ou par l'injection delobeline ou de parald6hyde. Ces methodes ont rendupossibles de nombreuses experiences qui sont relatees endetail. Bien que la toux artificiellement induite chez unsujet sain differe par maints caracteres de la toux d'originepathologique, les etudes de ce genre permettent cependantde definir les analogies entre les resultats obtenus chezl'animal et les donnees recueillies chez l'homme. IIimporte dans tous les cas de leur adjoindre des recherchesconcernant l'absorption, la distribution dans l'organismeet le metabolisme des drogues exp6riment6es afin dereunir davantage d'informations sur les similitudes entreles especes. Ces donnees fourniront la base de l'inter-pretation des resultats de laboratoire et des applicationscliniques.
L'evaluation des propriet6s sedatives des drogues chezdes malades presentant une toux de nature pathologiquedue a l'une ou l'autre cause doit etre men6e en se confor-mant aux exigences fondamentales de la pharmacologieclinique. Diverses methodes utilisees 'a cet effet sontdecrites et discutees.Le cas d'un certain nombre de substances sedatives de
la toux est examin6 sous l'angle de leur lieu d'action dansl'organisme: des produits douds de proprietes analge-siques locales, comme la cocaine, la t6tracalne, la lido-
caine, 1'ethoforme, le benzonatate, le caramiphene, leclof6danol, la diphenhydramine, l'isoamimile, l'oxola-mine et la pholcodine sont capables d'agir sur les recep-teurs peripheriques reflexogenes. Bien que le site sp6ci-fique d'action des drogues sedatives de la toux soitprobablement le ((centre de la toux *, situe dans la moelle,on note entre les composes qui agissent a ce niveau(aminoindane, codeine, dextromethorphane, hexobarbi-tal, pipaz6tate) des variations portant sur la sp.cificitM del'effet, les modalites de la reponse et l'ampleur desreactions accessoires.
Les substances qui apaisent la toux ont parfois d'autreseffets pharmacodynamiques qui accroissent ou, aucontraire, diminuent l'efficacite de leur action sp6cifiquesur le reflexe. On examine a cet egard la fagon dontl'aminoindane, le benzonatate, l'hexobarbital, la pen-toxyverine, la pholcodine et le pipazetate agissent sur larespiration. Les analg6siques - du moins ceux dontl'action s'apparente a celle de la morphine - attenuentla toux, mais des composes comme le dextrom6thor-phane, la noscapine et la pholcodine, qui ont un effetsedatif sur la toux, ne sont pas necessairement dou6s deproprietes analgesiques. Pour mieux comprendre les rela-tions entre l'att6nuation de la douleur et la sedation dela toux, il faudra, par une 6tude experimentale plus pous-see, rechercher dans quelle mesure les sedatifs gen6raux(hypnotiques) sont capables de combattre la toux. Lesneuroleptiques comme la chlorpromazine, la perph6na-zine et la prochlorp6razine modifient le m6canisme dureflexe de toux. On a montr6 que l'inhalation d'hexa-methonium supprime la toux provoqu6e experimentale-ment chez l'homme par l'inhalation d'ac6tylcholine,mais des tests utilisant des sels quaternaires de substancessedatives de la toux n'ont pas permis d'apporter lapreuve definitive du r6le du blocage ganglionnaire dansla suppression du r6flexe. L'examen des donn6es experi-mentales concernant un certain nombre de substancesdouees de propri6tes spasmolytiques ou spasmogenes nefait ressortir aucune relation precise entre ces effetssp6cifiques et l'action sedative sur la toux. Du point devue clinique, 1'efficacite des substances actives contre latoux ne parait pas alt6ree lorsque leur emploi a pour re-sultat d'accroitre ou de diminuer la s6cretion bronchique.
L'action de la codeine sur la toux provoqu6e, tant chez1'homme que chez l'animal, a fourni matiere a de tresnombreuses recherches. La plupart des exp6rimentateursassignent a la codeine une efficacit6 plus ou moinsgrande, et rares sont ceux qui n'ont pas constate unesedation de la toux apres administration de la substance.Pour la majorite des chercheurs qui ont procd6 is des
451
452 N. B. EDDY AND OTHERS
essais cliniques, les effets calmants de la codeine, sur lafrequence comme sur l'intensite de la toux, sont supe-rieurs a ceux des placebos; dans un tiers des cas, ladifference d'action est statistiquement significative. Cesmemes essais ont montr6 que la codeine, administree a
raison de 30 a 60 mg en dose unique ou de 45 a 160 mgquotidiennement, combat efficacement la toux patholo-gique chez l'homme. II est des lors possible de l'utilisercomme substance de reference pour les essais d'evaluationd'autres composes sedatifs de la toux.
REFERENCES
Abelmann, W. H., Gaensler, E. A. & Badger, T. L. (1954)Dis. Chest, 25, 532
Abruzzi, W. A. (1962) J. New Drugs, 2, 310Amdur, M. 0. (1957) Amer. industr. Hyg. Ass. Quart.,
18, 149Amler, A. B. & Rothman, C. B. (1963) J. New Drugs, 3,
362Anonymous (1962) Practitioner, 188, 249Archibald, D. W., Slipp, L. B. & Shane, S. J. (1959)
Canad. med. Ass. J., 80, 734Balea, T. & Buret, J. (1964) ThJrapie, 19, 631Banyai, A. L. & Johannides, M., Jr (1956) Dis. Chest,
29, 52Bedell, G. N. & Seebohm, P. M. (1959) J. Amer. med.
Ass., 169, 1699Beecher, H. K. (1955) J. Amer. med. Ass., 159, 1602Behrens, H. 0. (1932) Ther. d. Gegenw., 73, 399Bein, H. J. & Bucher, K. (1957) Helv. physiol. pharmacol.
Acta, 15, 55Benson, W. M., Stefko, P. L. & Randall, L. 0. (1953)
J. Pharmacol. exp. Ther., 109, 189Bickerman, H. A. (1960a) In: Modell, W., ed., Drugsof choice, St. Louis, USA, Mosby Co., p. 493
Bickerman, H. A. (1960b) In: Gordon, B. L., ed., Clinicalcardiopulmonary physiology, New York, Grune and
Stratton, p. 495Bickerman, H. A. & Barach, A. L. (1954) Amer. J. med.
Sci., 228, 156Bickerman, H. A. & Itkin, S. E. (1960) Clin. Pharmacol.
Ther., 1, 180Bickerman, H. A., et al. (1956) Amer. J. med. Sci., 232,
57Bickerman, H. A., et al. (1957) Amer. J. med. Sci., 234,
191Bidwell, S. M. R. & Boyd, E. M. (1952) J. Pharmacol.
exp. Ther., 104, 224Bobb, J. R. & Ellis, S. (1951) J. Physiol., 167, 768Boissier, J.-R. & Pagny, J. (1960a) Therapie, 15, 93Boissier, J.-R. & Pagny, J. (1960b) Therapie, 15, 97Borison, H. L. (1948) Amer. J. Physiol., 154, 55Boyd, E. M. (1954) Pharmacol. Rev., 6, 521Boyd, E. M. & Boyd, C. E. (1960) Canad. med. Ass. J.,
83, 1298Bucher, K. (1958) Pharmacol. Rev., 10, 43Bucher, K. & Jacot, C. (1951) Helv. physiol. pharmacol.
Acta, 9, 454
Cahen, R. & Boucherle, A. (1961) C. R. Soc. Biol. (Paris),155, 1034
Cahen, R. & Boucherle, A. (1964) C. R. Soc. Biol. (Paris),158, 1021
Cahen, R. & Boucherle, A. (1965) Fed. Proc., 24, 549Calesnick, B. & Christensen, J. A. (1967) Clin. Pharmacol.
Ther., 8, 374Calesnick, B., Christensen, J. A. & Munch, J. C. (1961)Amer. J. med. Sci., 242, 560
Capello, G. & DiPasquale, S. (1955) Schweiz. Z. Tuberk.,12, 80
Carter, C. H. & Maley, M. C. (1957) Amer. J. med. Sci.,233, 77
Cass, L. J. & Frederik, W. S. (1953) New Engl. J. Med.,249, 139
Cass. L. J. & Frederik, W. S. (1956) J. Lab. clin. Med.,48, 879
Cass, L. J. & Frederik, W. S. (1958) Ann. intern. Med., 49,151
Cass, L. J. & Frederik, W. S. (1964) Curr. ther. Res., 6, 14Cass, L. J., Frederik, W. S. & Andosca, J. B. (1954) Amer.
J. med. Sci., 227, 291Cavalieri, U., et al. (1960) J. Geront., 8, 981Chabrier, B., Giudicelli, R. & Thuillier, J. (1950) Ann.pharm. franc., 8, 261
Chakravarty, N. K., et al. (1956) J. Pharmacol. exp. Ther.,117, 127
Chen, J. Y. P., Biller, H. F. & Montgomery, E. G. (1960)J. Pharmacol. exp. Ther., 128, 384
Dalhamn, T. (1960) Acta physiol. scand., 49, 242Davenport, L. F. (1938) J. Pharmacol. exp. Ther., 64, 236David, A., Leith-Ross, F. & Vallance, D. K. (1957)
J. Pharm. Pharmacol., 9, 446DeVleeschhauwer (1954) Arch. int. Pharmacodyn., 97, 34DiGregorio, M. (1960) Minerva med., 51, 4086Domenjoz, R. (1952) Arch. exp. Path. Pharmak., 215, 19Douglass, B. E. (1954) Med. Clin. N. Amer., 38, 949Eichler, 0. & Smiatek, A. (1940) Arch. exp. Path.Pharmak., 194, 621
Engelhorn, R. (1960) Arzneimittel-Forsch., 10, 785Engelhorn, R. & Weller, E. (1961) Pflugers Arch. ges.
Physiol., 273, 614Engelhorn, R. & Weller, E. (1965) Pfluigers Arch. ges.
Physiol., 284, 224Ernst, A. M. (1938) Arch. int. Pharmacodyn., 58, 363Ernst, A. M. (1939) Arch. int. Pharmacodyn., 61, 73
CODEINE AND ITS ALTERNATES FOR PAIN AND COUGH RELIEF. 3 453
Fantus, B. (1936) J. Amer. med. Ass., 106, 375Floersheim, G. L. (1959) Helv. physiol. pharmacol. Acta,
17, 153Frey, R., Hugin, W. & Mayrhofer, 0. (1955) Lehrbuch
der Anaesthesiologie, Bcrlin, Springer-VerlagFriebel, H. (1960) Klin. Wschr., 38, 621Friebel, H. (1963) In: Muller, W. A., ed., Klinische Physio-
logie, Stuttgart, Thieme, vol. 1, p. 301Friebel, H. & Hahn, K.-J. (1966) Med. pharmacol. exp.
(Basel), 14, 78Friebel, H. & Kuhn, H.-F. (1962) Arch. exp. Path.
Pharmak., 243, 162Friebel, H. & Kuhn, H.-F. (1964) Arch. exp. Path.
Pharmak., 246, 527Friebel, H., Reichle, C. & von Graevenitz (1955) Arch.
exp. Path. Pharmak., 224, 384Furakawa, F. & Okabe, M. (1958) Ig. Kenkyyu, 28, 1643Glaser, J. (1961) Practitioner, 12, 715Glick, J. (1963) Delaware med. J., 35, 180Gordonoff, T. (1938) Ergebn. Physiol., 40, 53Gosswald, R. (1958) Arzneimittel-Forsch., 8, 550Graham, J. D. P. (1962) J. New Drugs, 2, 43Granier-Doyeux, M. et al. (1959) Arch. int. Pharmacodyn.
121, 287Gravenstein, J. S. & Beecher, H. K. (1955) Arzneitmittel-
Forsch., 5, 364Gravenstein, J. S., Devloo, R. A. & Beecher, H. K. (1954)
J. appl. Physiol., 7, 119Green, A. F. & Ward, N. B. (1955) Brit. J. Pharmacol.,
10, 418Groszman, M., Birker, I. 0. & Casimir, F. (1961) App!.
Ther., 3, 95Haas, H. (1955) Arch. exp. Path. Pharmak., 225, 442Hahn, K.-J. & Friebel, H. (1966) Med. Pharmacol. exp.
(Basel), 14, 87Hahn, L. A. & Wilbrand, H. (1952) Arch. int. Pharmaco-
dyn., 91, 144Hara, S. & Yanaura, S. (1959) Jap. J. Pharmacol., 9, 46Haslreiter, E. (1959) Arzneimittel-Forsch., 9, 769Hengen, 0. and Kasparek, H. (1958) Arzneimittel-Forsch.,
8, 620Herzog, H. (1967) Therapiewoche, 17, 532Hillis, B. R. (1952) Lancet, 1, 1230Hillis, B. R. & Kelly, J. C. C. (1951) Glasgow med. J., 32,
72Himmelsbach, C. K., et al. (1940) Publ. Hlth Rep. (Wash.)
Suppl. 158Hoglund, N. J. & Michaelsson, M. (1950) Acta physiol.
scand., 21, 168Isbell, H. & Fraser, H. F. (1953) J. Pharmacol. exp. Ther.,
107, 524Kallquist, I. & Melander, B. (1957) Arzneimittel-Forsch.,
7, 301Kase, Y. (1952) Jap. J. Pharmacol., 2, 7Kase, Y. (1954) Chem. pharm. Bull., 2, 298Kase, Y. (1955) Jap. J. Pharmacol., 4, 130Kase, Y. & Yuizono, T. (1959) Chem. pharm. Bull.,
7, 378
Kase, Y., et al. (1959) Chem. pharm. Bull., 7, 372Kelentey, B., et al. (1957) Arzneimittel-Forsch., 7, 594Kelentey, B., et al. (1958) Arzneimittel-Forsch., 8, 325Kleibel, F. (1964) Med. Welt (Stuttg.) 24, 1317Kleibel, F., Steinhoff, E. & Wilde, W. (1965) Therapie-
woche, 15, 1115Klein, B. (1958) Antibiot. Med., 5, 462Kohli, R. P., et al. (1960) Ind. J. med. Res., 48, 193Konar, N. R. & Dasgupta, S. (1959) J. Ind. med. Ass.,
32, 189Konzett, H. (1955) Wien. klin. Wschr., 67, 306Konzett, H. & Rothlin, E. (1954) Experientia, 10, 472Korpas, J., Tomori, Z. & Ivanca, 1. (1957) Physiol.
bohemoslov., 6, 111Krause, D. (1958) Arzneimittel-Forsch., 8, 553Kraushaar, A. E., Schunk, R. W. & Thym, H. F. (1964)
Arzneimittel-Forsch., 14, 986Kroepfli, P. (1950) Helv. physiol. pharmacol. Acta, 8, 33Krueger, H. M., Eddy, N. B. & Sumwalt, M. (1943) Publ.
Hlth Rep. (Wash.), Suppl. 165Krug, F. (1964) Med. Welt (Stuttg.), 18, 1026Kuhn, H.-F. & Friebel, H. (1960a) Arch. exp. Path.Pharmak., 240, 18
Kuhn, H.-F. & Friebel, H. (1960b) Med. exp. (Basel), 3,329
LaBarre, J. & Plisnier, H. (1959) Arch. int. Pharmacodyn.,119, 205
Larsell, 0. & Burget, G. E. (1924) Amer. J. Physiol., 70,311
Levis, S., Preat, S. & Moyersoons, F. (1955) Arch. int.Pharmacodyn., 103, 200
Lorenz, D. (1962) Arzneimittel-Forsch., 12, 1183Martin (1834) Arch. gen. Mid., 4, 2s, 692Martini, H. (1957) In: Nuckel, H. Aerosol-Therapie, Stutt-
gart, Schattauer, p. 120Matallana, A. & Borison, H. L. (1955) Fed. Proc., 14, 367Maurer, H. (1955) Deutsch. med. Wschr., 80, 351May, A. J. &Widdicombe, J. G.(1954)Brit. J. Pharmacol.,
9, 335Moll, E. L. (1953) Practitioner, 170, 76Morris, D. J. & Shane, S. J. (1960) Canad. med. Ass. J.,
83, 1093Mulinos, M. G. (1960) Toxicol. appl. Pharmacol., 2, 635Mulinos, M. G., Nair, K. G. & Epstein, J. G. (1962) N. Y.Med. J., 62, 2373
Nicolis, F. B. & Pasquariello, G. (1962a) Clin. ter.,23, 215
Nicolis, F. B. & Pasquariello, G. (1962b) J. Pharmacol.exp. Ther., 136, 183
Ozawa, H., et al. (1962) J. pharmacol. Soc. Jap., 82, 1314Parish, F. A. (1959) Med. Tms (N.Y.), 87, 1488Pasquariello, G. & Nicolis, F. B. (1962) Clin. ter., 23, 226Pellmont, B. & Bachtold, H. (1954) Schweiz. med. Wschr.,
84, 1368Perry, W. P. & Boyd, E. M. (1941) J. Pharmacol. exp.
Ther., 73, 65Phillips, A. M., Phillips, R. W. & Thompson, J. L. (1956)
Ann. intern. Med., 45, 216
454 N. B. EDDY AND OTHERS
Plisnier, H. (1957) Etude comparative de l'action des deri-ves de l'opium et de diverses substances synthetiques aeffet non morphinique sur le mecanisme de la toux, sur lebronchospasme et sur la secretion bronchique, Thesis,Brussels
Plisnier, H. (1958) C. R. Soc. Biol. (Paris), 152, 1267Plisnier, H. (1960) C. R. Soc. Biol. (Paris), 154, 451Plisnier, H. & Hernalsteen, L. (1953) C. R. Soc. Biol.
(Paris), 153, 363Pottenger, F. M. (1934) Clinical Tuberculosis, 2nd ed., St.
Louis, Mosby Co., p. 485Prime, F. J. (1961) Brit. med. J., 1, 1149Priissing, G. (1960) Deutsch. med. J., 11, 95Rasch, M. (1957) Nord. Med., 57, 629Reichle, C. & Friebel, H. (1955) Arch. exp. Path. Pharmak.,
226, 558Renovanz, H. D. & Liebrich, K. G. (1965) Arzneimittel-
Forsch., 15, 1393Rosiere, C. E. & Winder, C. V. (1955) J. Pharmacol. exp.
Ther., 113, 46Rosiere, C. E., Winder, C. V. & Wax, J. (1956) J. Pharma-
col. exp. Ther., 116, 296Ross, B. B., Gramia, R. & Rahn, H. (1955) J. appl.
Physiol., 8, 264Salem, H. & Aviado, D. M. (1964) Amer. J. med. Sci.,
247, 585Salle, J. & Brunaud, M. (1960) Arch. int. Pharmacodyn.,
126, 120Saundby, R. (1879) Brit. med. J., 1, 545Schlez, K. (1965) Ober die Verwendung des Vagusschlingen-
hundes far die Wertbestimmung hustenstillender Sub-stanzen, Thesis, Heidelberg
Schofield, P. B. (1963) Brit. J. Clin. Pract., 17, 583Schroder, G. (1899) Ther. d. Gegenew., 1, 113Schroeder, W. (1951) Arch. exp. Path. Pharmak., 212,433Sell, R., Lindner, E. & Jahn, H. (1958) Arch. exp. Path.
Pharmak., 234, 164Sevelius, H. D. and Colmore, J. P. (1967) Clin. Pharmacol.
Ther., 8, 381Sevelius, H., Lester, P. D. & Colmore, J. P. (1965) Clin.
Pharmacol. Ther., 6, 146Shane, S. J., Krzyski, T. K. & Copp, S. E. (1957) Canad.
med. Ass. J., 77, 600Silson, J. S. (1965) J. New Drugs, 5, 94Silvestrini, B. & Maffli, G. (1959) Farmaco, Ed. Sci., 14,440
Silvestrini, B.& Pozzatti, C. (1960) Arch. int. Pharmacodyn.,129, 249
Silvestrini, B. & Pozzatti, C. (1961) Brit. J. Pharmacol.,16, 209
Snell, E. S. & Armitage, P. (1957) Lancet, 1, 860Sollmann, T. (1957) Manual of pharmacology, 8th ed.,
Philadelphia, SaundersStaehelin, R. (1914) Jahreskurse drztl. Fortbild, 5, 32Stefko, P. L. and Benson, W. M. (1953) J. Pharmacol.
exp. Ther., 108. 217Stefko, P. L., Denzel, J. & Hickey, I. (1961) J. pharm.
Sci., 50, 216Suter, C. M. (1951) Medical chemistry, New York, J. Wiley& Sons, p. 405
Tannenbaum, F. J. (1965) Pharmacologist, 7, 77Tedeschi, R. E. et al. (1959) J. Pharmacol. exp. Ther., 126,
338Ther, L. & Lindner, E. (1958) In: Medizin und Chemie,
Berlin, I. G. Farbenindustrie, vol. 6, p. 351Tiffeneau, R. (1955) Z. Aerosol-Forsch., 4, 116Tiffeneau, R. (1957) Dis. Chest., 31, 404Tomori, Z. et al. (1960) Anesthetist, 9, 169Toner, J. J. & Macko, E. (1952) J. Pharmacol. exp. Ther.,
106, 246Trendelenburg, U. (1950) Acta physiol. scand., 21, 174Van Dongen, K. (1956) Acta physiol. pharmacol. neerl.,
4, 500Watt, J. (1959) Pharm. Industrie, 21, 386Weidemeyer, J. C., Kremer, H. W. & DeJongh, D. K.
(1960) Acta physiol. pharmacol. neerl., 9, 501Widdicombe, J. G. (1954a) J. Physiol., 123, 55Widdicombe, J. G. (1954b) J. Physiol., 123, 71Widdicombe, J. G. (1961) Arch. exp. Path. Pharmak., 241,
415Widdicombe, J. G. (1964) In: Fenn, W. 0. & Rahn, H.,
ed., Handbook of Physiology, Baltimore, Williams &Wilkins, vol. 1, sect. 3, Respiration, p. 585
Winder, C. V. & Rosiere, C. E. (1955) J. Pharmacol. exp.Ther., 113, 55
Winder, C. V., et al. (1961) J. Pharmacol. exp. Ther., 133,117
Winter, C. A. & Flataker, L. (1952) Proc. Soc. exp. Biol.(N.Y.), 81, 463
Winter, C. A. & Flataker, L. (1954) J. Pharmacol. exp.Ther., 112, 99
Woolf, C. R. & Rosenberg, A. (1962) Canad. med. Ass. J.,86, 810
Woolf, C. R. & Rosenberg, A. (1964) Thorax, 19, 125












![Selection of showering events and background suppression in … Ibnsalih... · 1.1.2 Mechanism of acceleration As mentioned previously, Enrico Fermi [4] rstly suggested the CRs mechanism](https://static.fdocuments.fr/doc/165x107/607b0e8880d79137e703d237/selection-of-showering-events-and-background-suppression-in-ibnsalih-112.jpg)





