- Indications, Techniques, Résultats-orthodoc.aaos.org/DrDidierFontes/EPAULE-Protheses.pdf · -...
77
Arthroplasties de l’Epaule - Indications, Techniques, Résultats- Didier FONTÈS Institut Main, Epaule et Sport Paris Espace Médical Vauban - Paris VII e
Transcript of - Indications, Techniques, Résultats-orthodoc.aaos.org/DrDidierFontes/EPAULE-Protheses.pdf · -...
Arthroplasties de l’Epaule
- Indications, Techniques, Résultats- Didier FONTÈS
Institut Main, Epaule et Sport Paris Espace Médical Vauban - Paris VIIe
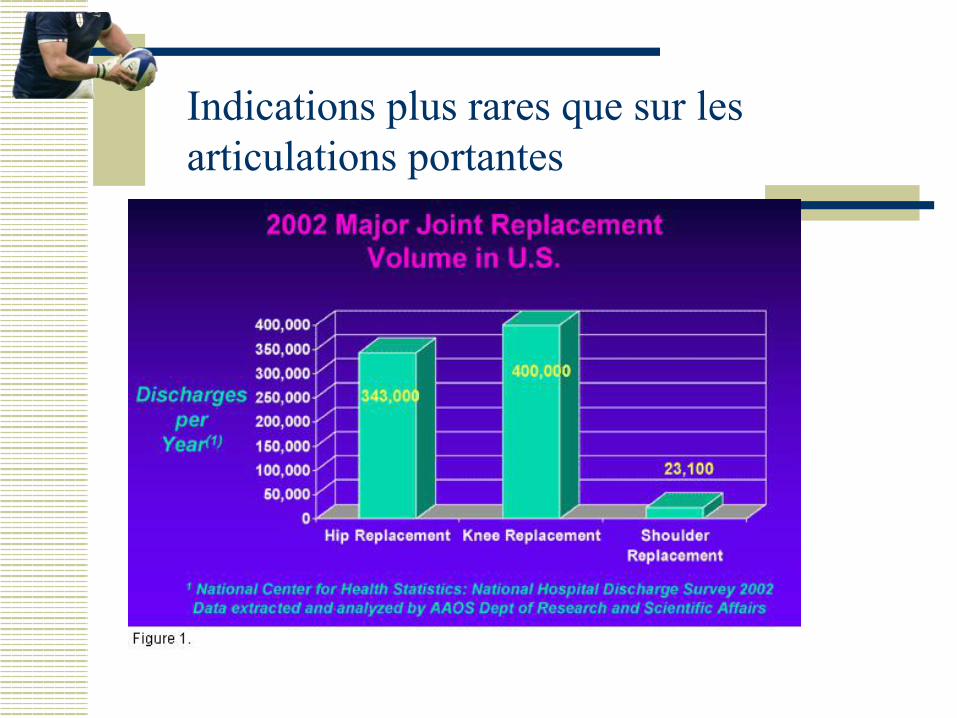
Indications plus rares que sur les articulations portantes
Anatomie de l’Epaule
w Grand secteur de Mobilité w Pas d’emboîtement articulaire w Stabilité tributaire des parties
molles sujettes à (micro)-traumatismes fréquents (coiffe, labrum)
w Dysproportion entre glène et tête humérale
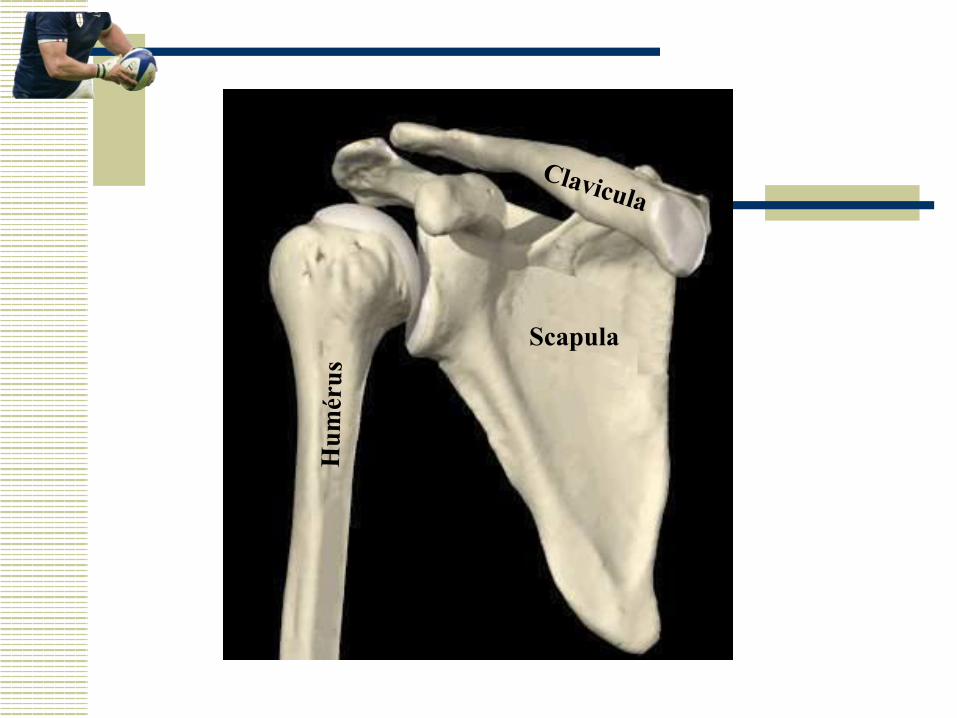
Clavicula
Scapula H
umér
us
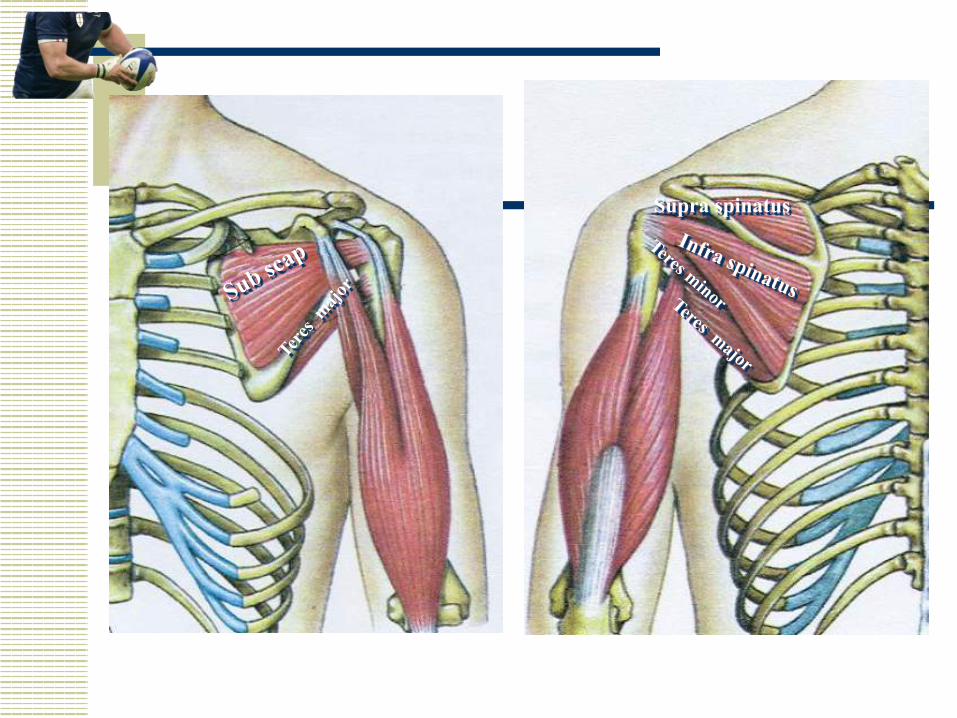
Supra spinatus
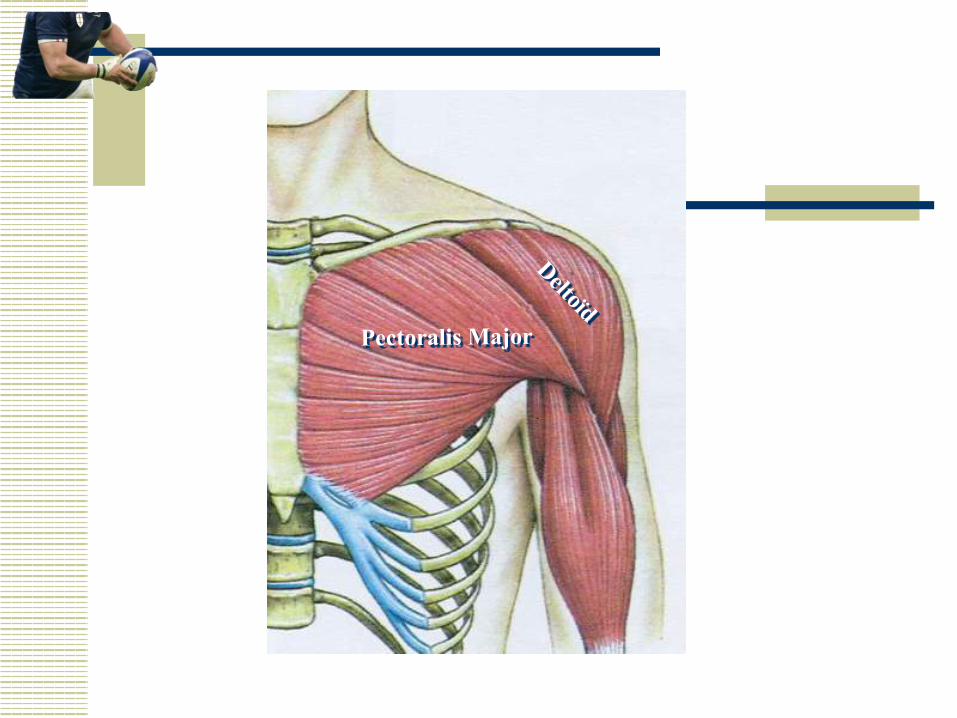
Pectoralis Major
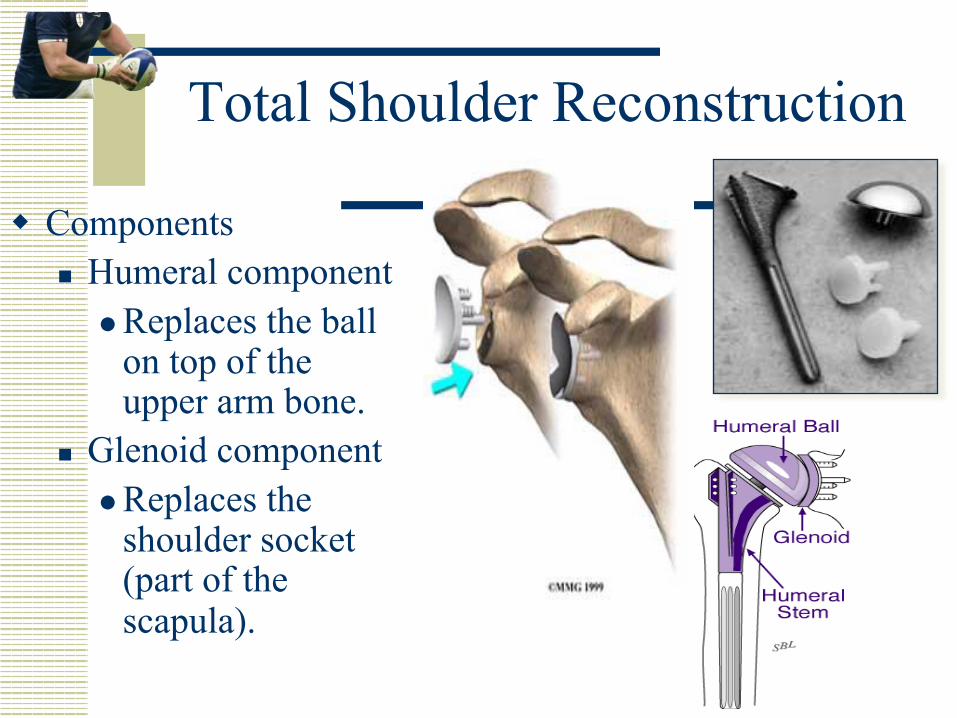
Total Shoulder Reconstruction
w Components n Humeral component
l Replaces the ball on top of the upper arm bone.
n Glenoid component l Replaces the
shoulder socket (part of the scapula).
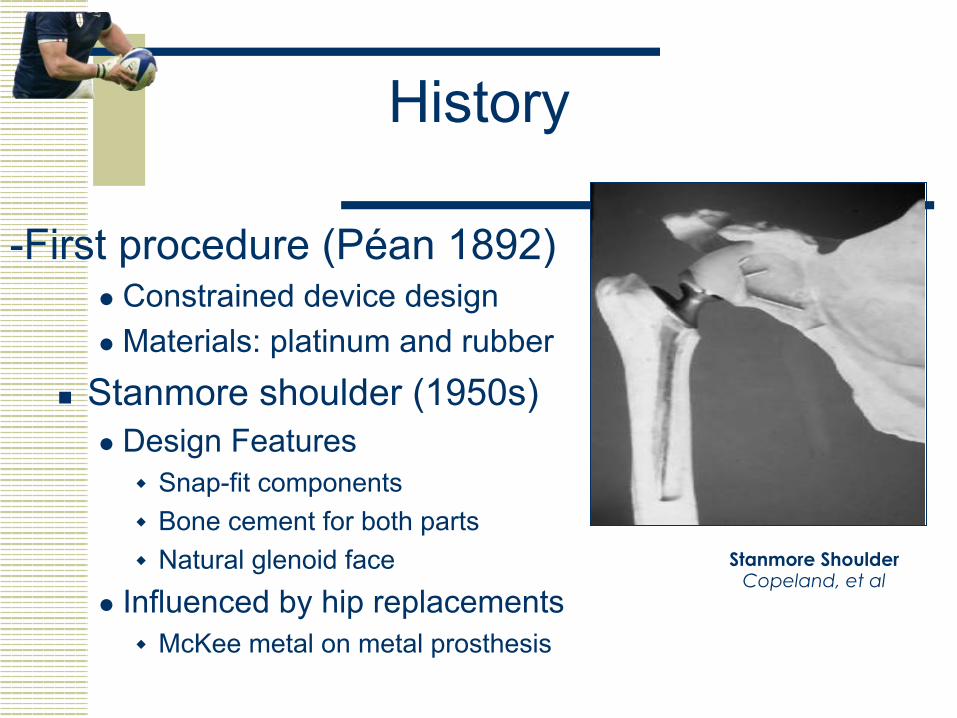
History
-First procedure (Péan 1892) l Constrained device design l Materials: platinum and rubber
n Stanmore shoulder (1950s) l Design Features
w Snap-fit components w Bone cement for both parts w Natural glenoid face
l Influenced by hip replacements w McKee metal on metal prosthesis
Stanmore Shoulder Copeland, et al
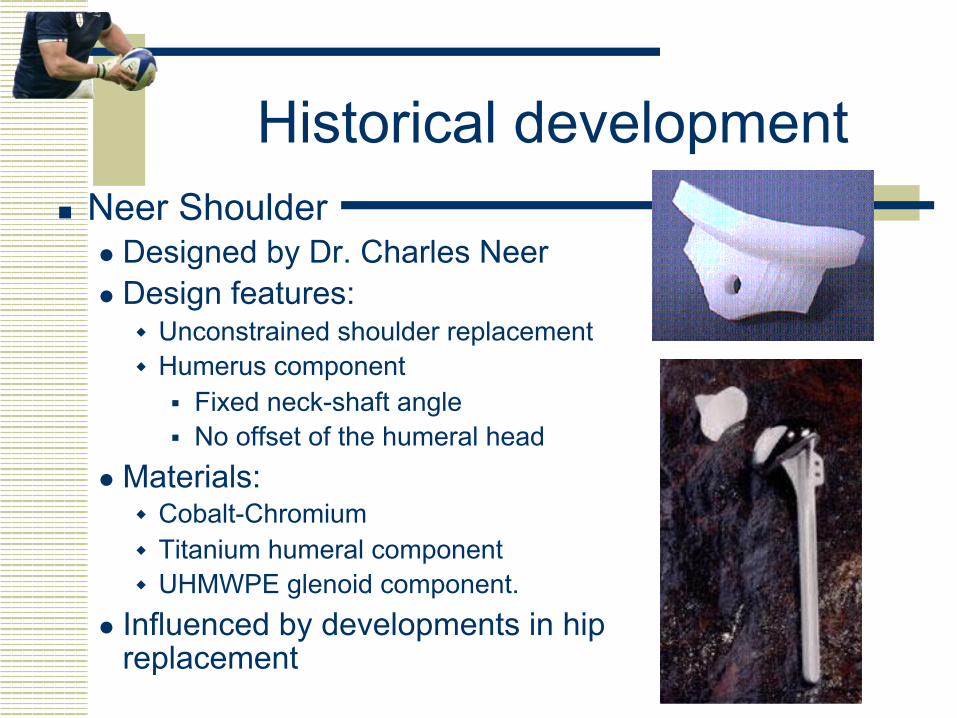
Historical development n Neer Shoulder
l Designed by Dr. Charles Neer l Design features:
w Unconstrained shoulder replacement w Humerus component
§ Fixed neck-shaft angle § No offset of the humeral head
l Materials: w Cobalt-Chromium w Titanium humeral component w UHMWPE glenoid component.
l Influenced by developments in hip replacement
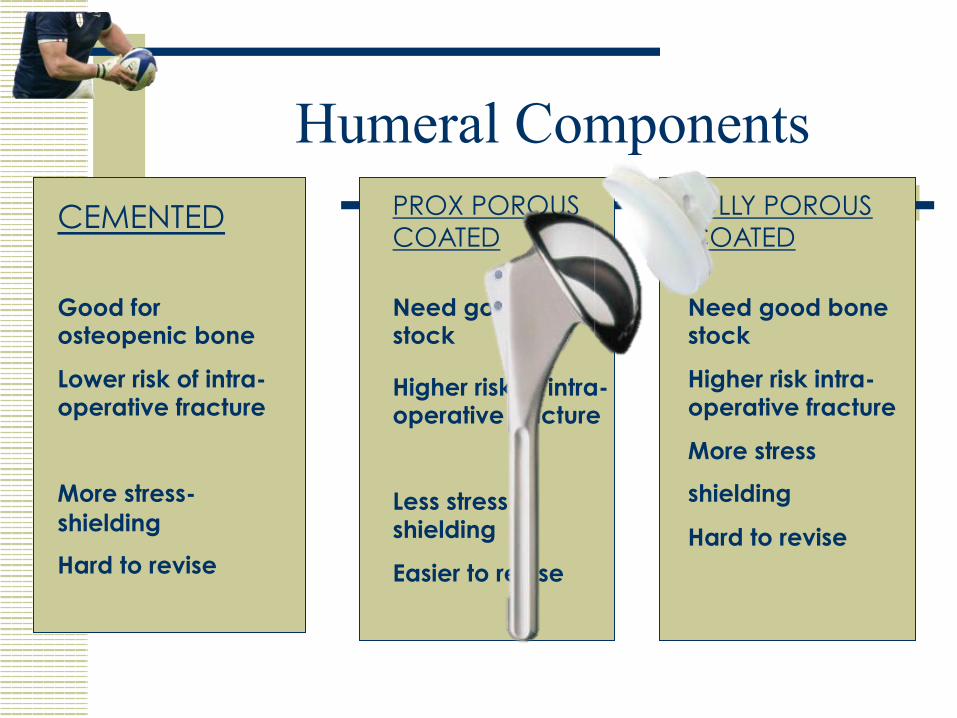
Humeral Components CEMENTED
Good for osteopenic bone
Lower risk of intra-operative fracture
More stress-shielding
Hard to revise
PROX POROUS COATED
FULLY POROUS COATED
Higher risk of intra-operative fracture
Less stress-shielding
Easier to revise
Need good bone stock
Need good bone stock
Higher risk intra-operative fracture
More stress
shielding
Hard to revise
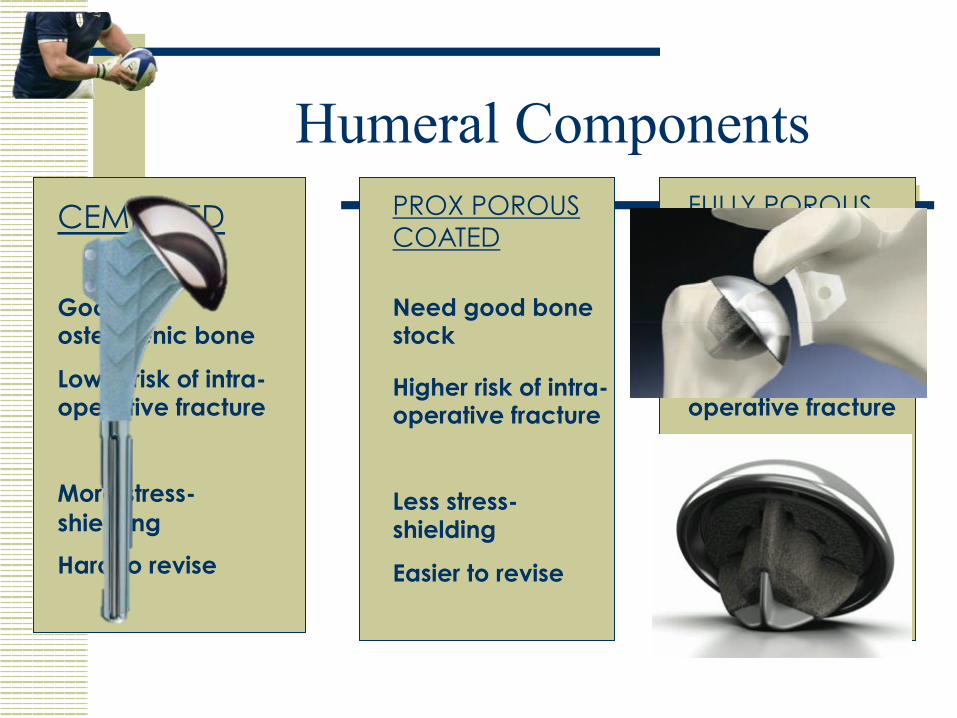
Humeral Components PROX POROUS COATED
Higher risk of intra-operative fracture
Less stress-shielding
Easier to revise
Need good bone stock
CEMENTED FULLY POROUS COATED
Good for osteopenic bone
Lower risk of intra-operative fracture
More stress-shielding
Hard to revise
Need good bone stock
Higher risk intra-operative fracture
More stress
shielding
Hard to revise
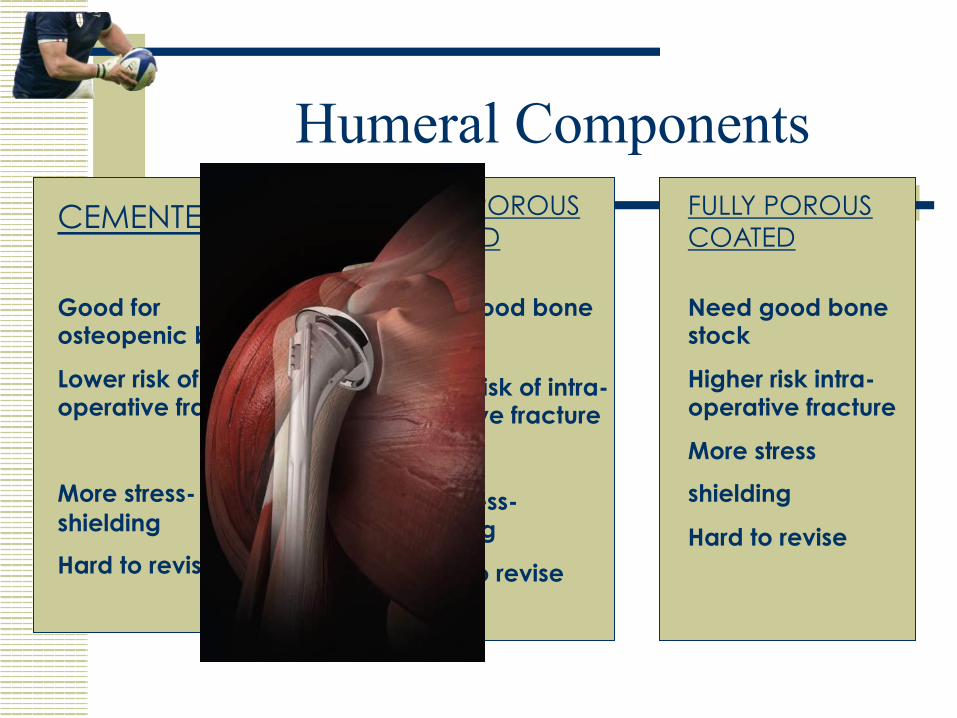
Humeral Components FULLY POROUS COATED
CEMENTED PROX POROUS COATED
Good for osteopenic bone
Lower risk of intra-operative fracture
More stress-shielding
Hard to revise
Higher risk of intra-operative fracture
Less stress-shielding
Easier to revise
Need good bone stock
Need good bone stock
Higher risk intra-operative fracture
More stress
shielding
Hard to revise
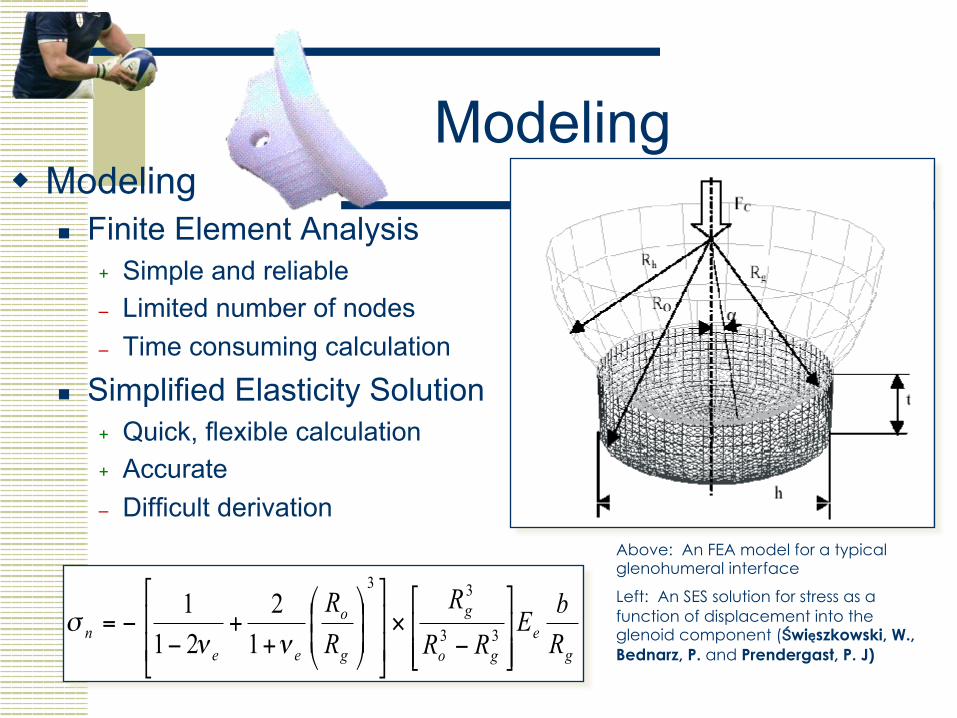
Modeling w Modeling
n Finite Element Analysis + Simple and reliable – Limited number of nodes – Time consuming calculation
n Simplified Elasticity Solution + Quick, flexible calculation + Accurate – Difficult derivation
ge
go
g
g
o
een R
bE
RR
R
RR
!!"
#
$$%
&
−×!!
"
#
$$
%
&
))*
+,,-
.
++
−−= 33
33
12
211
ννσ
Above: An FEA model for a typical glenohumeral interface
Left: An SES solution for stress as a function of displacement into the glenoid component (Święszkowski, W., Bednarz, P. and Prendergast, P. J)
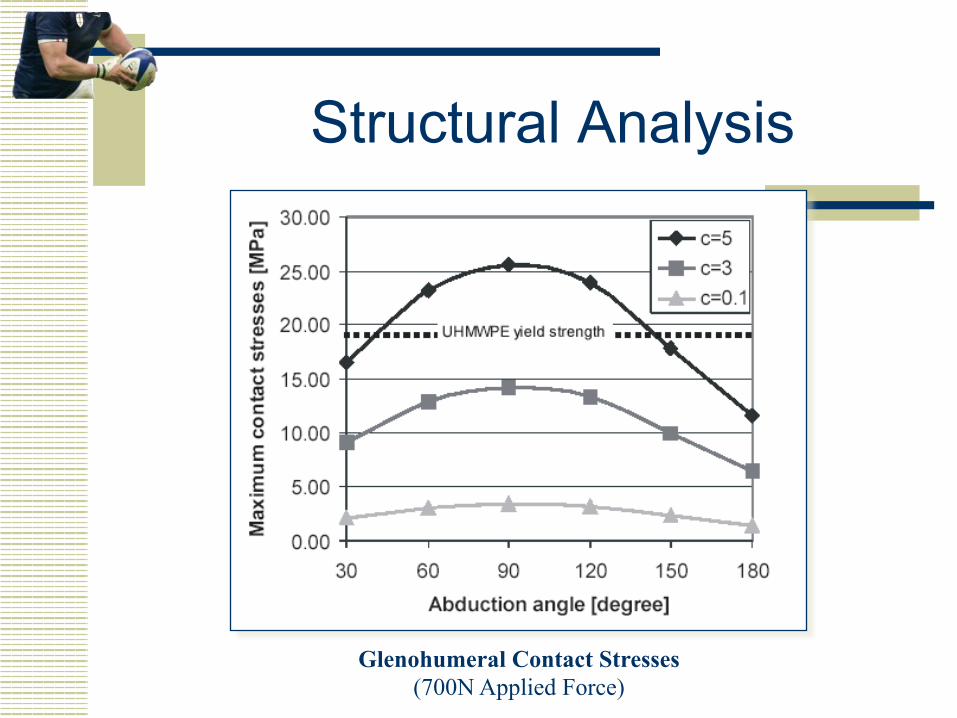
Structural Analysis
Glenohumeral Contact Stresses (700N Applied Force)
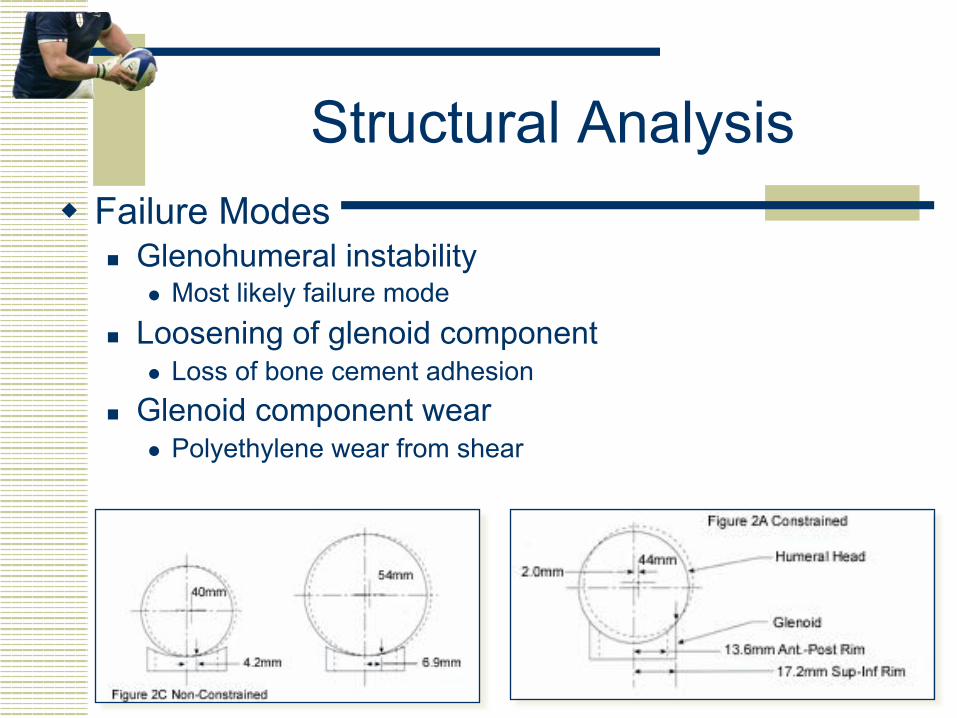
Structural Analysis w Failure Modes
n Glenohumeral instability l Most likely failure mode
n Loosening of glenoid component l Loss of bone cement adhesion
n Glenoid component wear l Polyethylene wear from shear
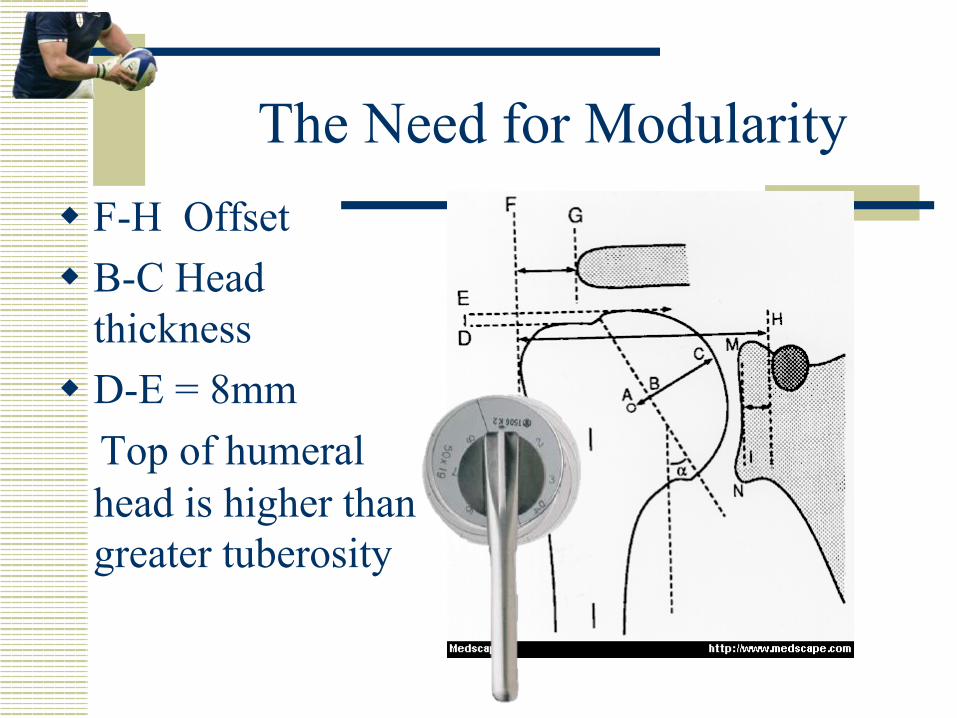
The Need for Modularity w F-H Offset w B-C Head
thickness w D-E = 8mm Top of humeral
head is higher than greater tuberosity
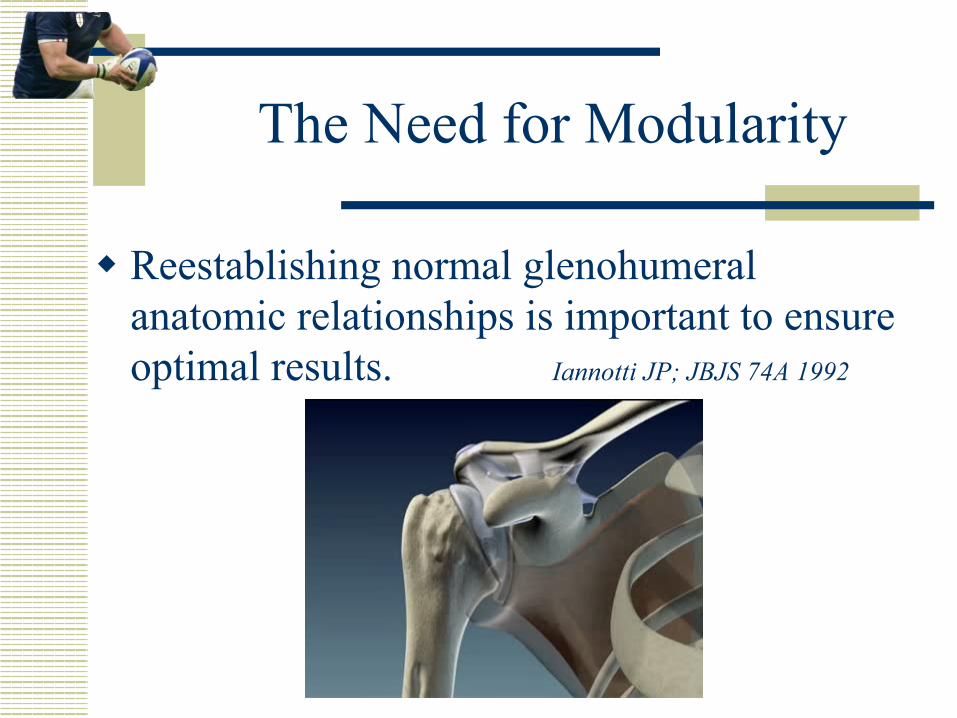
The Need for Modularity
w Reestablishing normal glenohumeral anatomic relationships is important to ensure optimal results. Iannotti JP; JBJS 74A 1992
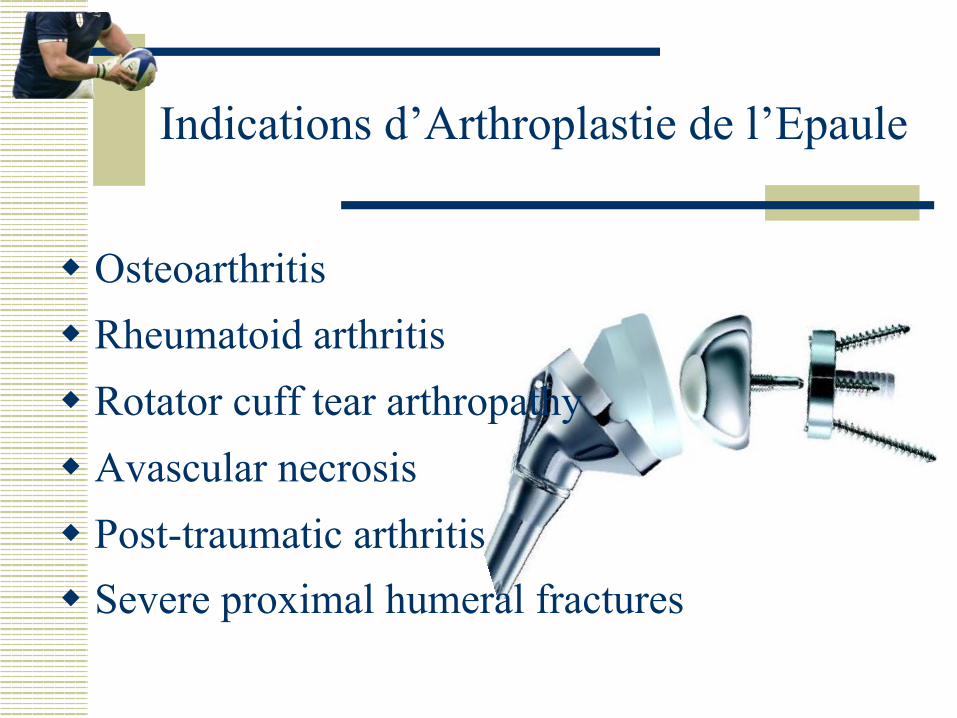
Indications d’Arthroplastie de l’Epaule
w Osteoarthritis w Rheumatoid arthritis w Rotator cuff tear arthropathy w Avascular necrosis w Post-traumatic arthritis w Severe proximal humeral fractures
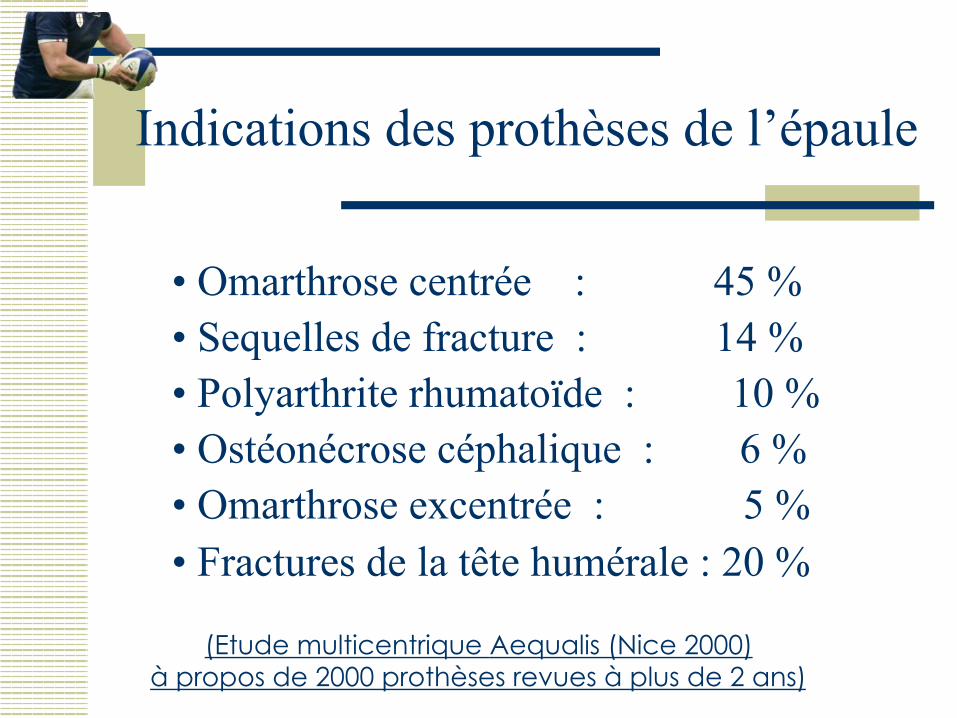
Indications des prothèses de l’épaule
• Omarthrose centrée : 45 % • Sequelles de fracture : 14 % • Polyarthrite rhumatoïde : 10 % • Ostéonécrose céphalique : 6 % • Omarthrose excentrée : 5 % • Fractures de la tête humérale : 20 %
(Etude multicentrique Aequalis (Nice 2000) à propos de 2000 prothèses revues à plus de 2 ans)
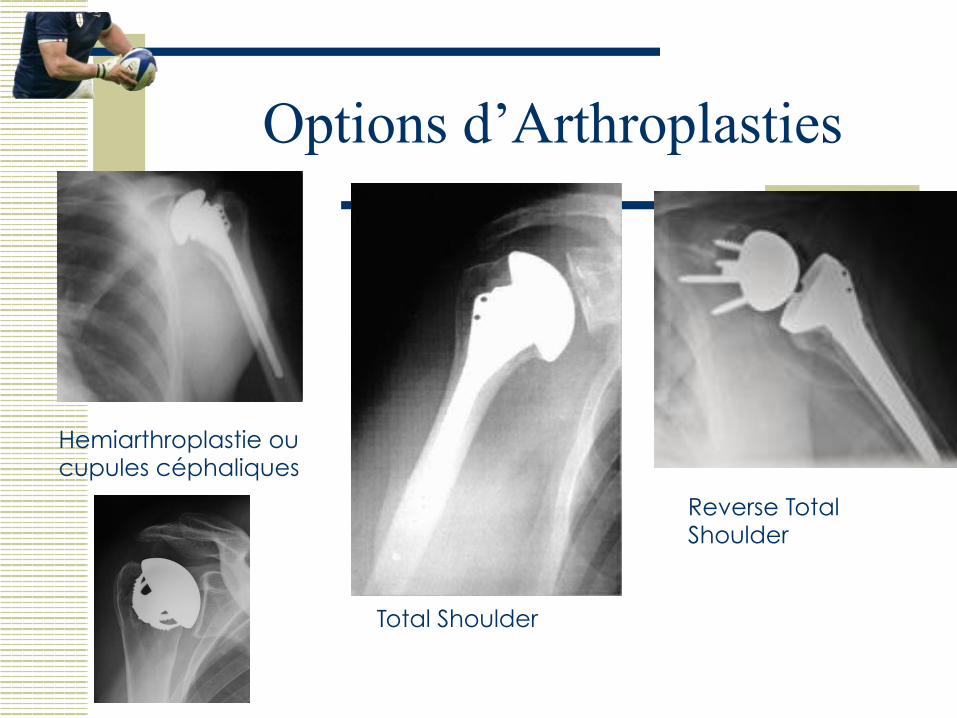
Hemiarthroplastie ou cupules céphaliques
Total Shoulder
Reverse Total Shoulder
Options d’Arthroplasties

Omarthrose centrée
w Classification de Samilson n Stade 0 : pas d’arthrose n Stade 1 : osteophyte inf < 3 mm n Stade 2 : 3 > osteophyte > 7 mm n Stade 3 : osteophyte > 7 mm + pincement gléno-huméral
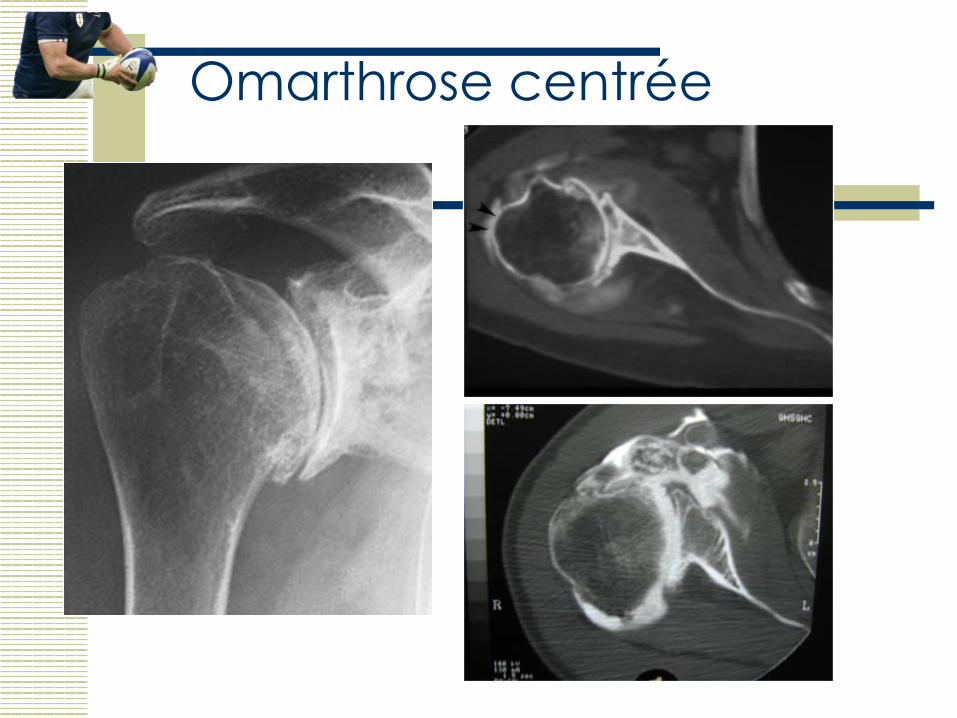
Omarthrose centrée
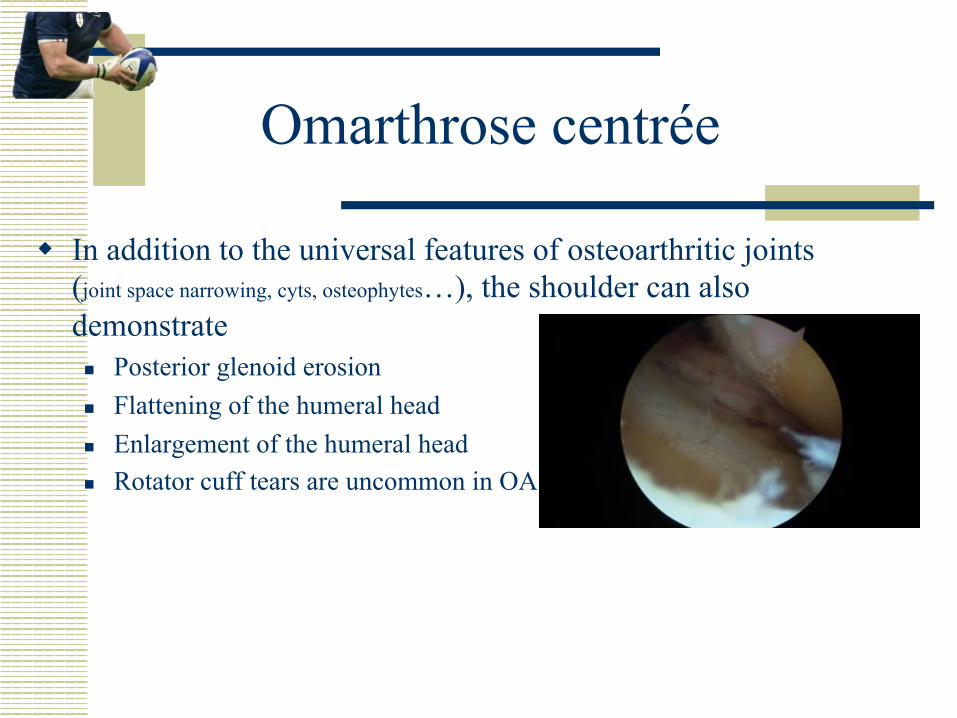
w In addition to the universal features of osteoarthritic joints (joint space narrowing, cyts, osteophytes…), the shoulder can also demonstrate n Posterior glenoid erosion n Flattening of the humeral head n Enlargement of the humeral head n Rotator cuff tears are uncommon in OA
Omarthrose centrée
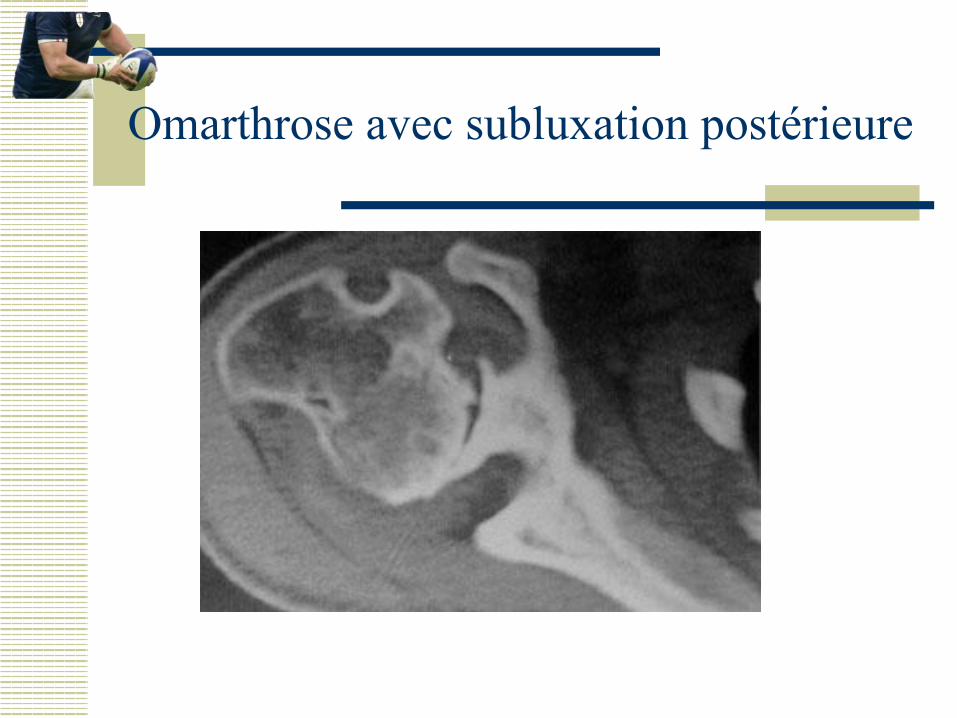
Omarthrose avec subluxation postérieure
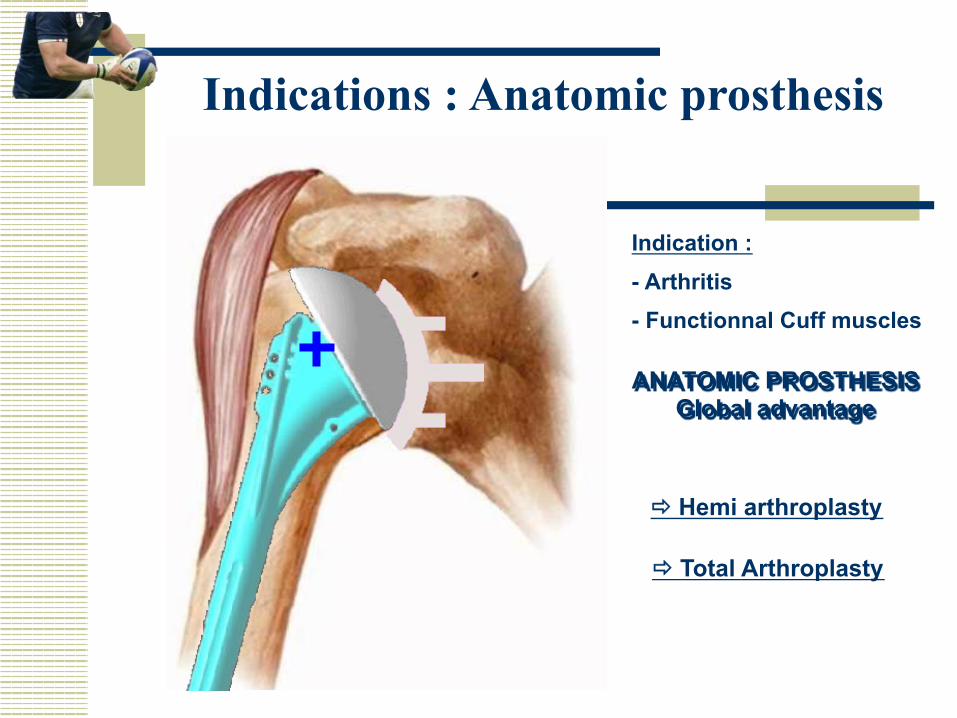
Indications : Anatomic prosthesis
Indication : - Arthritis - Functionnal Cuff muscles
ð Hemi arthroplasty
ð Total Arthroplasty
ANATOMIC PROSTHESIS Global advantage
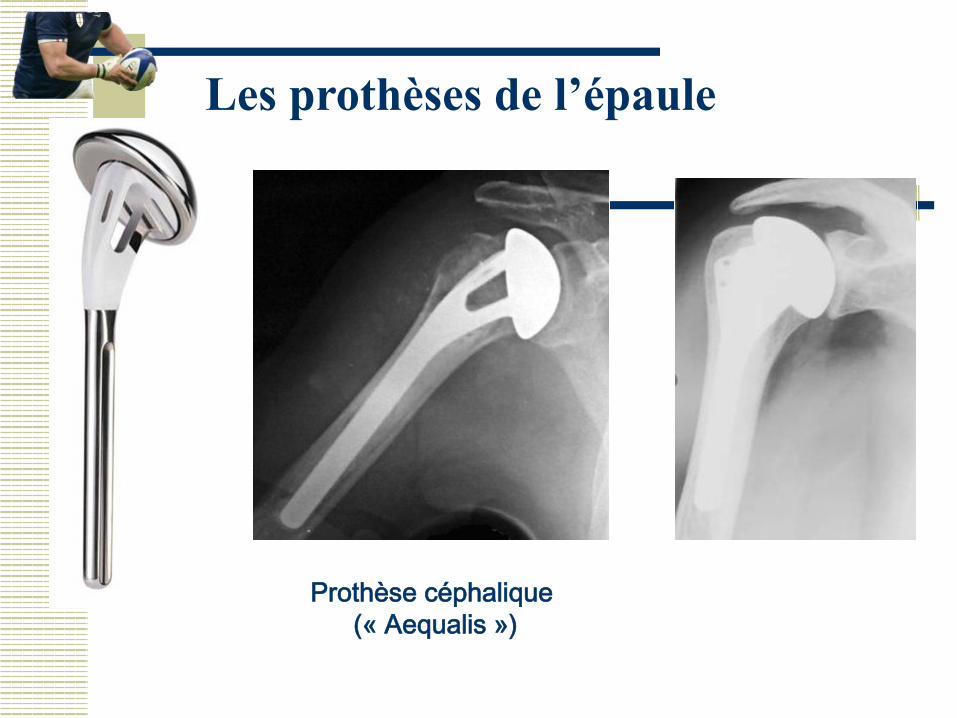
Les prothèses de l’épaule
Prothèse céphalique (« Aequalis »)
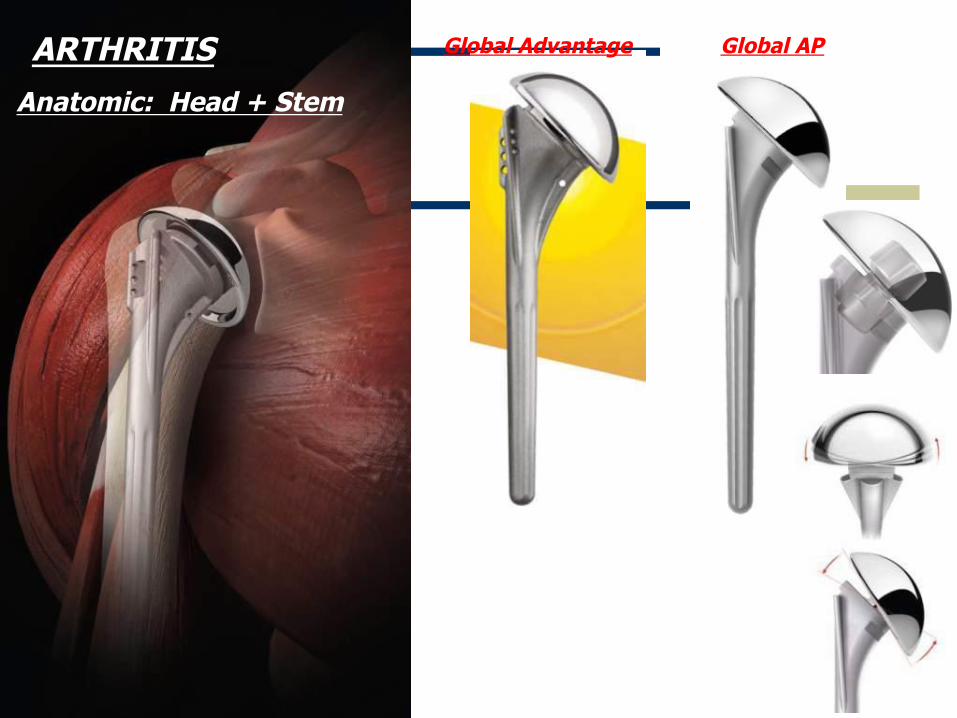
Anatomic: Head + Stem
Global Advantage Global AP ARTHRITIS
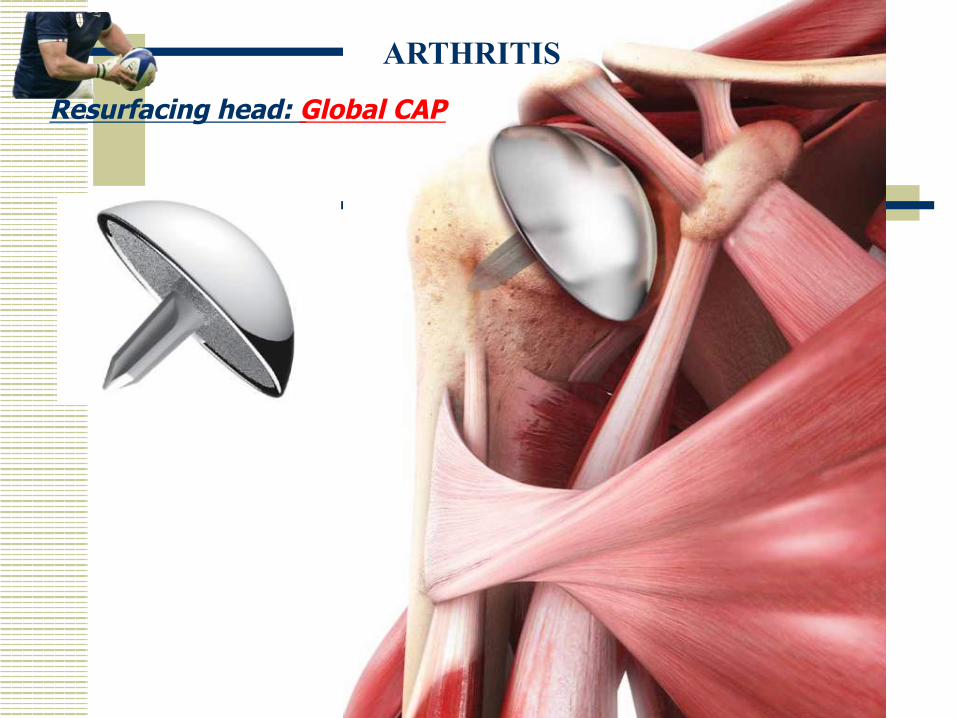
Resurfacing head: Global CAP
ARTHRITIS
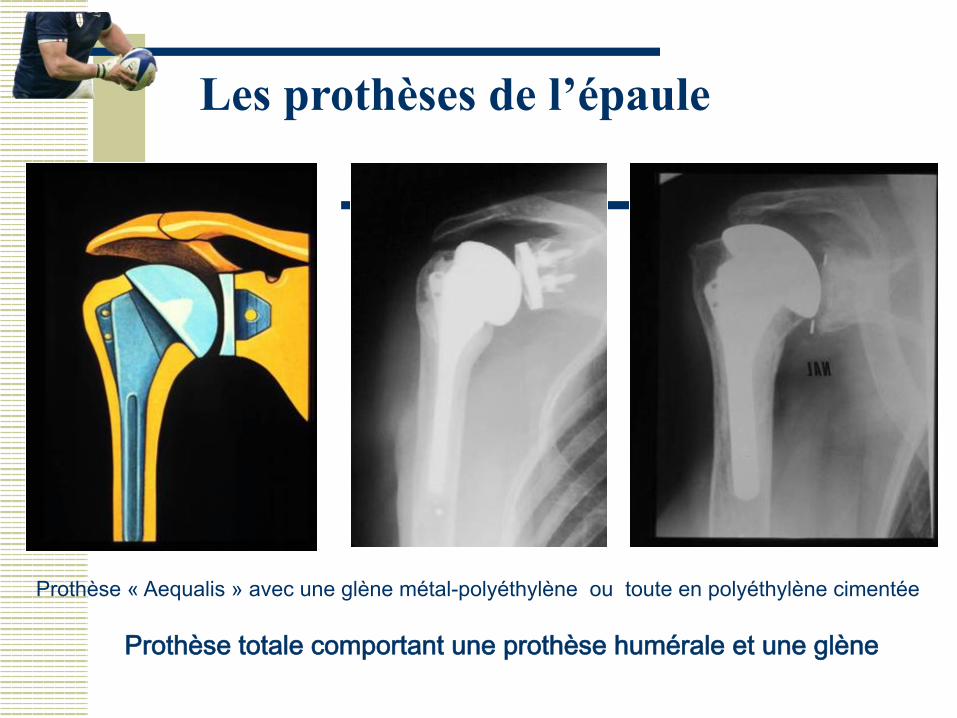
Les prothèses de l’épaule
Prothèse totale comportant une prothèse humérale et une glène
Prothèse « Aequalis » avec une glène métal-polyéthylène ou toute en polyéthylène cimentée
Hemi versus Total Shoulder
w Easy procedure w Short Operating time w Less risk of instability w Can be revised to TSA û Less reliable pain relief û Progressive Glenoid erosion
may cause results to deteriorate over time
û Need concentric glenoid
w More consistent pain relief w Better fulcrum for active
motion
û Difficult procedure û Longer OR time û Poly wear can cause
loosening of both components û More Glenoid bone loss
Recommendations based on Evidence
w The results of arthroplasty in osteoarthritis of the shoulder. Haines JF et al. J Bone Joint Surg Br. 2006 Apr;88(4):496-501
w Prospective study of 124 shoulder arthroplasties for OA
(Hemi and TSA) w Similar improvement in pain and function in both groups if
rotator cuff was intact . Better results with Hemi if + rotator cuff tear
w Hemi à Revision at mean of 1.5 years for glenoid pain w TSA à Revision at mean of 4.5 years for glenoid loosening

Les indications des prothèses de l’épaule dépendent de l’état de la coiffe
Prothèse totale stable sur omarthrose centrée avec coiffe correcte
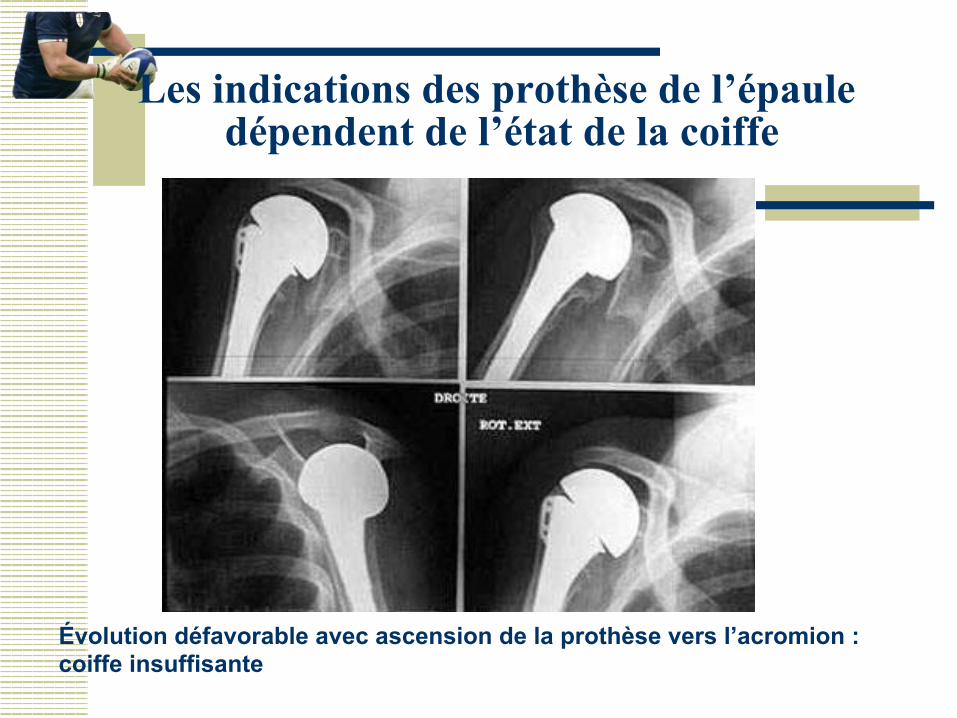
Les indications des prothèse de l’épaule dépendent de l’état de la coiffe
Évolution défavorable avec ascension de la prothèse vers l’acromion : coiffe insuffisante
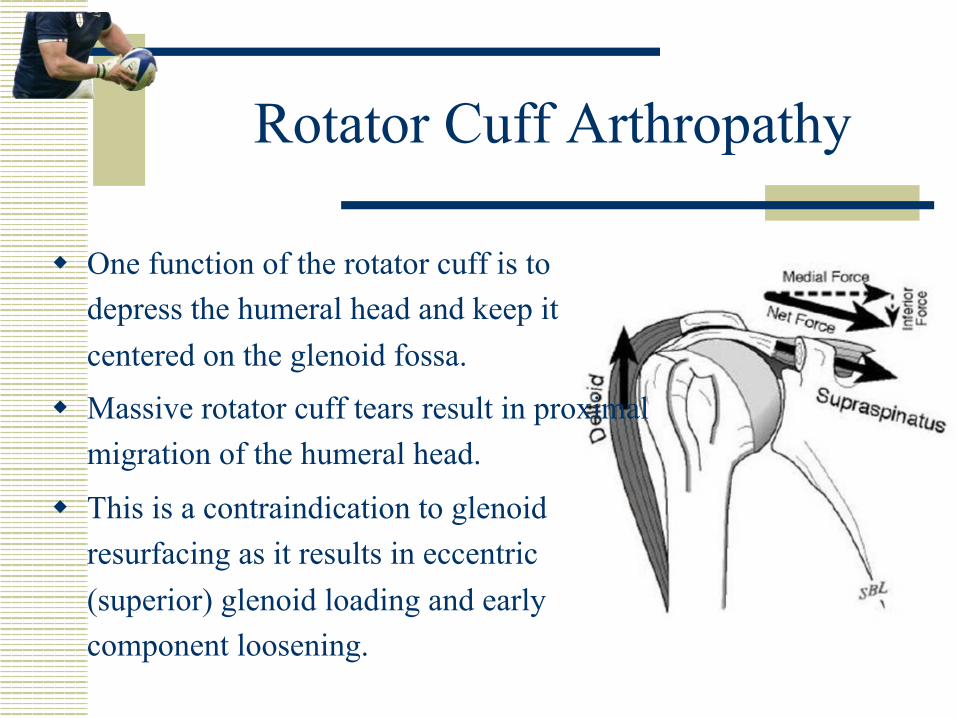
Rotator Cuff Arthropathy
w One function of the rotator cuff is to depress the humeral head and keep it centered on the glenoid fossa.
w Massive rotator cuff tears result in proximal migration of the humeral head.
w This is a contraindication to glenoid resurfacing as it results in eccentric (superior) glenoid loading and early component loosening.
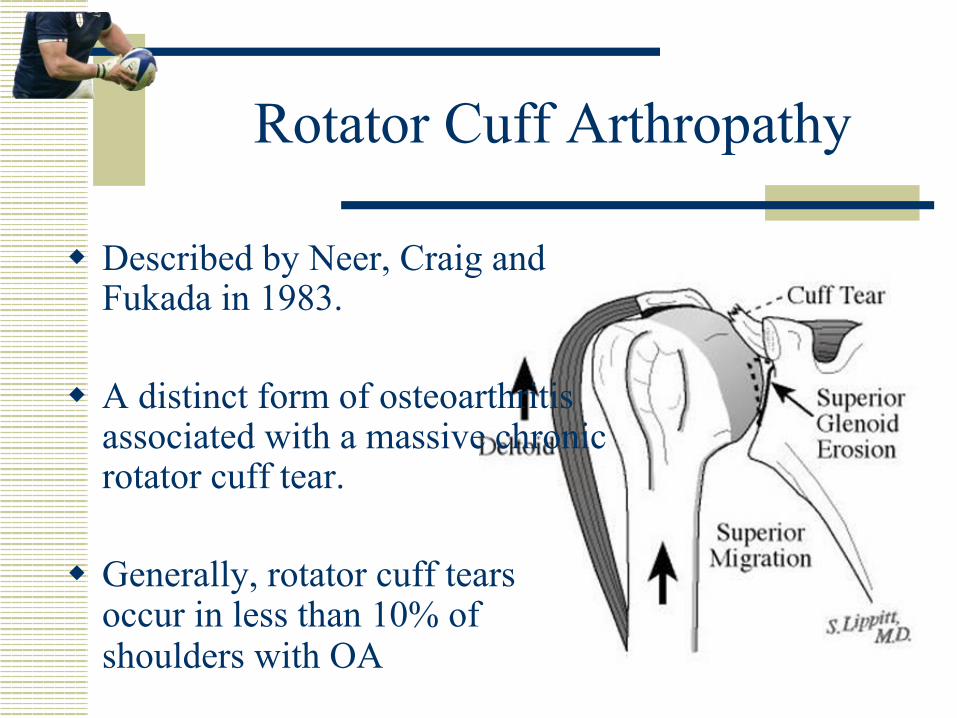
Rotator Cuff Arthropathy
w Described by Neer, Craig and Fukada in 1983.
w A distinct form of osteoarthritis associated with a massive chronic rotator cuff tear.
w Generally, rotator cuff tears
occur in less than 10% of shoulders with OA
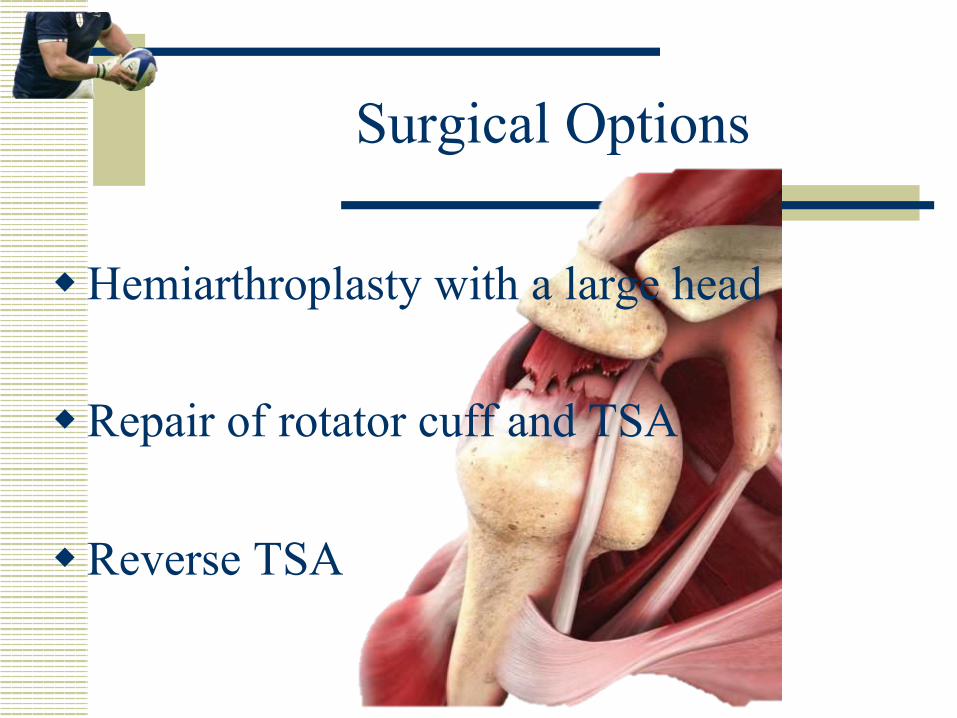
Surgical Options
w Hemiarthroplasty with a large head
w Repair of rotator cuff and TSA
w Reverse TSA
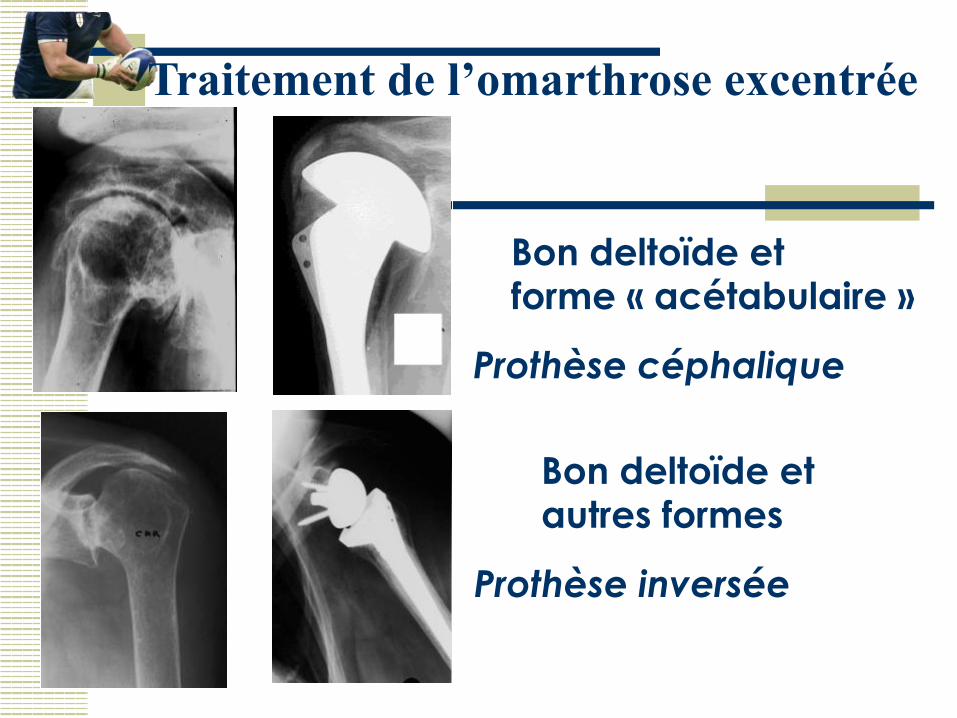
Traitement de l’omarthrose excentrée
Bon deltoïde et forme « acétabulaire »
Prothèse céphalique
Bon deltoïde et autres formes
Prothèse inversée mais mauvaise force en rot. ext.
Photos C. Lévigne
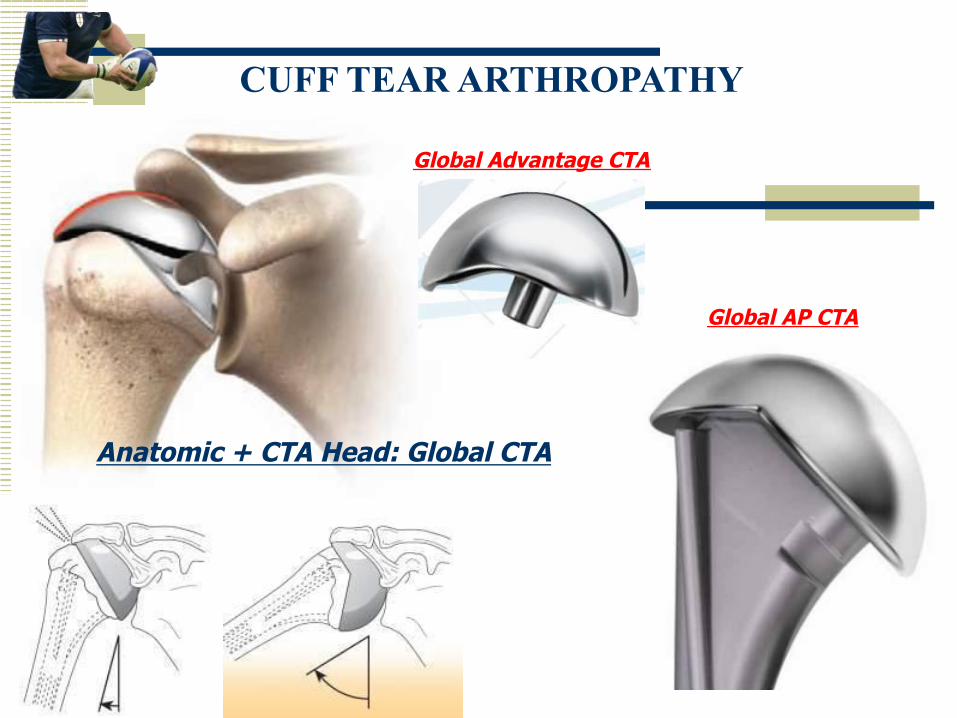
Anatomic + CTA Head: Global CTA
Global Advantage CTA
Global AP CTA
CUFF TEAR ARTHROPATHY
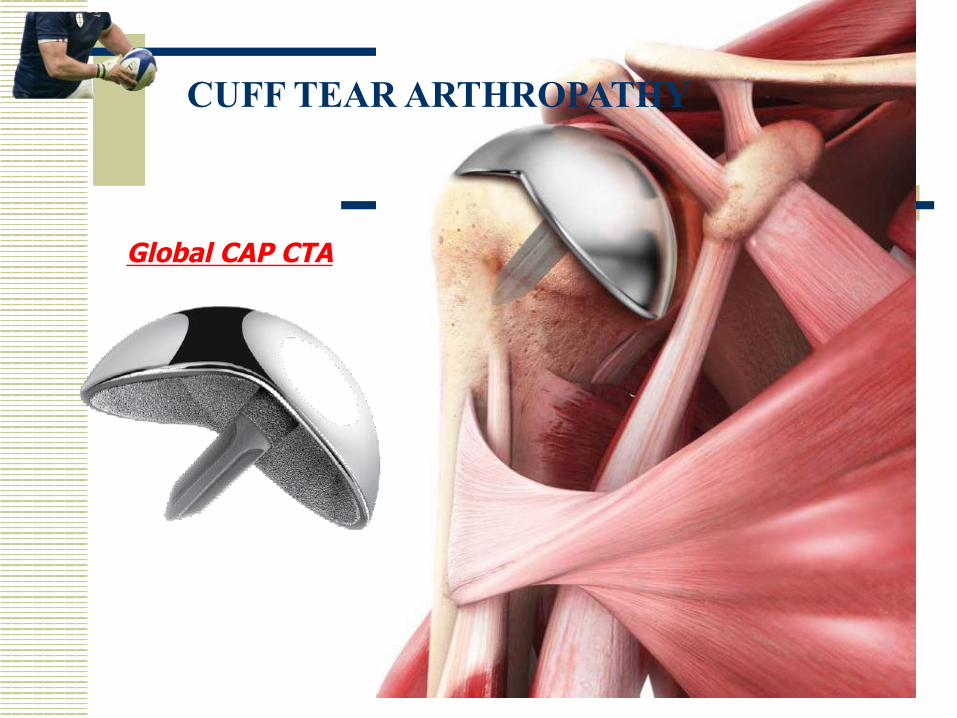
Global CAP CTA
CUFF TEAR ARTHROPATHY
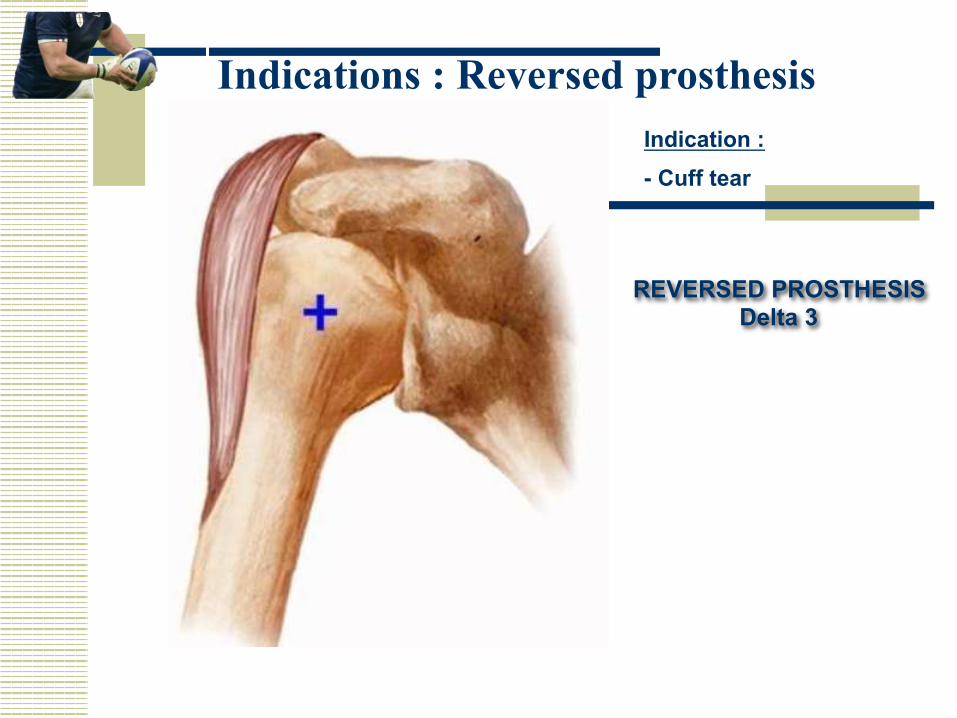
Indications : Reversed prosthesis
REVERSED PROSTHESIS Delta 3
Indication : - Cuff tear
Outcomes of Hemiarthroplasty
w Rockwood: 86% satisfactory results after 4 years
w Zuckerman: 93% adequate pain relief and 90% had improved function.
w Sanches-Sotelo: 75% modest improvements in ROM and strength. Good pain relief.
Outcomes of Hemiarthroplasty
w Field et al, and Sanchez-Sotelo reported that impaired deltoid function and previous subacromial decompression (loss of coracoacromial ligament) were significantly associated with clinical shoulder instability post hemiarthroplasty.
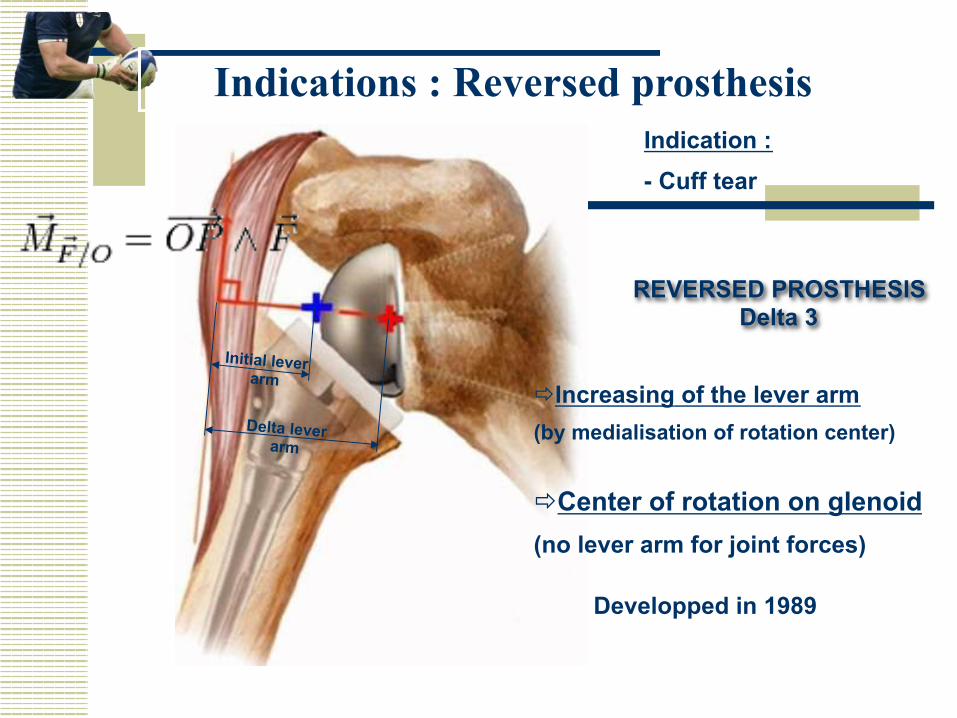
Indication : - Cuff tear
REVERSED PROSTHESIS Delta 3
ð Increasing of the lever arm (by medialisation of rotation center)
Initial lever arm
Delta lever arm
ð Center of rotation on glenoid (no lever arm for joint forces)
Developped in 1989
Indications : Reversed prosthesis
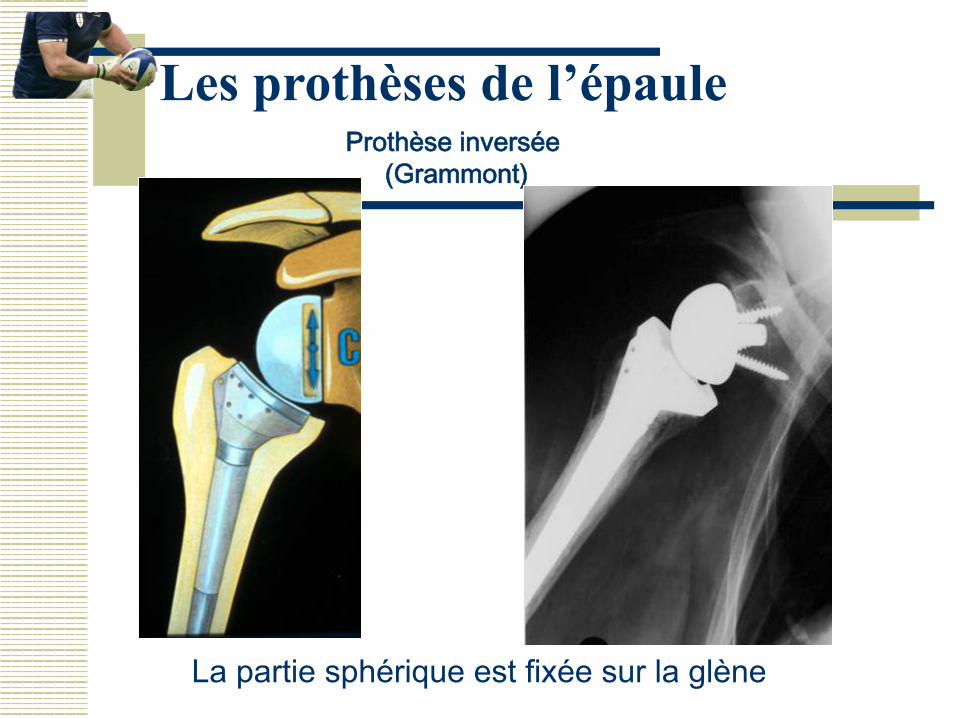
Les prothèses de l’épaule Prothèse inversée
(Grammont)
La partie sphérique est fixée sur la glène
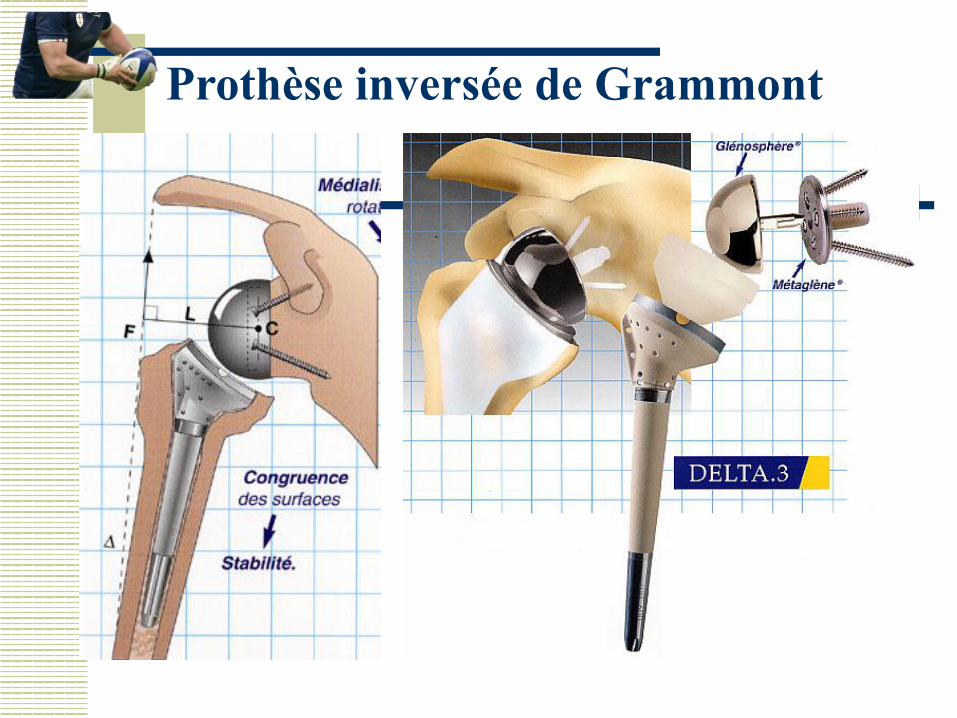
Prothèse inversée de Grammont
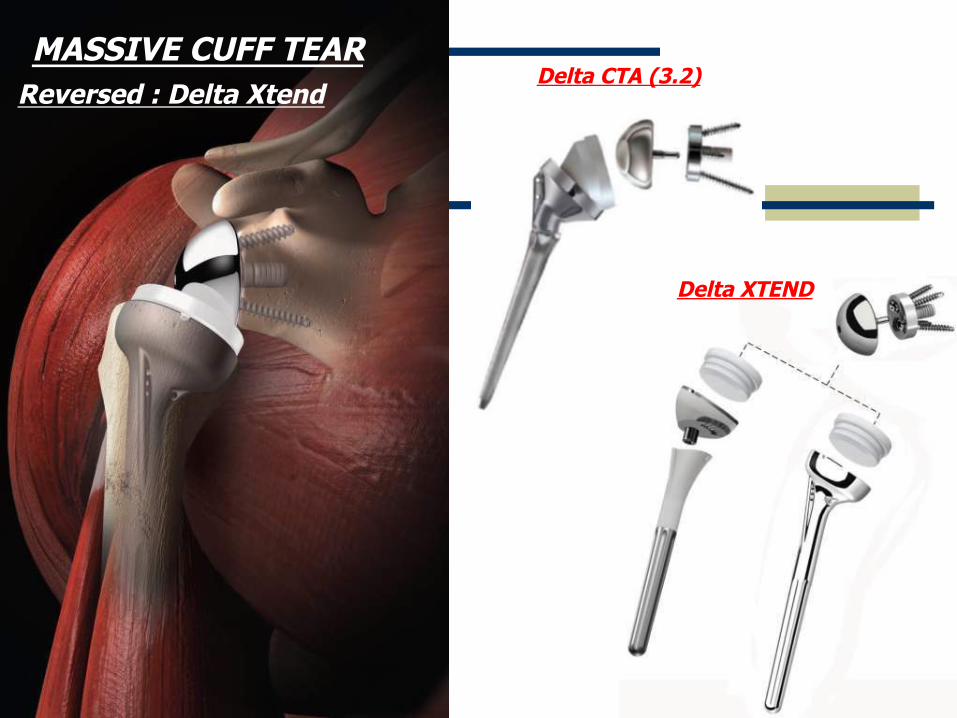
Reversed : Delta Xtend MASSIVE CUFF TEAR
Delta CTA (3.2)
Delta XTEND
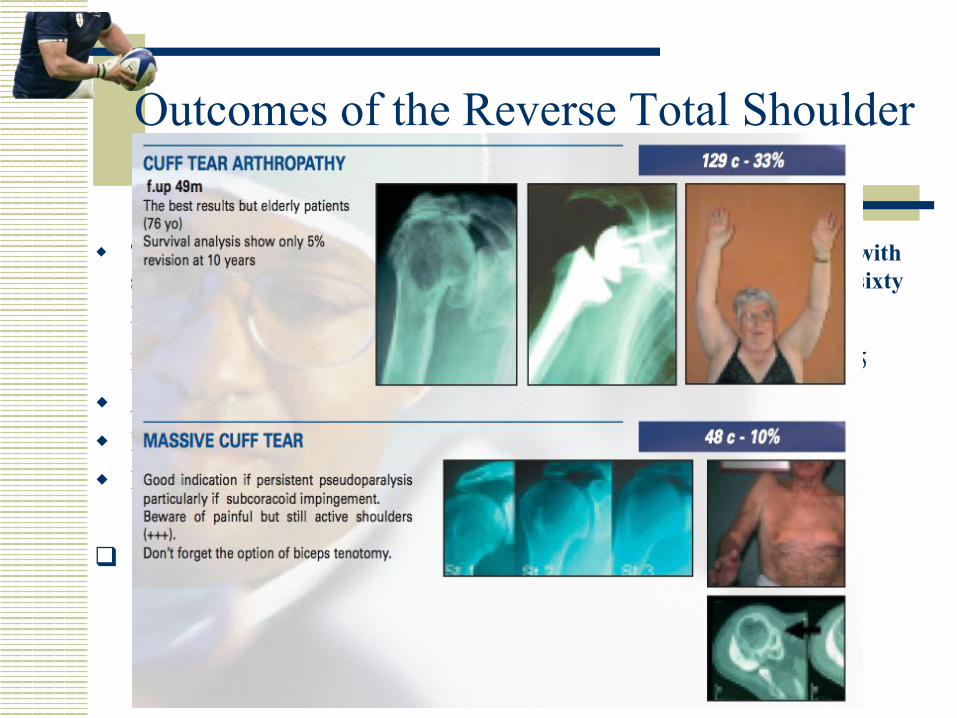
Outcomes of the Reverse Total Shoulder
w The Reverse Shoulder Prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency. A minimum two-year follow-up study of sixty patients.
Frankle M, Siegel S, J Bone Joint Surg Am. 2005 Aug;87(8):1697-705 w Average age = 70 w Improved ASES scores w Improved ROM Flex: 55 à 105° Abd: 41 à 102° q 17% Complication rate
7 failures à 5 revised to new Reverse TSA à 2 revised to Hemiarthroplasties
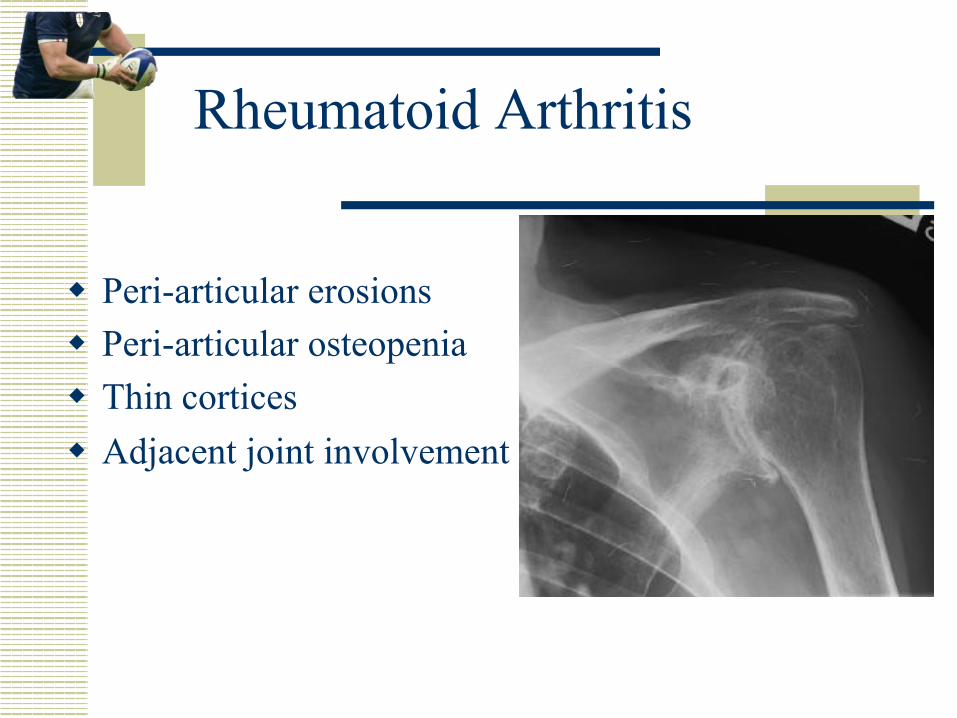
Rheumatoid Arthritis
w Peri-articular erosions w Peri-articular osteopenia w Thin cortices w Adjacent joint involvement
Rheumatoid Arthritis
w Cemented short-stemmed prosthesis w Gill, Cofield et al recommend at least 60mm
between the cement mantles of ipsilateral shoulder and elbow arthroplasties.
w If this cannot be achieved, join both cement mantles together.
Rheumatoid Arthritis
w Generally, TSA performed due to destruction of the glenoid articular surface by the disease.
w Glenoid erosion may require bone grafting, however, if glenoid is eroded to the level of the coracoid process, glenoid resurfacing is contraindicated
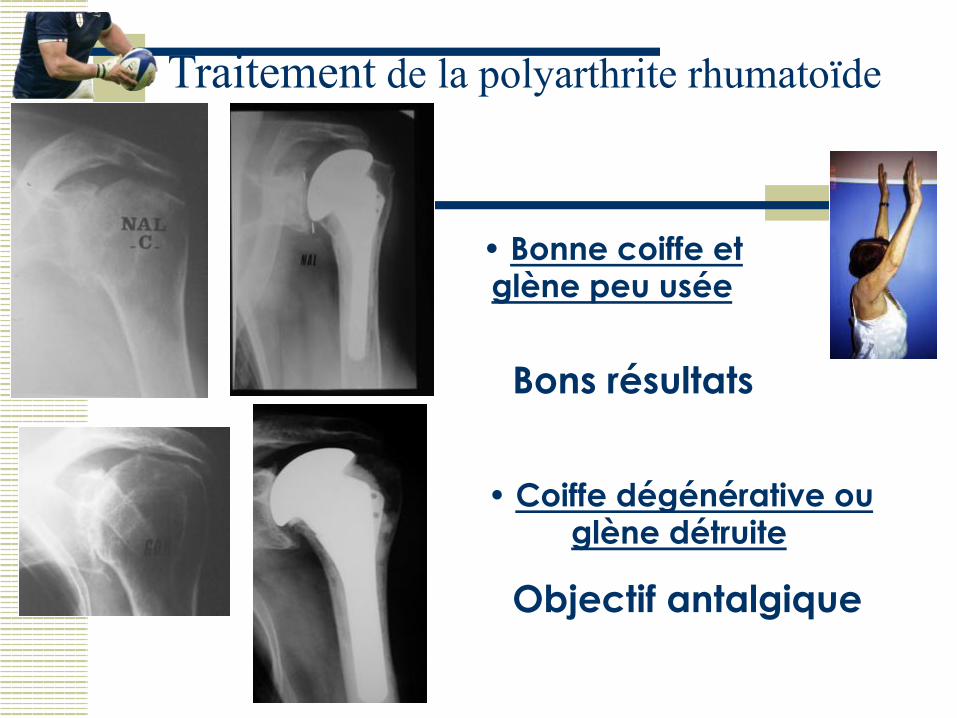
Traitement de la polyarthrite rhumatoïde
• Bonne coiffe et glène peu usée
Bons résultats
• Coiffe dégénérative ou glène détruite
Objectif antalgique
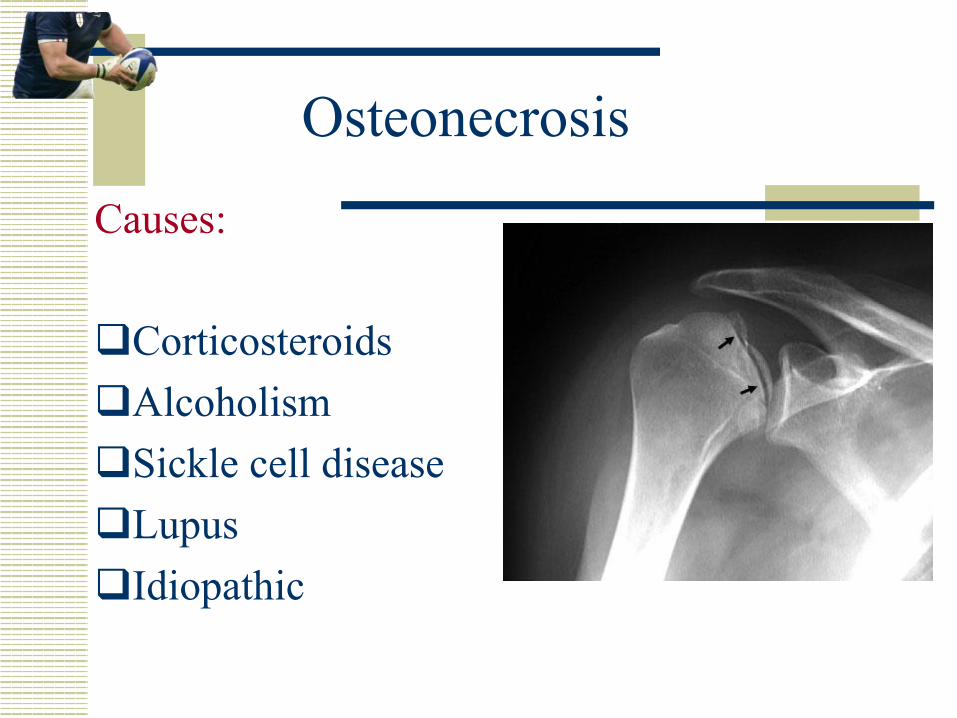
Osteonecrosis
Causes: q Corticosteroids q Alcoholism q Sickle cell disease q Lupus q Idiopathic
Osteonecrosis
w Usually young patients with adequate bone stock.
w Prefer proximally porous-coated, press-fit humeral prosthesis.
ü less stress-shielding ü easier to revise if necessary q Only resurface glenoid in stage V
osteonecrosis (glenoid erosion).
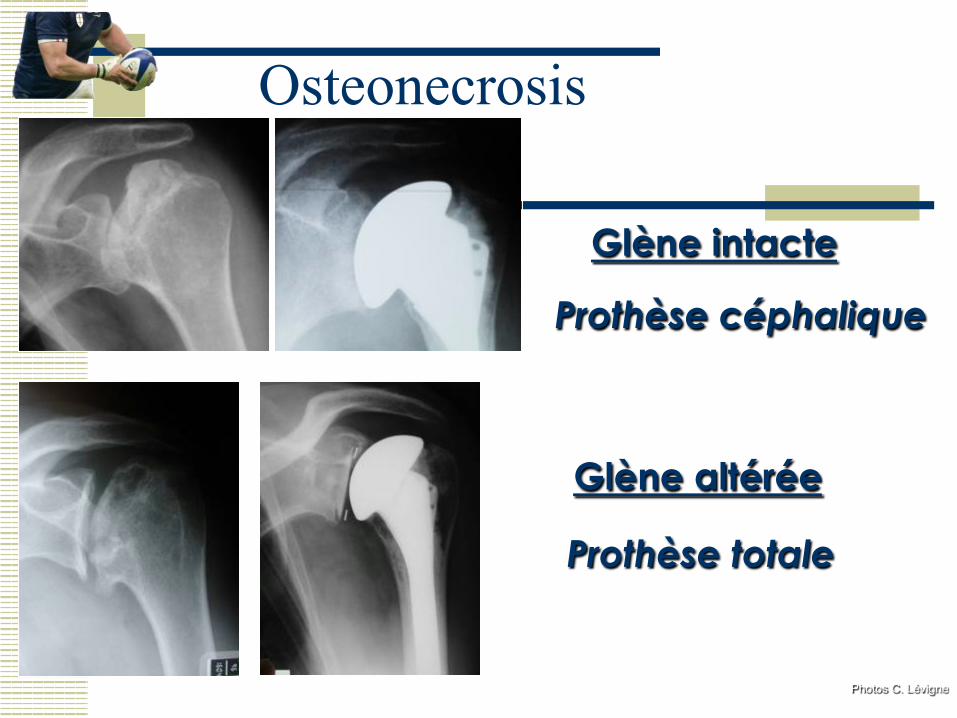
Glène intacte
Prothèse céphalique
Glène altérée
Prothèse totale
Photos C. Lévigne
Osteonecrosis

Nécrose de la tête humérale après traitement orthopédique d’une fracture
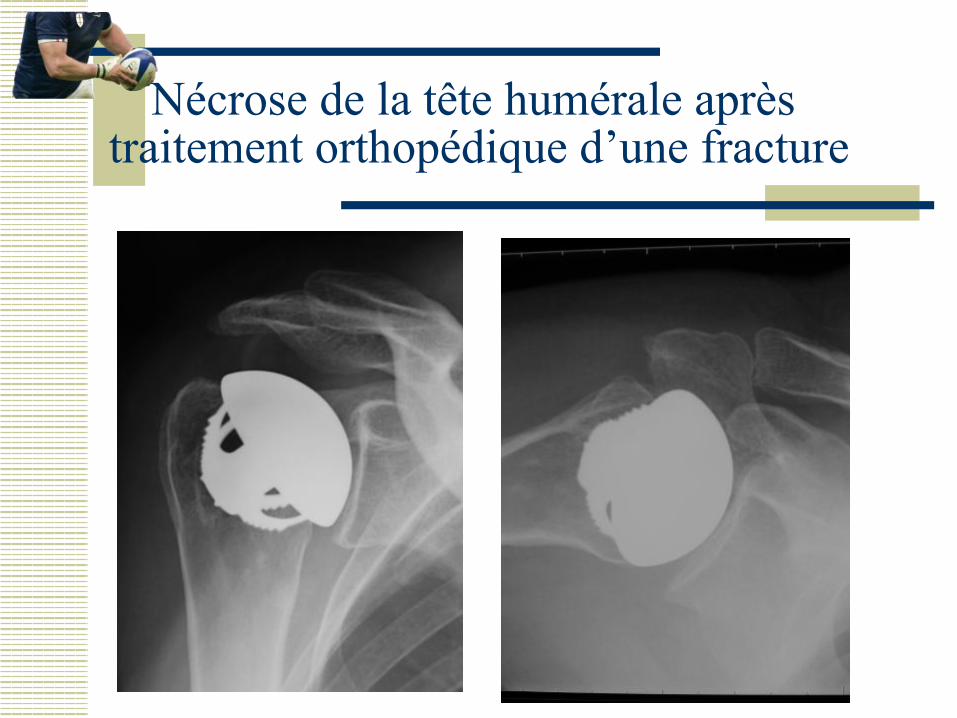
Nécrose de la tête humérale après traitement orthopédique d’une fracture

Post-Traumatic Arthritis
w Due to fractures treated conservatively w May have mal-union of tuberosities,
distorting normal anatomic landmarks w 12% of patients have axillary nerve palsies
(Neer). w Many have soft-tissue contractures and
muscle weakness
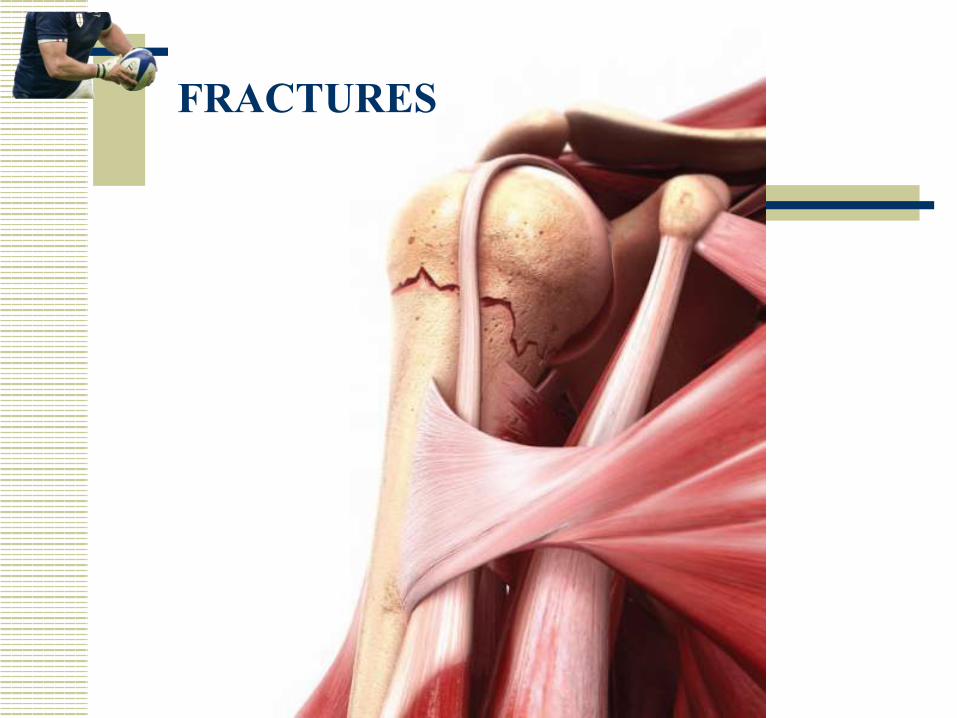
FRACTURES

Fracture stem: Global Fx FRACTURES
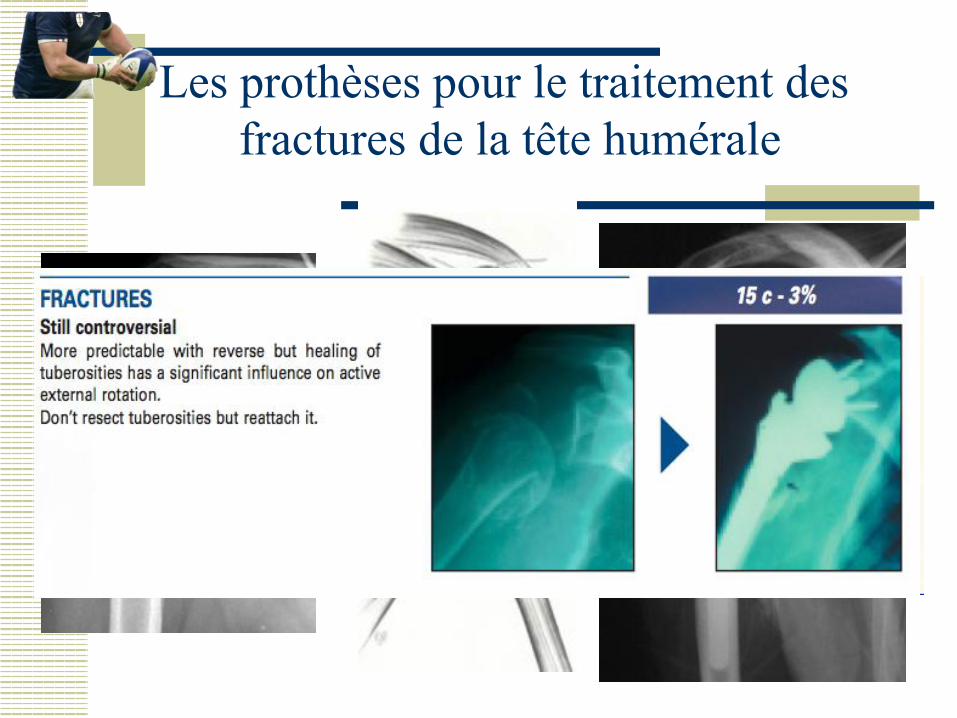
Les prothèses pour le traitement des fractures de la tête humérale

Les prothèses pour le traitement des fractures de la tête humérale
Difficultés pour rétablir : - Une hauteur correcte - Une rétroversion correcte - Trochiter et trochin en bonne place Conditions indispensables pour avoir un bon résultat fonctionnel
Après 70 ans
Fractures comminutives
Prothèses céphaliques
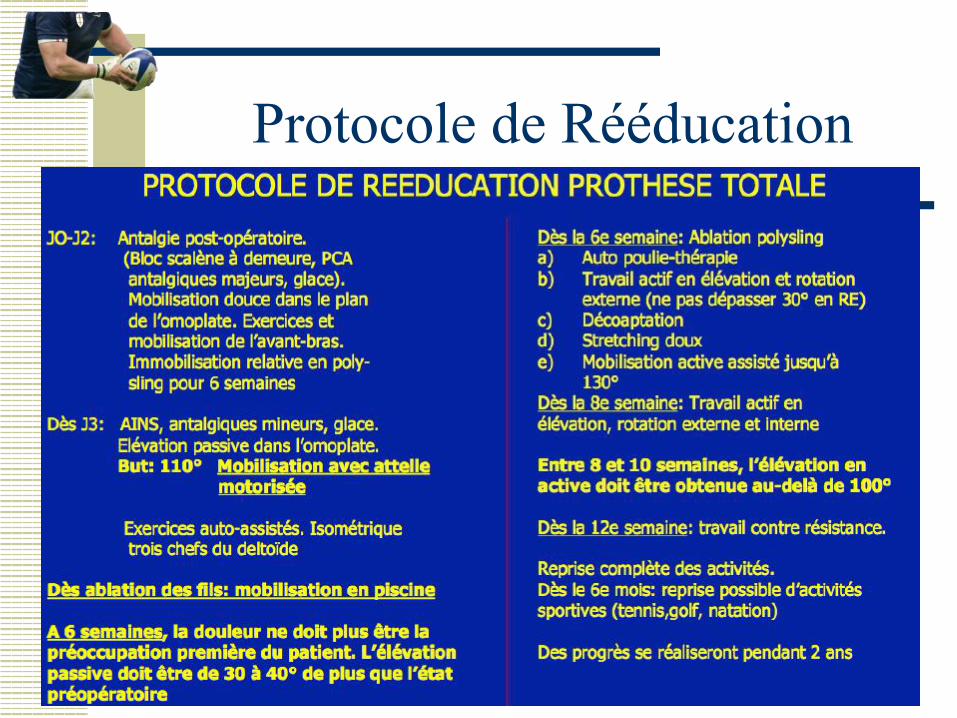
Protocole de Rééducation
Protocole de Rééducation Amélioration possible même après la deuxième année
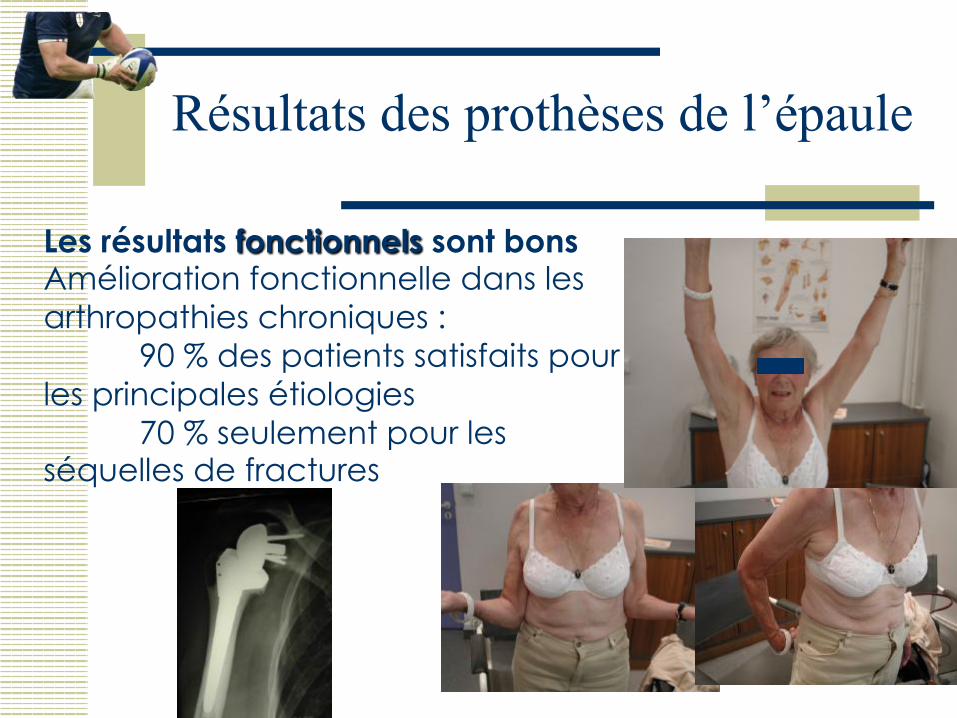
Les résultats fonctionnels sont bons Amélioration fonctionnelle dans les arthropathies chroniques :
90 % des patients satisfaits pour les principales étiologies
70 % seulement pour les séquelles de fractures
Résultats des prothèses de l’épaule
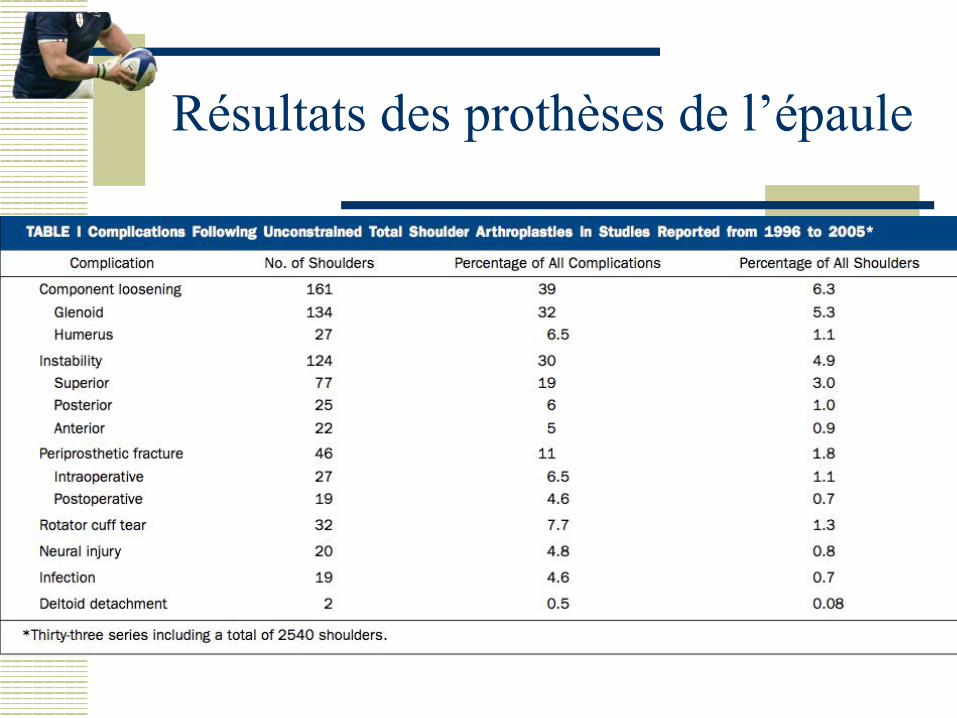
Résultats des prothèses de l’épaule
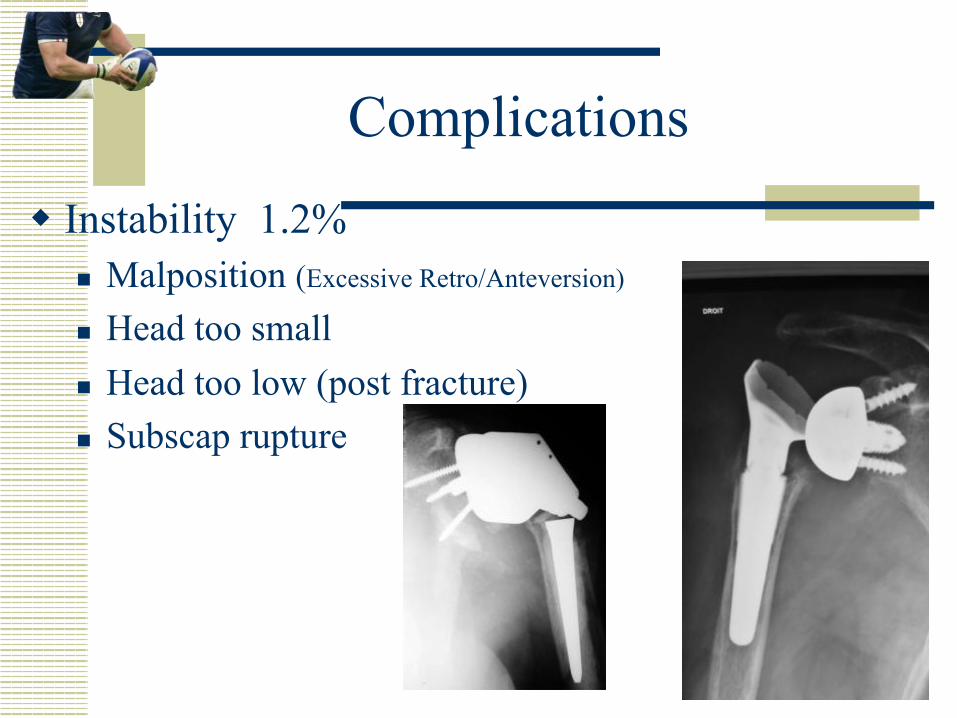
Complications
w Instability 1.2% n Malposition (Excessive Retro/Anteversion)
n Head too small n Head too low (post fracture) n Subscap rupture
Complications
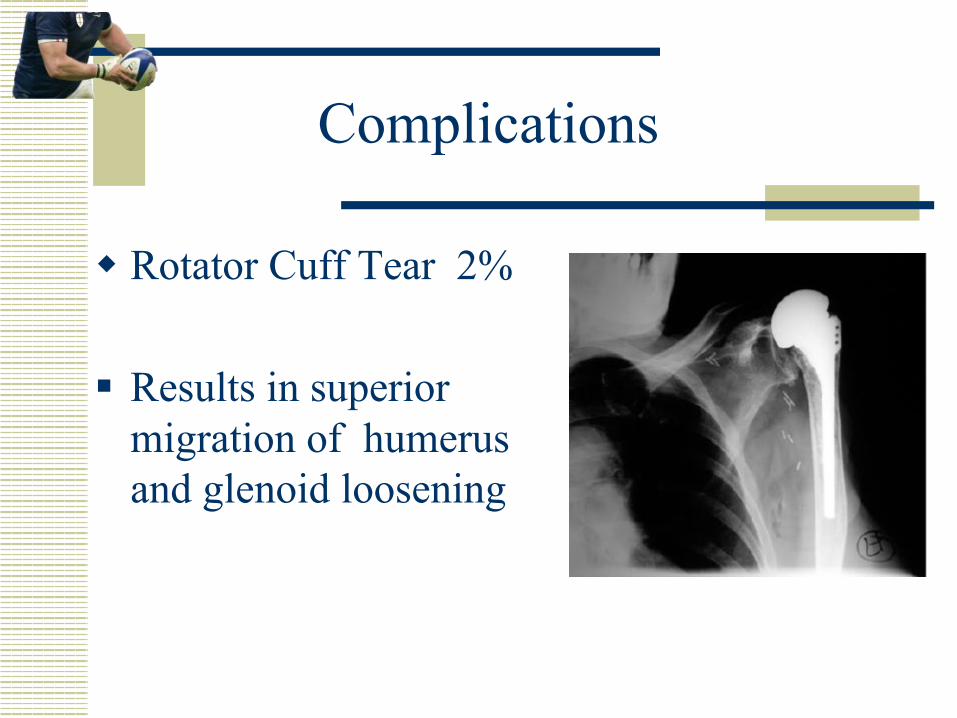
w Rotator Cuff Tear 2%
§ Results in superior migration of humerus and glenoid loosening

Les descellements glénoïdiens sont fréquents (Liseré fréquent après 5 ans mais souvent asymptomatique)
Complications
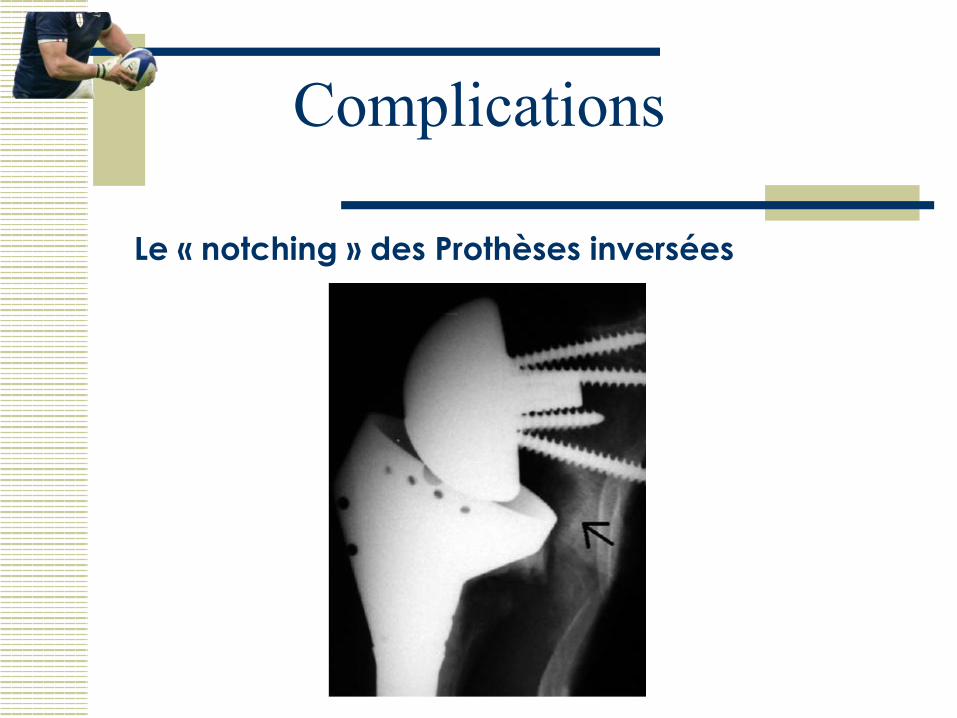
Le « notching » des Prothèses inversées
Complications
Complications
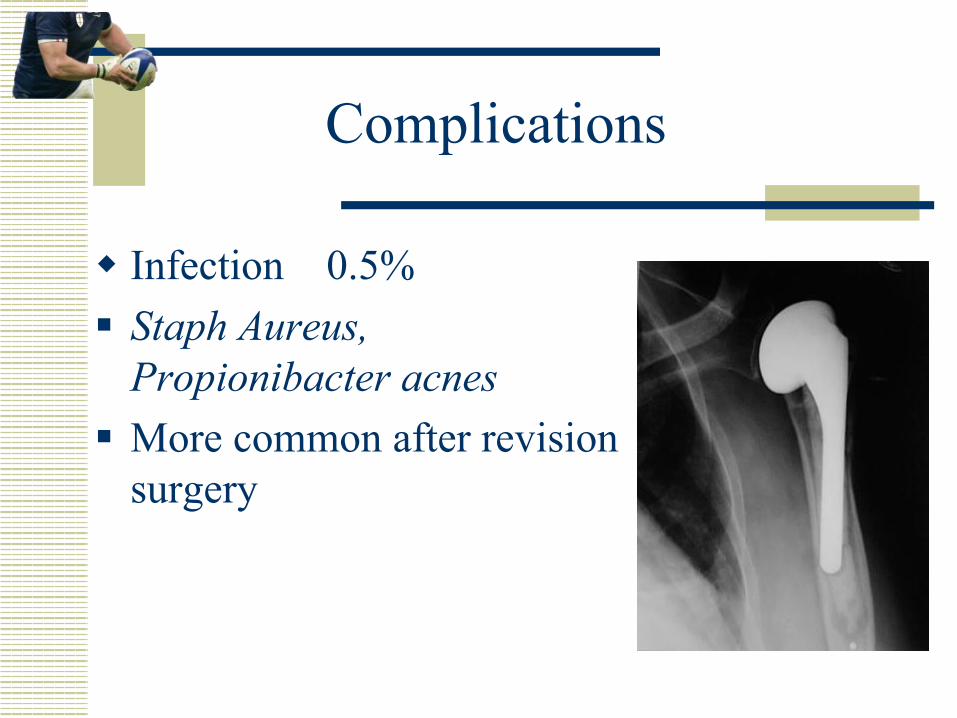
w Infection 0.5% § Staph Aureus,
Propionibacter acnes § More common after revision
surgery
Complications
w Heterotopic Ossification 10 -45% n Males n Dx = osteoarthitis n Low grade n Non-progressive n Does not affect outcome
Sperling, Cofield et al
Complications
w Stiffness n Depends on indication for arthroplasty n Subscap shortening n Oversized components n Inappropriate rehab
Complications
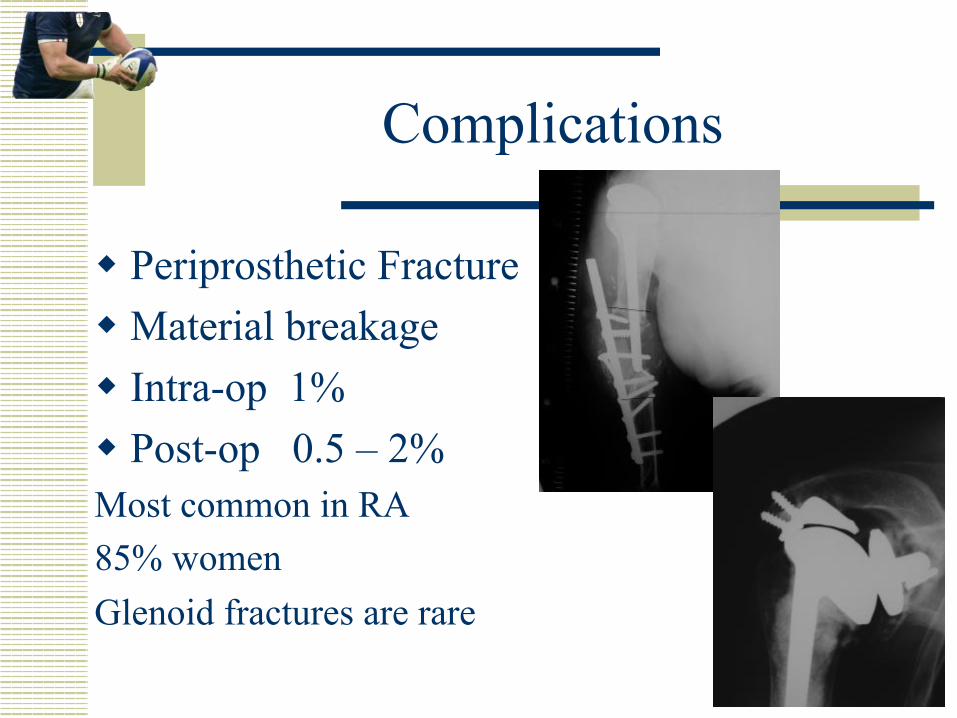
w Periprosthetic Fracture w Material breakage w Intra-op 1% w Post-op 0.5 – 2% Most common in RA 85% women Glenoid fractures are rare
Complications
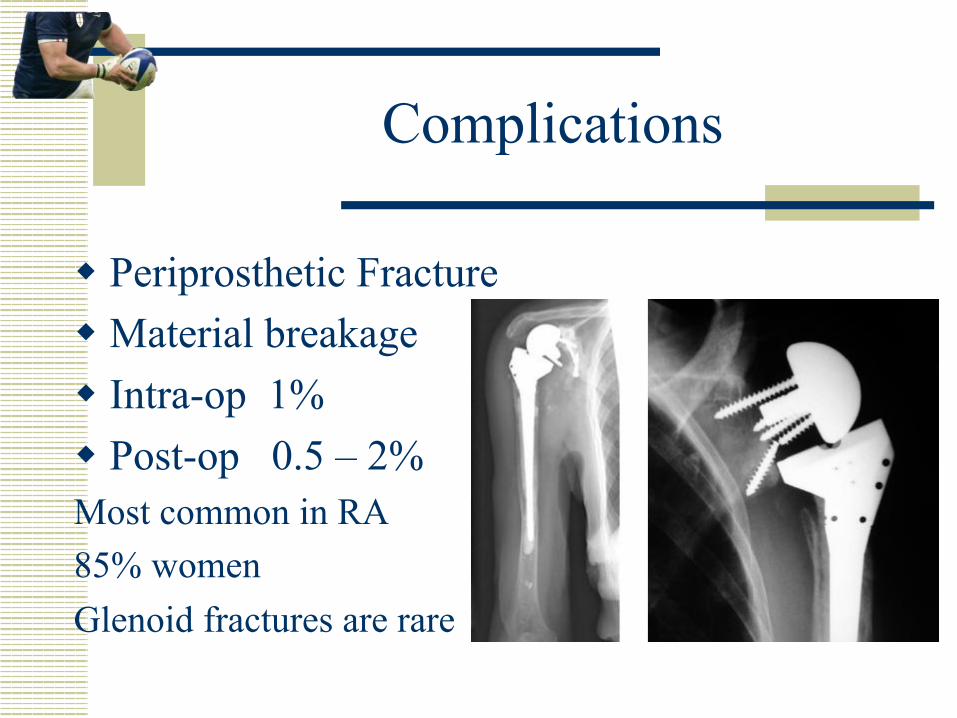
w Periprosthetic Fracture w Material breakage w Intra-op 1% w Post-op 0.5 – 2% Most common in RA 85% women Glenoid fractures are rare
Complications
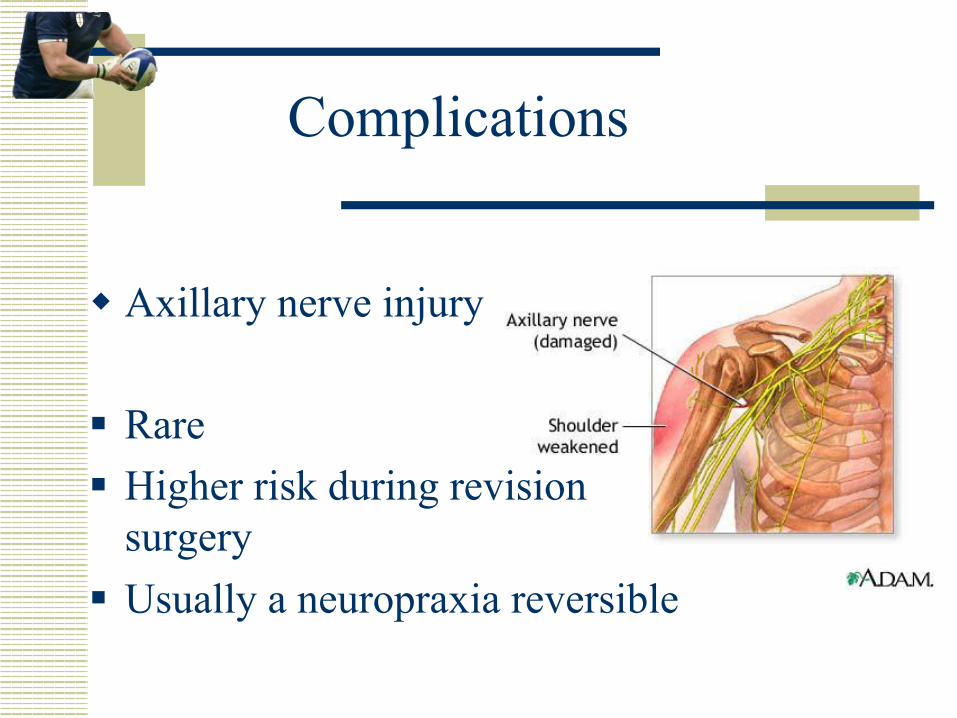
w Axillary nerve injury § Rare § Higher risk during revision
surgery § Usually a neuropraxia reversible
Ultimate Bail -Outs
w Excision Arthroplasty w Reversed arthroplasty w Shoulder Arthrodesis
Conclusion
w Grande modularité dans l’offre prothétique w L’état de la coiffe des rotateurs dicte l’indication et
conditionne le pronostic w Bilan systématique par Arthroscanner ou IRM w Le résultat des d’autant meilleur que l’on a pas tardé
à poser l’indication